Article Text

Abstract
Introduction Several risk factors for severe COVID-19 specific for patients with inflammatory rheumatic and musculoskeletal diseases (RMDs) have been identified so far. Evidence regarding the influence of different RMD treatments on outcomes of SARS-CoV-2 infection is still poor.
Methods Data from the German COVID-19-RMD registry collected between 30 March 2020 and 9 April 2021 were analysed. Ordinal outcome of COVID-19 severity was defined: (1) not hospitalised, (2) hospitalised/not invasively ventilated and (3) invasively ventilated/deceased. Independent associations between demographic and disease features and outcome of COVID-19 were estimated by multivariable ordinal logistic regression using proportional odds model.
Results 2274 patients were included. 83 (3.6%) patients died. Age, male sex, cardiovascular disease, hypertension, chronic lung diseases and chronic kidney disease were independently associated with worse outcome of SARS-CoV-2 infection. Compared with rheumatoid arthritis, patients with psoriatic arthritis showed a better outcome. Disease activity and glucocorticoids were associated with worse outcome. Compared with methotrexate (MTX), TNF inhibitors (TNFi) showed a significant association with better outcome of SARS-CoV-2 infection (OR 0.6, 95% CI0.4 to 0.9). Immunosuppressants (mycophenolate mofetil, azathioprine, cyclophosphamide and ciclosporin) (OR 2.2, 95% CI 1.3 to 3.9), Janus kinase inhibitor (JAKi) (OR 1.8, 95% CI 1.1 to 2.7) and rituximab (OR 5.4, 95% CI 3.3 to 8.8) were independently associated with worse outcome.
Conclusion General risk factors for severity of COVID-19 play a similar role in patients with RMDs as in the normal population. Influence of disease activity on COVID-19 outcome is of great importance as patients with high disease activity—even without glucocorticoids—have a worse outcome. Patients on TNFi show a better outcome of SARS-CoV-2 infection than patients on MTX. Immunosuppressants, rituximab and JAKi are associated with more severe course.
- COVID-19
- antirheumatic agents
- glucocorticoids
Data availability statement
Data are available upon reasonable request. Applications to access the data should be made to the COVID-19 steering committee of the German Society for Rheumatology.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Also in rheumatic and musculoskeletal diseases (RMDs) age, male sex and specific comorbidities are general risk factors for severity of SARS-CoV-2 infection.
RMD disease activity and glucocorticoids are specific risk factors.
What does this study add?
RMD treatment is associated with SARS-CoV-2 infection severity.
While patients under TNFi treatment show better outcome, those under immunosuppressants, Janus kinase inhibitor (JAKi) and rituximab show worse outcome.
How might this impact on clinical practice or further developments?
Patients with RMD under treatment with immunosuppressants, JAKi and rituximab need special guidance during the pandemic.
Introduction
Since the beginning of the SARS-CoV-2 pandemic, increasing evidence about COVID-19 in inflammatory rheumatic and musculoskeletal diseases (RMDs) has been gained. In the general population, age, male sex and certain chronic diseases such as cardiovascular disease (CVD) have been identified as risk factors for severity of COVID-19.1 2 In patients with RMD, similar risk factors have been described. In addition, for those patients also RMD-specific risk factors play a role.3–6 Disease activity of the underlying RMD, for example, is of utmost importance for the outcome of COVID-19.4 6
Since immunomodulatory treatment can influence the outcome of infectious diseases significantly, the impact of the RMD treatment is also of great interest for patients with RMD suffering from SARS-CoV-2 infection. On the one hand, certain immunomodulatory drugs have been proven beneficial in the course of a SARS-CoV-2 infection7; on the other hand, immunomodulatory drugs can be detrimental.8 Moreover, timing and dosing of the treatment appears to be crucial. For example, dexamethasone is a standard treatment for severe COVID-197 at present, but a long-term glucocorticoid treatment due to RMD is associated with a worse outcome of SARS-CoV-2 infection.4 6 The same might be true for Janus kinase inhibitor (JAKi) treatment.9
The impact of TNFi on SARS-CoV-2 infection is not completely understood. Use of TNFi in comparison to ‘no disease-modifying anti-rheumatic drug (DMARD)’ was associated with a lower risk of hospitalisation in the first analysis of the data from the Global Rheumatology Alliance (GRA).3 However, it was not significantly associated with lower risk of mortality in a more recent analysis of the GRA in which MTX was used as reference category.4 Potential beneficial effects of TNFi have also been described in patients with COVID-19 with inflammatory bowel disease.10
Due to the lack of interventional studies in patients with RMDs and SARS-CoV-2 infection, the effects of RMD treatment have been evaluated in observational studies only. In this analysis from the German COVID19-RMD registry, we analysed the risk factors for the severity of SARS-CoV-2 infection in patients with RMD, specifically focusing on the impact of RMD treatment.
