Article Text

Statistics from Altmetric.com
Key messages
What is already known about this subject?
18F-fluorodeoxyglucose positron emission/CT (18FDG-PET/CT) is able to detect both synovial and vascular inflammation underlying rheumatoid arthritis (RA).
What does this study add?
This is the very first study where synovial and vascular inflammation were assessed by PET/CT in patients with RA undergoing tofacitinib therapy.
One-year tofacitinib treatment significantly attenuated vascular and synovial inflammations.
Joint and vascular inflammations as determined by PET/CT exerted multiple correlations with autoantibodies, systemic inflammation, lipids, carotid atherosclerosis and arterial stiffness.
How might this impact on clinical practice or further developments?. Please check and provide
13F-FDG-PET/CT may be a suitable technique to determine synovial and vascular inflammation simultaneously and to do follow-up assessments during targeted therapies of RA.
Introduction
Rheumatoid arthritis (RA) has been associated with accelerated atherosclerosis, increased cardiovascular (CV) morbidity and mortality, as well as metabolic changes.1 2 Targeted therapies may have beneficial effects on CV outcomes1 3 4 and metabolism2 5 in RA. Four Janus kinase (JAK) inhibitors including tofacitinib have been approved for RA.6 JAK inhibition has been associated with lipid elevation7; however, it had no CV consequences.1 7
Vascular inflammation may precede atherosclerosis. Traditionally, ultrasound-based techniques have been applied to assess preclinical vascular pathophysiology in RA.1 8 Early endothelial dysfunction indicated by abnormal brachial artery flow-mediated vasodilation (FMD), overt atherosclerosis shown by the presence of carotid plaques and increased common carotid intima–media thickness (IMT), as well as arterial stiffness indicated by increased arterial pulse-wave velocity (PWV) have been reported in association with RA.1 8–11 These preclinical abnormalities predict the development of subsequent CV events in arthritis.1 8 Biologics may, at least transiently, dampen the progression of abnormal FMD, IMT and PWV in RA (reviewed in Szekanecz et al3). There has been only one study showing that tofacitinib decreased carotid atherosclerosis.12
18F-fluorodeoxyglucose-positron emission tomography/CT (18F-FDG-PET/CT) may be able to simultaneously detect tissue inflammation all over the body.13–16 Therefore, this technique may be suitable to assess synovial and vascular inflammation in the very same patient.14 There have been reports on the examination of joints or blood vessel inflammation in RA by positron emission tomography (PET) or PET/CT.17–26 There is increased 18F-fluorodeoxyglucose (FDG) uptake in the arterial wall in RA,24 26 27 as well as ankylosing spondylitis (AS)28 and psoriatic arthritis.29 18F-FDG-PET was able to follow disease activity, joint destruction and predict clinical outcome in patients with RA undergoing combination conventional synthetic disease-modifying antirheumatic drug (csDMARD),30 anti-tumour necrosis factor,17 31–33 rituximab34 or tocilizumab therapy.35 In AS, the effects of statins could be monitored by PET/CT.28 In atherosclerosis, inflammatory variability could be determined by PET/CT over time.20 The composition of atherosclerotic plaques can also be analysed by PET.23 Vascular inflammation could be detected and monitored by PET/CT in large-vessel vasculitis.36–38 There have been rather few studies where synovial and vascular inflammations were simultaneously assessed. In a pilot study performed in patients with psoriasis, skin, joint and subclinical vascular inflammations were detected by FDG-PET/CT.14 In a cross-sectional study of 33 patients with RA, synovial and arterial FDG uptakes correlated with each other.26 In another cross-sectional PET/CT study, vascular inflammation correlated with sacroiliitis.29
To our best knowledge, there have been no prospective studies that simultaneously assess synovial and vascular inflammations by PET/CT in patients with RA over time. Moreover, JAK inhibitors have not yet been included in any PET/CT studies. Therefore, we conducted a 1-year study in order to simultaneously determine the effects of tofacitinib on inflammation of the joints and aorta in relation to vascular and bone status.