Methods
Data source
The German COVID-19 registry for patients with RMDs was founded in March 2020 by the German Society for Rheumatology, together with the Justus-Liebig-University Giessen. Rheumatologists voluntarily entered the data into a web-based registry with implemented plausibility checks (https://www.covid19-rheuma.de; for more details, see Hasseli et al11).
SARS-CoV-2 infection outcome parameters
The primary outcome of interest was the mutually exclusive ordinal COVID-19 severity outcome:
(1) neither hospitalised, ventilated nor deceased; (2) hospitalised with or without non-invasive ventilation, but neither invasively ventilated nor deceased; and (3) invasively ventilated or deceased. At the time of analysis, all patients were required to have a resolved clinical course.
Statistical analyses
Patient characteristics are shown descriptively, stratified by the three categories of the ordinal outcome. Independent associations between demographic and disease features and the ordinal COVID-19 outcome were estimated by multivariable ordinal logistic regression using the proportional odds model and were reported as OR and 95% CI. In the proportional odds model, an increase in severity is assumed to be equal across categories: the increase from ‘neither hospitalised, ventilated nor deceased’ to ‘hospitalised with or without non-invasive ventilation, but neither invasively ventilated nor deceased’ is treated in the same way as the increase from the latter category to ‘invasively ventilated or deceased’. Potential deviations from this assumption were assessed graphically and did not show relevant deviation (data not shown). Covariates included in the model were age, sex, key comorbidities (hypertension alone or CVD alone, hypertension combined with CVD, chronic lung disease, chronic kidney disease (CKD) and diabetes), RMD or diagnostic group, rheumatic disease treatment prior to COVID-19 diagnosis (without glucocorticoids), as well as the combined status of disease activity as per the physician’s global assessment (severe/high or moderate disease activity vs minimal/low disease activity or remission), and the prednisolone-equivalent glucocorticoid use (1–10 mg/day and >10 mg/day). The combined status of disease activity and glucocorticoid use represents both their main effects and interaction (in an additive sense) and is analysed to disentangle the effects of both factors.
All patients with confirmed SARS-CoV-2 infection were included in the main analyses. Patients with missing primary outcome (n=2) or missing values for age, sex and DMARDs (n=2) were excluded from analysis. Smoking status was missing in many cases. Therefore, we have not included smoking in the analysis. Missing values for glucocorticoid therapy and disease activity were derived by multiple imputation using full conditional specification.12 Results of the ordinal logistic regression analyses for 10 imputed data sets were pooled by Rubin’s rules.
For patients listed as having more than one RMD or being treated with more than one of the medications of interest, we created a hierarchy based on clinical expertise to categorise patients. We used the same hierarchy as in Strangfeld et al.4 This process produces disjoint categories, allowing a clear reference group for interpretation of the regression models and avoiding collinearities. Patients with more than one of the following diseases were grouped according to the following hierarchy: systemic lupus erythematosus >vasculitis>other CTD >rheumatoid arthritis (RA) >psoriatic arthritis (PsA)>(other) spondyloarthritis (SpA) >other non-inflammatory joint diseases (IJDs)/non-CTD rheumatic disease; where ‘X>Y’ means that disease X has priority over disease Y and an individual who has both disease X and disease Y is counted as patient with disease X. Similarly, patients receiving multiple csDMARDs or immunosuppressants (except glucocorticoids) were grouped according to the following hierarchy: immunosuppressants>sulfasalazine>antimalarials>leflunomide>methotrexate. Patients receiving a bDMARD/tsDMARD alone or in combination were considered solely in the bDMARD/tsDMARD group. Patients with an IJD other than RA, PsA or SpA (n=6); patients treated with more than one bDMARD/tsDMARD (n=1); and patients receiving interleukin-1 inhibitors (n=27) or belimumab (n=11) were excluded from analysis due to low numbers.