Patients and methods
Patients and study design
Thirty patients with active RA were recruited for this study. Patient characteristics are presented in table 1. Inclusion criteria were a definitive diagnosis of RA according to the 2010 EULAR/American College of Rheumatology classification criteria for RA,39 moderate-high disease activity (28-Joint Disease Activity Score (DAS28) >3.2) at baseline and clinical indication of targeted therapy. Patients were either naïve to any targeted therapies (n=16) or initiated tofacitinib after stopping a biologic followed by an appropriate washout period (n=14). Exclusion criteria included inflammatory diseases other than RA, acute/recent infection, standard contraindications to JAK inhibition, uncontrolled CV disease or hypertension, chronic renal or liver failure and malignancy within 10 years.
Patient characteristics
The 30 enrolled patients were randomly assigned in a 1:1 ratio to either 5 or 10 mg tofacitinib two times per day treatment arms. All patients received tofacitinib in combination with either MTX with folic acid (n=23) or leflunomide (n=7). MTX and leflunomide had been taken in stable dose at least 1 year prior to the present study. No dose changes of these disease-modifying antirheumatic drugs were allowed throughout the course of the study. None of the patients had been on corticosteroids for at least 3 months prior to and during the study.
Clinical assessment
Clinical assessments were performed at baseline and after 3, 6 and 12 months of therapy. First, a detailed medical history was taken on history of CV disease, current smoking, hypertension, diabetes mellitus, gout, anxiety, osteoporosis and malignancy by a questionnaire (table 1). This was followed by further clinical assessments including physical examination. The history of concomitant drugs is also included in table 1.
PET/CT assessments
All patients underwent 18F-FDG-PET/CT after at least 6 hours of fasting and serum glucose level check as described previously.40 The accepted prescan glucose level was ≤7.2 mmol/L. Two hours after the intravenous administration of the 18F-FDG radiopharmaceutical (4.4 MBq/kg) (University of Debrecen, Department of Nuclear Medicine, Debrecen, Hungary), whole-body scans were acquired from the skull base to the level of the knees using AnyScan PC (Mediso Medical Imaging Systems, Budapest, Hungary). For interpretation, axial, coronal and sagittal attenuation corrected and non-corrected PET images were reconstructed using low-dose non-enhanced CT images. After visual assessment of the PET and CT images, in order to quantify vascular inflammation, maximum standardised uptake value (SUVmax) and mean standardised uptake value (SUVmean) were determined by two-dimensional circular regions of interest drawn around the external aortic contour and merged into tube-like volumes of interest (VOIs) outlining five predefined aortic segments (ascending aorta, aortic arch, descending thoracic aorta, suprarenal and infrarenal abdominal aorta) using dedicated analysis software (InterView FUSION, Mediso, Budapest, Hungary). The maximum (TBRmax) and mean target-to-background ratios (TBRmean) are the most commonly used parameters for global assessment of vascular inflammation.20 21 41 Aortic TBR-VASCmax and TBR-VASCmean values were calculated by dividing SUV-VASCmax or SUV-VASCmean values of the aortic segments by the SUVmean value of the superior vena cava (blood pool), respectively.13 Thresholds for target-to-background ratio (TBR) have been determined.41 Mean metabolic volumetric product (MVPmean) was computed by multiplying SUVmean by VOI volume (cm3) for each segment as reported in the literature.14 For the quantification of synovial inflammation, SUV-SYNmax and SUV-SYNmean values were determined in VOIs placed with the help of the CT structural images around five predefined articular regions (hand/wrist, elbow, shoulder, hip and knee) on both sides. Liver SUVmean values were determined and used as reference values. TBR-SYNmean values were calculated by dividing SUV-SYNmean values of the joints by the SUVmean value of the liver. Finally, the mean (±SD) of the five TBR-VASCmax and TBR-VASCmean values obtained in the five predefined aortic segments, as well as mean (±SD) of the five SUV-SYNmean and TBR-SYNmean values obtained in the five articular regions were calculated.
Laboratory measurements and assessment of disease activity
Blood samples were drawn from fasting patients in the morning into EDTA-treated tubes and were immediately processed, aliquoted and stored at −70°C until use. Blood samples were taken at baseline, after 6 and 12 months of tofacitinib treatment.