Regression coefficients were considered statistically significant for p values <0.05. All analyses were conducted in SAS V.9.4 or R V.4.0.4.
Results
Patient characteristics
Baseline characteristics of the patients are shown in table 1. Of the 2274 patients included, 1771 (78%) did not require hospitalisation. Eighty-three patients died, resulting in a case fatality rate of 3.6%.
Patient characteristics
The mean age of all patients was 57 years; 67% were female. The most common RMD was RA with 46%, followed by PsA (14%), SpA (13%) and vasculitides (11%).
Eighty-six per cent of patients had a PCR-confirmed diagnosis of SARS-CoV-2 infection; 8% had only an antibody-confirmed diagnosis; the remaining patients had an unknown/other type of diagnosis (two patients were diagnosed based on symptoms only). For all patients, the outcome of SARS-CoV-2 infection was known.
RMD treatments
At the time of SARS-CoV-2 infection, 18% did not receive any DMARD treatment (see table 1). Immunosuppressants (mycophenolate mofetil, azathioprine, cyclophosphamide and ciclosporin) were used in 5%, csDMARDs in 35%, bDMARDs in 35% and tsDMARDs in 7%. Methotrexate was the most common csDMARD, and TNFi was the most common bDMARD. Rituximab was used in 91 patients (4%), and JAKi was used in 147 patients (6.5%).
SARS-CoV-2 infection outcome analysis
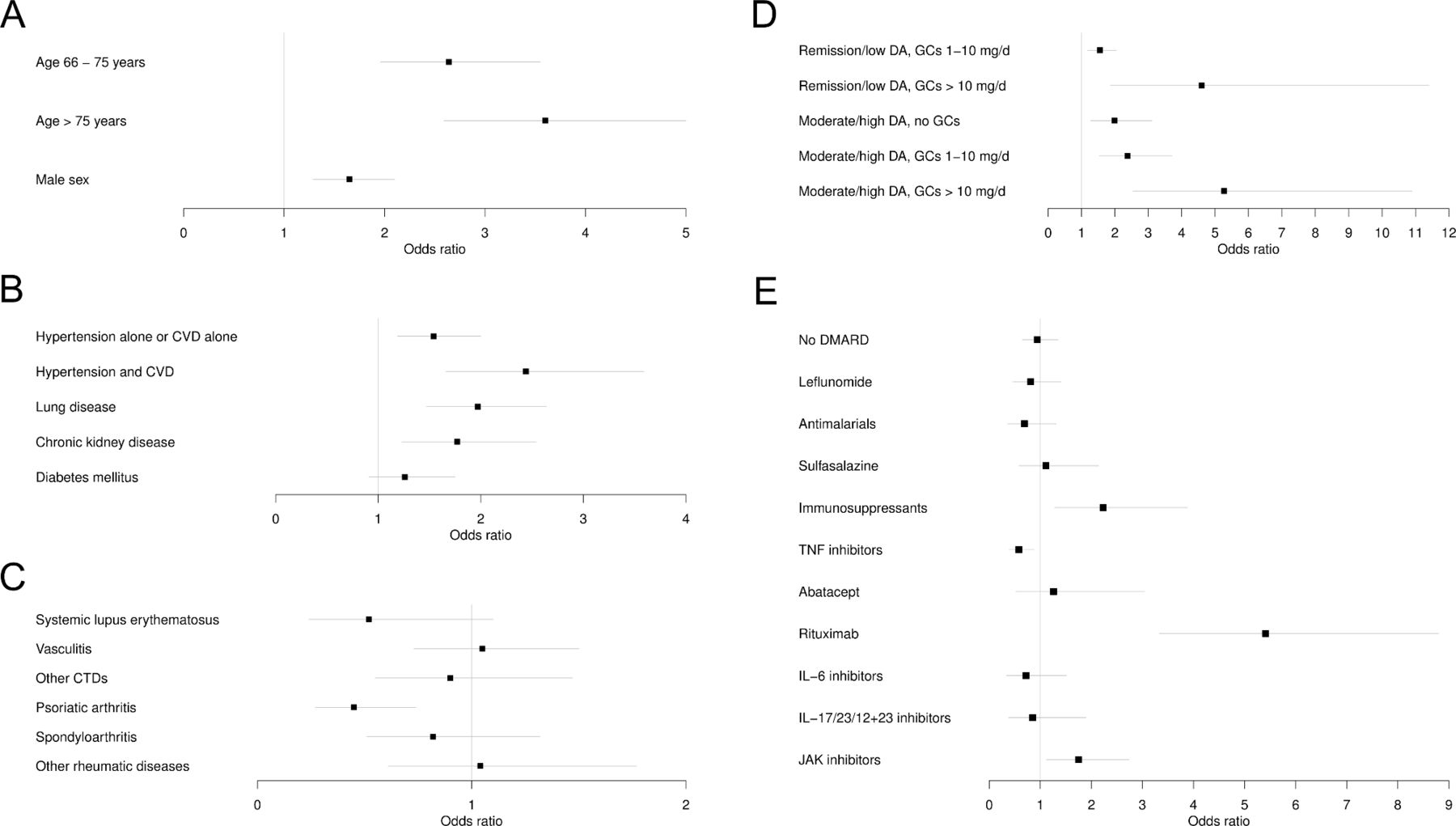
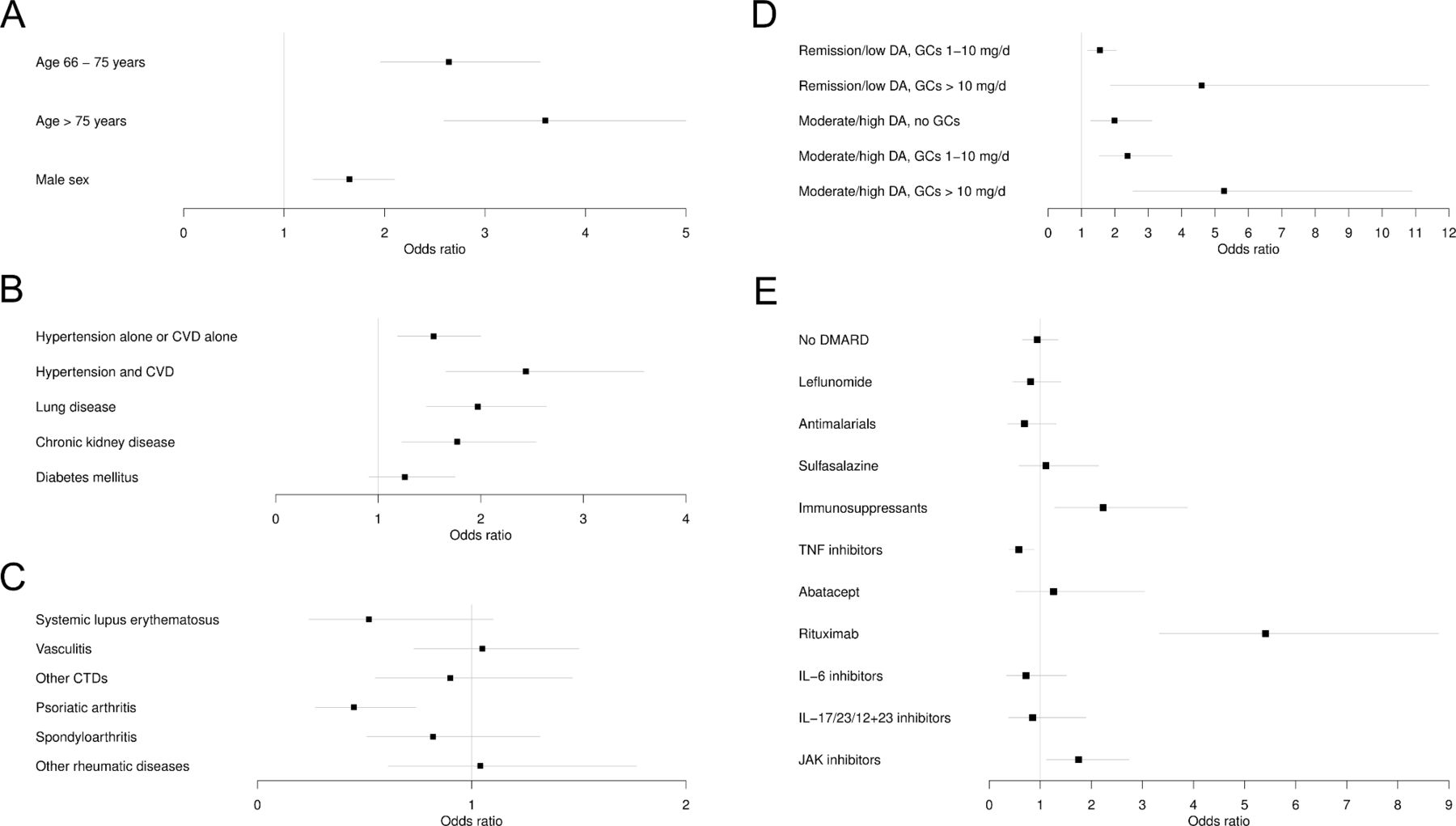