Serum high-sensitivity C reactive protein (normal: ≤5 mg/L) and IgM rheumatoid factor (RF, normal: ≤50 IU/mL) were measured by quantitative nephelometry (Cobas Mira Plus; Roche Diagnostics, Basel, Switzerland), using C reactive protein (CRP) and RF reagents (both Dialab, Budapest, Hungary). anticitrullinated protein antibody (aCCP (cyclic citrullinated peptide)) autoantibodies were detected in serum samples using a second generation Immunoscan-RA CCP2 ELISA test (Euro Diagnostica, Malmö, Sweden; normal:≤25 IU/mL). The assay was performed according to the manufacturer’s instructions.
Disease activity of RA was calculated as DAS28-CRP (three variables). Health Assessment Questionnaire (HAQ) was also evaluated in order to determine the functional status of the patients.
Serum levels of lipids including total cholesterol (TC), low-density lipoprotein cholesterol (LDL-C), high-density lipoprotein cholesterol (HDL-C), triglyceride (TG) and lipoprotein A (Lp(a)) were determined in fresh sera using a Cobas c501 autoanalyser (Roche, Mannheim, Germany) in the Department of Laboratory Medicine of our university.
Among biomarkers of bone metabolism, serum parathyroid hormone, 25-hydroxy-vitamin D3, osteocalcin (OC), procollagen 1 N-terminal propeptide (P1NP), C-terminal collagen crosslinks (CTX), sclerostin, cathepsin K, osteoprotegerin, soluble receptor activator nuclear factor κB ligand (RANKL) and Dickkopf-1 were determined as described before in more detail.42 All measurements were performed at baseline, as well as 6 and 12 months after treatment initiation. Bone studies carried out in the very same tofacitinib cohort have been performed and published in detail previously.42 Here we used those bone biomarker results in order to correlate PET/CT data with bone metabolism.
Assessment of vascular physiology
FMD, IMT and PWV assessments were carried out as published previously.43 Vascular pathophysiology studies carried out in this very same tofacitinib cohort have been performed previously.44 Evaluation was performed at baseline and after 12 months of tofacitinib treatment. Here we used those results in order to correlate PET/CT data with vascular pathophysiology.
Assessment of bone mineral density (BMD)
Areal BMD was determined by dual-energy X-ray absorptiometry (DXA) as described previously in more detail.42 45 Bone studies carried out in the very same tofacitinib cohort have been performed and published in detail previously.42 Evaluation was performed at baseline and after 12 months of tofacitinib treatment. Here we used those results in order to correlate PET/CT data with bone status.
Statistical analysis
Statistical analysis was performed using the SPSS software V.22.0 (IBM, Armonk, NY, USA). Data are expressed as mean±SD for continuous variables and percentages for categorical variables. The distribution of continuous variables was determined by Kolmogorov-Smirnov test. Continuous variables were assessed by paired two-tailed t and Wilcoxon tests. Nominal variables were compared by χ2 or Fisher’s exact test. Pearson’s analysis was used to test for correlations. Univariable and multivariable regression analyses using the enter and stepwise methods, respectively, were applied to determine independent associations between PET/CT (dependent variables) and other (clinical, inflammatory, vascular and bone) parameters (independent variables). β standardised linear coefficients were calculated for indicating linear correlations between two parameters. The B (+95% CI) regression coefficient indicated independent associations between dependent and independent variables during changes. General linear model multivariate analysis of variance (MANOVA) was performed to determine effects of any independent variable on two concurrent dependent variables. Repeated measures analysis of variance (RM-ANOVA) was performed to evaluate the effects of multiple parameters on 12-month changes of PET/CT parameters. In RM-ANOVA, partial η2 is an indicator of effect size. Values of 0.01 suggest small, 0.06 medium and 0.14 large effects. The reliability of the vascular ultrasound measurements was tested by interitem correlation and intraclass correlation (ICC). Regarding the FMD, IMT and PWV tests, ICC=0.470; F-test value: 1.887; p=0.001. A p value of <0.05 was considered significant in all tests mentioned previously. In this study, because of the patient numbers, we pooled the 5 and 10 mg two times per day arms during data analysis.
Results
Characteristics of patients and clinical response to tofacitinib
Table 1 indicates relevant data of the 30 patients included in the study at baseline. Six patients (three–three on each arm) had a positive CV history. A total of 14 patients had hypertension; 2 had diabetes mellitus; and 7 had been current smokers at the time of inclusion (table 1). Eventually, a total of four patients, two–two on each treatment arms, dropped out after 6 months of treatment. Two had inefficacy; one had elevated transaminases; and one moved abroad. Thus, 13–13 patients on each arm were eligible for further data analysis.