Age above 65 years was associated with higher COVID-19 severity with an OR of 2.6 (95% CI 2.0 to 3.6) and above 75 years with an OR of 3.6 (95% CI 3.0 to 5.0) (table 2 and figure 1A). Male sex was also associated with greater severity (OR 1.7, 95% CI 1.3 to 2.1).
{kind=link}
(A–E) Results of the multivariable ordinal logistic regression using the proportional odds model and reported as OR and 95% CI for each regressor variable. Associations with SARS-CoV-2 infection severity are shown with (A) general factors, (B) comorbidities, (C) RMD diagnosis, (D) RMD disease activity and glucocorticoids, (E) RMD treatment (immunosuppressants: mycophenolate mofetil, azathioprine, cyclophosphamide and ciclosporin). The reference categories are as follows: (A) ≤65 years, ≤65 years, female sex; (B) the non-presence of the specific comorbidity; (C) rheumatoid arthritis; (D) remission/low disease activity, no glucocorticoids; and (E) methotrexate monotherapy. Missing values were imputed via multiple imputation. N=2222. Compared with table 1, the following numbers of patients were excluded: 27 patients receiving IL-1 inhibitors, 11 patients receiving belimumab, 8 patients receiving apremilast, 6 patients with non-systemic JIA, one patient receiving multiple bMARDs/tsDMARDs. bDMARD, biological disease-modifying antirheumatic drug; CVD, cardiovascular disease; CTD, connective tissue diseases; DMARD, disease-modifying anti-rheumatic drugs; DA, disease activity; GC, Glucocorticoids; IL, interleukin; JAK, Janus kinase; TNF, tumour necrosis factor; tsDMARD, targeted synthetic disease-modifying anti-rheumatic drugs.