The clinical response to tofacitinib treatment in this cohort has been assessed before.42 44 In brief, both 5 mg two times per day and 10 mg two times per day tofacitinib significantly decreased DAS28 and CRP after 6 and 12 months compared with baseline (p<0.005) (data not shown).42 44
Effects of tofacitinib on vascular and bone status
The effects of 1-year tofacitinib treatment on IMT, FMD and PWV in the very same cohort have been investigated previously.44 In brief, carotid IMT significantly increased after 12 months compared with baseline in the 5 mg two times per day subset, while in the 10 mg two times per day subset, there were no differences in IMT over time. In addition, neither FMD nor PWV showed any significant changes over time (data not shown).44
Also the effects of tofacitinib treatment on BMD as determined by DXA and bone biomarkers in the same cohort have also been reported.42 In brief, tofacitinib attenuated further bone loss in RA. Moreover, it stabilised bone turnover as indicated by bone biomarkers (data not shown).42
Changes in synovial and vascular inflammation on tofacitinib therapy as determined by PET-CT
One-year tofacitinib treatment simultaneously and significantly attenuated synovial (figure 1) and vascular inflammation (figure 2) as visualised by PET/CT. Articular SUV-SYNmean significantly decreased from 3.18±1.13 at baseline to 2.55±0.50 after 12 months (p=0.010) (figure 3A). Similarly, TBR-SYNmean decreased from 1.53±0.54 to 1.12±0.22 over time (p=0.001) (figure 3B). Aortic TBR-VASCmax significantly decreased from 2.17±0.52 at baseline to 1.80±0.30 after 12 months (p<0.001) (figure 3C). TBR-VASCmean showed only a non-significant tendency of decrease overtime (baseline: 1.29±0.29, 12 month: 1.20±0.20) (p=0.170) (figure 3D).