Results of the multivariable ordinal logistic regression using the proportional odds model
Arterial hypertension, CVD, chronic lung disease (including chronic obstructive pulmonary disease, asthma and interstitial lung diseases), and CKD showed significant associations with COVID-19 severity (table 2 and figure 1B). The strongest association was found for patients having both comorbidities, arterial hypertension and CVD (OR 2.4, 95% CI 1.7 to 3.6).
With respect to the underlying RMD entity, PsA was associated with less severe COVID-19 course in comparison to RA (OR 0.5, 95% CI 0.27 to 0.74) (table 2 and figure 1C).
Since disease activity and the use of glucocorticoids are usually linked, both factors were analysed jointly. The results are shown in table 2 and figure 1D. Remission/low disease activity with low dose GCs (1–10 mg/d) showed a significant association with worse outcome (OR 1.6, 95% CI: 1.2 to 2.0) compared with remission/low disease activity without GCs. This effect increased with higher GC doses (OR 4.6, 95% CI 1.9 to 11.4). Moderate/high disease activity but no GCs were also associated with a worse outcome compared with remission/low disease activity with no GCs (OR 1.99, 95% CI 1.28 to 3.11). Moderate/high disease activity with low-dose GC were associated with a worse COVID-19 outcome with an OR of 2.4 (95% CI 1.5 to 3.7), and in case of moderate/high disease activity with high-dose GC, this was even more prominent with an OR of 5.3 (95% CI 2.53 to 10.9).
For the analysis of the impact of RMD treatment on the outcome of SARS-CoV-2 infection, MTX monotherapy was used as reference (table 2 and figure 1E). Treatment with immunosuppressants (mycophenolate mofetil, azathioprine, cyclophosphamide and ciclosporin) was associated with a higher COVID-19 severity (OR 2.2, 95% CI 1.3 to 3.9). JAKis were also associated with a significantly worse severity (OR 1.8, 95% CI 1.1 to 2.7). The strongest association with worse outcome of COVID-19 was found for rituximab with an OR of 5.4 (95% CI 3.3 to 8.8). In contrast, TNFi showed a significant association with a better outcome of SARS-CoV-2 infection with an OR of 0.6 (95% CI 0.4 to 0.9).
Discussion
This analysis adds evidence that medication for RMD has a considerable impact on the course of SARS-CoV-2 infection. Two main results could be retrieved from this analysis: (1) TNFi is not associated with a more severe course of SARS-CoV-2 infection in patients with RMD and, (2) in contrast, immunosuppressants, JAKis and rituximab are associated with a more severe course. Moreover, it could be confirmed that general risk factors like age, male sex and certain chronic conditions are also associated with greater severity of SARS-CoV-2 infection in patients with underlying RMD.1 2
RMD-specific risk factors have been described. The impact of disease activity and GC use are of utmost importance. Disease activity and the use of GC are usually linked. Analysing these effects separately from each other is very difficult because of the known confounding by indication in the setting of observational data. In a correspondence to the COVID-19 mortality analysis of the GRA data set,4 this interaction was shown.13 Here, we present similar results. However, in this analysis, GC use was associated with worse outcome even in patients in remission or low disease activity.
In this analysis, PsA was associated with a better COVID-19 course compared with RA. In the COVID-19 mortality analysis, PsA was not significantly associated but also showed an OR of less than 1.0 (0.75, 95% CI 0.53 to 1.07). Whether the positive association seen in our analysis is due to true differences between the diseases or unmeasured confounders is not clear. However, the risk of severe infection in bDMARD-treated patients with psoriasis compared with patients with RA is much lower, which might be a signal of different susceptibility for severe infections.14
A very important finding of our analysis is the potential beneficial effect of TNFi. This association was not seen in an earlier mortality analysis, although TNFi showed also an OR of less than 1.0 (0.9; 95% CI: 0.5 to 1.4).4 This discrepancy might be due to the large heterogeneity in the GRA data set with large differences between the countries regarding the outcomes. In the analysis by Sparks et al. TNFi were used as reference medication and therefore, due to methodological reasons, the impact of TNFi could not be estimated in this study.5 There are also clinical trials using TNFi in different settings of COVID-19.15
In the GRA analysis concerning the risk of mortality, sulfasalazine was significantly associated with mortality.4 In our analysis, sulfasalazine was not associated with COVID-19 severity, which may be due to more homogenous data with regard to healthcare system-related factors.