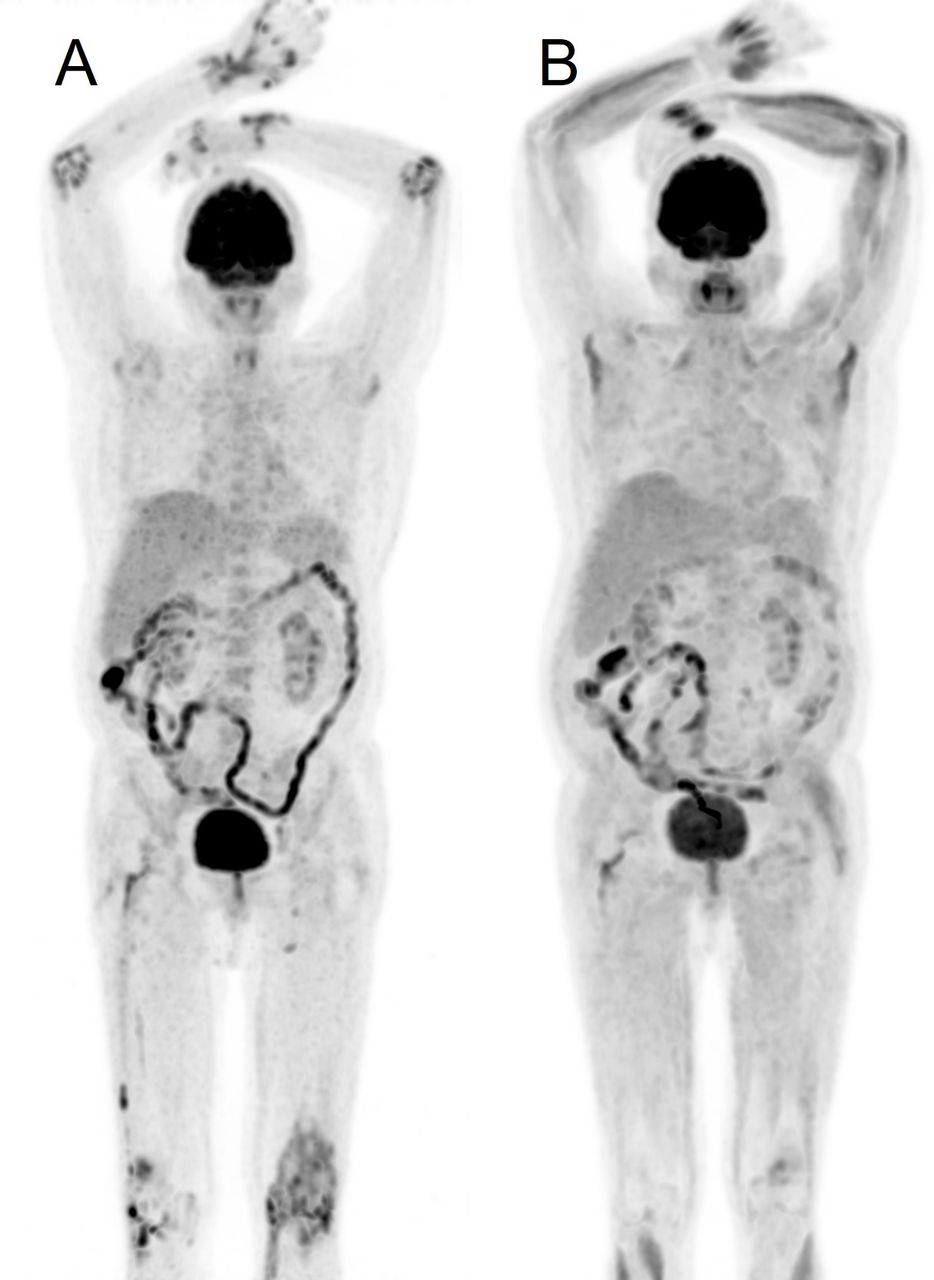
Representative image of joint inflammation visualised by 18F-fluorodeoxyglucose-PET/CT at baseline and after tofacitinib treatment in a patient with RA. (A) Baseline PET/CT MIP image demonstrates intense synovial activity in multiple joints, including wrists, small hand joints, elbows and knees bilaterally. (A) Baseline PET/CT MIP image demonstrates intense synovial activity in multiple joints including wrists, small hand joints, elbows and knees bilaterally. (B) There is marked reduction of FDG uptake after 12 months of treatment. FDG, 18F-fluorodeoxyglucose; MIP, multiple intensity projection; PET, positron emission tomography; RA, rheumatoid arthritis.
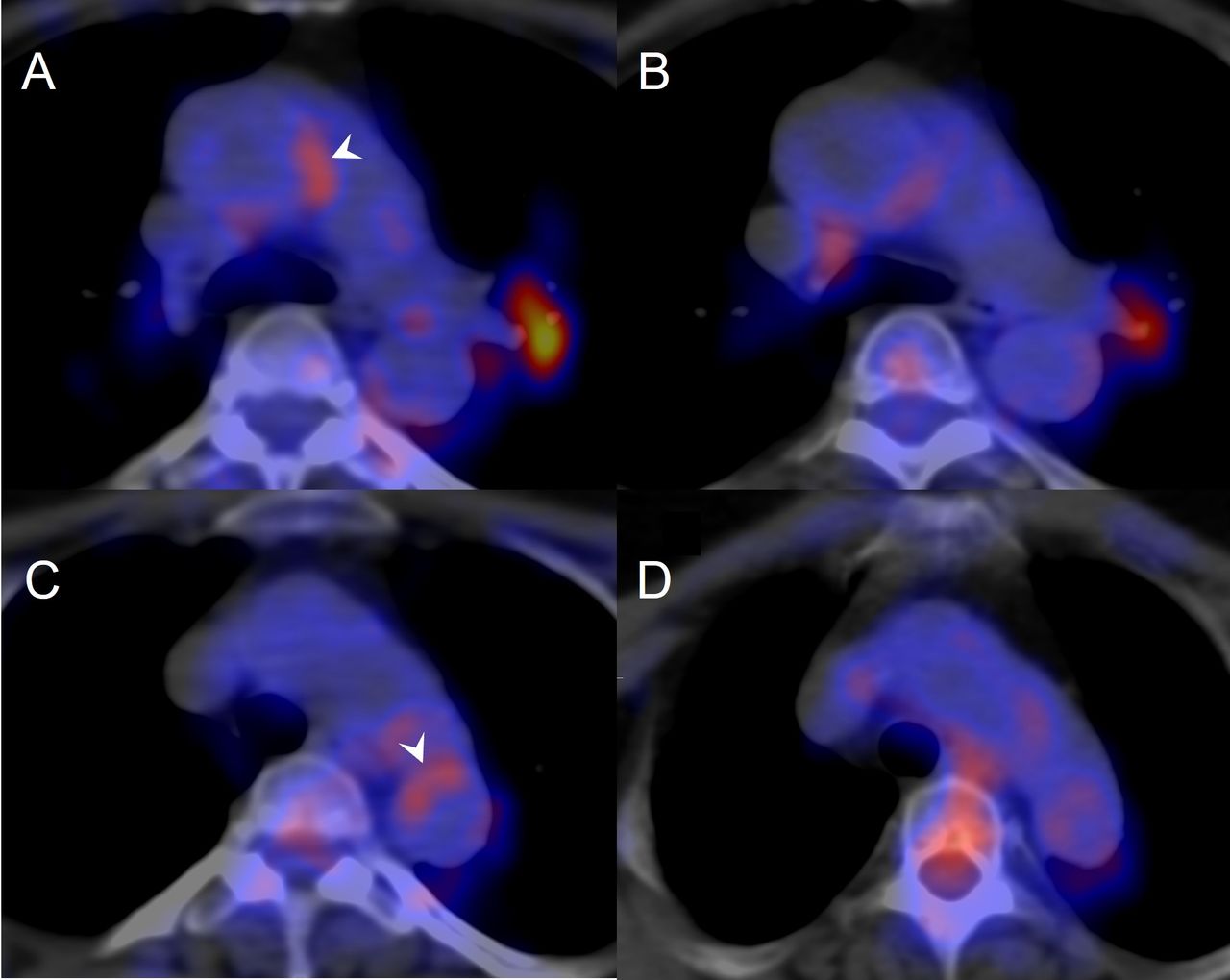
Representative image of vascular inflammation visualised by 18F-FDP-PET/CT at baseline and after tofacitinib treatment in a patientaseline (C) ost-treatment (D)

{kind=link}
{kind=link}
{kind=link}
Effects of 1-year tofacitinib therapy on articular SUV-SYNmean (A), TBR-SYNmean (B), aortic TBR-VASCmean (C) and TBR-VASCmax (D) as determined by 18F-FDG-PET/CT. *P<0.05. 18F-FDG-PET/CT, 18F-fluorodeoxyglucose-positron emission tomography/CT; SUV, standardised uptake value; SYN, synovial; TBR, target-to-background ratio; VASC, vascular.
Correlations of synovial and vascular inflammation with each other and with other parameters
We did not find any significant correlations between articular SUV/TBR and aortic TBR values (data not shown).
When correlating articular SUV-SYNmean and TBR-SYNmean values at baseline or after 12 months of treatment with other parameters, synovial inflammation as determined by PET/CT positively and significantly correlated with CRP, anti-CCP, RF, Lp(a), PWV, IMT, RANKL, CTX, as well as DXA L2-4 BMD (p<0.05) (online supplemental table 1). Similarly, aortic TBR-VASCmean and TBR-VASCmax values at baseline and after 12 months variably, positively correlated with DAS28, erythrocyte sedimentation rate (ESR), PWV, OC, P1NP and negatively with HAQ, as well as DXA L2-4 BMD (p<0.05) (online supplemental table 1).
Supplemental material
Some of these simple correlations were confirmed by univariable and multivariable regression analyses. In the univariable analysis, synovial inflammation as determined by PET/CT after 12 months of tofacitinib treatment was positively associated with CRP, Lp(a), PWV, IMT, CTX and negatively with DXA L2-4 BMD (p<0.05) (table 2). Aortic inflammation was associated with DAS28, PWV, OC and P1NP and inversely associated with HAQ (table 2). In the multivariable analysis, further conformation was obtained for synovial inflammation and Lp(a) after 12 months, as well as for vascular inflammation and DAS28, P1NP and HAQ at various time points (p<0.05) (table 2).
Univariable and multivariable regression analyses of the associations between PET/CT as dependent variables and other parameters as independent variables
As synovial and vascular inflammation as determined by PET/CT did not correlate with each other, we wished to look for associations of synovial inflammation (PET/CT) and vascular pathophysiology (ultrasound) as covariates with markers of disease activity and systemic inflammation as independent variables. In the MANOVA model, DAS28, ESR and CRP variably and significantly determined both synovial inflammation and FMD or PWV after 12 months (p<0.05) (table 3).
Significant results of general linear model multivariate analysis of variance test determining the effects of inflammatory markers as independent variables on 12-month positron emission tomography/CT and vascular pathophysiology parameters as concurrent dependent variables
Finally, RM-ANOVA analysis was performed to analyse the combined effects of tofacitinib treatment and other parameters on 1-year changes in PET/CT parameters over time. Treatment together with higher baseline RANKL levels significantly determined 12-month articular SUV-SYNmean and TBR-SYNmean changes (p<0.05) (table 4). Similarly, treatment along with higher ESR or lower DXA lumbar 2–4 vertebrae BMD indicated more pronounced 12-month changes in TBR-VASCmean and TBR-VASCmax (p<0.05) (table 4).
Significant results of general linear model repeated measures analysis of variance test determining the effects of treatment and other independent variables on 1-year changes in positron emission tomography/CT parameters as dependent variables
Discussion
To our best knowledge, this may be the first prospective study on assessing joints and vessels simultaneously by PET/CT in RA. Furthermore, tofacitinib has not yet been investigated in any PET/CT studies. Therefore, it is rather difficult to compare our data with others. This study focuses on the effects of JAK inhibition on synovial and vascular inflammation (PET/CT); however, we also correlated these results with those obtained from previous studies conducted in the very same cohort on vascular pathophysiology44 and bone status.42 Thus, we used these vascular and bone data published before during the data analysis of the 26 patients who completed the study.42 44
One-year tofacitinib treatment effectively suppressed disease activity and synovial inflammation (ESR and CRP). In parallel, JAK inhibition significantly attenuated mean synovial (SUV-SYNmean and TBR-SYNmean) and maximum aortic inflammation (TBR-VASCmax) as determined in five predefined articular and five aortic regions. With respect to RA synovitis, in multiple RA trials, 18F-FDG-PET or PET/CT was able to detect inflammation and associate FDG uptake with clinical disease activity, especially in large joints.17–19 25 In one study, baseline SUVmax before therapy correlated with subsequent large joint damage.33 Moreover, some investigators followed changes in synovial inflammation, clinical efficacy and outcome in patients with RA undergoing either csDMARD30 or biologic DMARD.31–35 In atherosclerosis, the evaluation of TBR was suitable to detect vessel wall inflammation20 24 and the composition of plaques.20 21 23 In RA, Agca et al24 found increased arterial wall inflammation.
When simultaneously assessing synovial and vascular inflammation by PET/CT, there were no correlations between articular SUV and aortic TBR values. In a pilot study carried out in six patients with psoriasis, Mehta et al14 described inflammation in the skin, joints and vessel walls by PET/CT; however, correlation analysis was not performed. Emami et al26 performed a cross-sectional study in patients with RA. In that study, synovial and arterial FDG uptake correlated with each other.26 However, they did not find any correlations between CRP and synovial or arterial FDG uptake.26 Rose et al29 found correlation between sacroiliitis and vascular inflammation by PET/CT. As we did find correlations of PET/CT parameters in the joint and aorta with markers of inflammation (CRP and ESR) and disease activity (DAS28), it is possible that the composition of our cohort and that of Emami et al26 differed. Although we have not found any associations between synovial and aortic PET/CT parameters, we found multiple correlations between PET/CT parameters and vascular pathophysiology as determined by ultrasound. Synovial inflammation by PET/CT exerted various positive correlations with PWV and IMT. Disease activity and ESR variably correlated with aortic inflammation by PET/CT. Moreover, in the MANOVA analysis, RA disease activity and acute phase reactants determined synovial inflammation and FMD or PWV together. Finally, aortic inflammation by PET/CT also correlated PWV. Thus, systemic inflammation may drive synovitis, vascular inflammation and vascular pathophysiology. Indeed, disease activity, as well as CRP and ESR are important drivers of vascular pathology in RA.1 8 46
Synovial and aortic inflammation determined by PET/CT also correlated with bone turnover and BMD, as well as with systemic inflammation, disease activity and vascular pathophysiology described previously. Suto et al33 found that synovial SUVmax predicted joint destruction. We found that synovial and vascular inflammation by PET/CT were associated not only with localised bone resorption but also with generalised osteoporosis. In our PET/CT study, synovial inflammation correlated with RANKL and CTX, markers of bone resorption, while aortic inflammation rather correlated with OC and P1NP, indicators of bone formation. Moreover, in the RM-ANOVA analysis, treatment together with higher baseline RANKL determined 1-year changes in SUV-SYNmean and TBR-SYNmean over time. Finally, lumbar spine BMD values were inversely associated with both synovial SUV/TBR and aortic TBR values. Again, systemic inflammation may drive bone loss, as well as synovial and vascular inflammations in RA.1 42 46–48 In the very same cohort, we also found that bone biomarkers and BMD were associated with CRP and DAS28 in tofacitinib-treated patients with RA.42 Moreover, there may be direct links between bone loss and atherosclerosis, which are further aggravated by arthritis (reviewed in Szekanecz et al47).
In this study, lipids and Lp(a) were also tested in relation to PET/CT parameters. In general, we did not find any notable associations between lipids (TC, LDL-C, HDL-C and TG) and either synovial or aortic inflammation. On the other hand, Lp(a) significantly correlated with FDG uptake in the synovium but not in the aortic wall. Lp(a) has been implicated in RA and in CV disease associated with RA.9 49–51 We have previously found correlations of Lp(a) with CRP in RA.9 Biologics are able to decrease Lp(a) production in RA.50 51
Our study has certain advantages and limitations. To our knowledge, this is the first study that longitudinally and simultaneously assesses the effects of tofacitinib on synovial and aortic inflammations by 18F-FDG-PET/CT. This is also a complex study evaluating PET/CT parameters in association with markers of inflammation, bone turnover, BMD and vascular pathophysiology. The possible limitations of this study include the relatively low number of patients. However, we assessed PET/CT parameters, as well as a great number of biomarkers in a prospective manner, which would have been more difficult in a larger patient cohort. We also did not have a control group as this is a self-controlled, therapeutic, follow-up study where later time points were compared with baseline.
Conclusions
In summary, tofacitinib therapy simultaneously attenuated synovial and vascular inflammation as determined by PET/CT. CRP, Lp(a), PWV, IMT, RANKL and CTX may be independent predictors of synovial inflammation. On the other hand, DAS28, ESR, HAQ, PWV, OC and P1NP determined aortic FDG uptake. Systemic inflammation and disease activity may drive both synovial inflammation and vascular pathophysiology. Thus, 18F-FDG-PET/CT may indeed be suitable to assess synovitis and aortic inflammation in parallel and to follow the effects of antirheumatic and other therapies on tissue inflammatory processes. Further studies are needed to evaluate the potential beneficial effects of tofacitinib and other JAK inhibitors on joint and vascular inflammation in arthritis.
Data availability statement
Data are available upon reasonable request. Data may be available upon reasonable request from the authors.
Ethics statements
Patient consent for publication
Ethics approval
The study was approved by the Hungarian Scientific Research Council Ethical Committee (approval number 56953-0/2015-EKL). Written informed consent was obtained from each patient, and assessments were carried out according to the Declaration of Helsinki and its amendments.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors AH: study concept, patient recruitment, data analysis and manuscript drafting. ZH: performance of positron emission tomography/CT assessments, data generation and analysis. AP and MC: performance of lab analysis and data analysis. EV, ZP, GK, BS, ÉS, SSzá and GS: patient recruitment and examination, and data generation. KG: performance of flow-mediated vasodilation, intima–media thickness and pulse-wave velocity assessments. KH: statistical analysis and result interpretation. TS: study concept, data analysis and manuscript drafting. ZS: senior investigator and supervisor, study concept, manuscript drafting and finalisation, and guarantor. SSza: senior investigator and supervisor, patient recruitment and manuscript drafting.
Funding This research was supported by the European Union and the State of Hungary and cofinanced by the European Social Fund in the framework of TAMOP-4.2.4.A/2-11/1-2012-0001 ‘National Excellence Program’ (ZS); by the European Union (grant GINOP-2.3.2-15-2016-00050, ZS) and by the Pfizer Investigator Initiated Research (grant number WI188341, ZS). This work was presented as a conference abstract at the EULAR congress in 2021.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.