Regarding the influence of rituximab, there is growing evidence for an association with a worse outcome. This has been shown in various settings in RMDs.4 5 16–18 In our analysis, we confirmed these results. The influence of B-cell depletion/anti-CD20 antibodies like rituximab on COVID-19 outcome has also been studied in other diseases in which these treatments are used.19 20 For example, observational studies from multiple sclerosis showed a similar association of rituximab with severe COVID-19 outcome as in RMD.21
Data addressing an influence of JAKis on COVID-19 outcome are still limited. Thus, our analysis adds important knowledge showing an association of JAKi as RMD treatment with a more severe course of COVID-19. A negative association with COVID-19 outcome was also seen in the RA analysis of the GRA data set.5 In an analysis from Sweden, an increased risk of COVID-19-related hospitalisation as well as COVID-19-related death has been described for patients under therapy with JAKis.16 In contrast, owing to their anti-inflammatory potential, JAKis have been approved for the short-term treatment of severe COVID-19.9 22 Here, the timing and duration of the treatment seems to play a role, with negative impact in patients with RMD pretreated with JAKis and potential benefits when initiated to treat severe SARS-CoV-2 infection. A pathophysiological explanation could be that type I interferon response is crucial in the initial phase of infection for a good outcome of SARS-CoV2 infection.23 Therefore, inhibition of the type I interferon pathway by JAKi in the early phase of infection might contribute to more severe COVID-19.
The strengths of this analysis in comparison to the GRA data lie in the fact that our data are more homogenous as they were collected in a single country within one healthcare system and similar treatments and chances of care for all included patients.
However, there also are study limitations. Missing data on known confounders like RMD disease duration and number of RMD pretreatments limit the interpretation. Especially for rituximab and JAKi, it is known that they are often used in non-responder to MTX/TNFi.24 25 Therefore, the negative impact of those therapies on COVID-19 severity needs to be interpreted carefully. Similarly, we do not have detailed data on RTX dosage and—even more important—time of last infusion to be able to calculate the number of days between RTX treatment and date of SARS-CoV-2 infection. Furthermore, we do not know if the RMD treatment was paused due to acute SARS-CoV-2 infection. Although most patients continue their RMD treatment in the pandemic as stated in the treatment recommendations, in the case of an acute symptomatic infection especially in hospitalised patients, it is recommended to pause the immunomodulating treatment.26–28 Differential effects of the RMD treatment might therefore also be explained by different half-lives of these drugs.
In conclusion, risk factors for higher severity of SARS-CoV-2 infection known for the general population, such as age, male sex and certain chronic conditions, play a similar role in patients with RMDs. In addition, further risk factors need to be taken into account, for example, the influence of higher disease activity with an increased risk of worse outcome even without using GCs on the one hand and association of chronically administered GCs with a similar worse outcome on the other. Regarding RMD medication, our data show that treatment with TNFi was associated with better outcome of SARS-CoV-2 infection than MTX. Moreover, treatment with immunosuppressants, JAKi and rituximab was associated with worse outcome of SARS-CoV-2 infection. These associations may be attributed to residual and unmeasured confounding due to higher burden of comorbidity or cumulative effect of therapies. Taken together, while it is crucial to control RMD disease activity, the medication used to achieve this control needs to be carefully chosen.
Data availability statement
Data are available upon reasonable request. Applications to access the data should be made to the COVID-19 steering committee of the German Society for Rheumatology.
Ethics statements
Patient consent for publication
Ethics approval
The study was approved by the ethics committee of the Justus-Liebig-University Giessen (#52–50) and is registered at EuDRACT (2020-001958-21#). For the present analysis, we included data from 30 March 2020 to 9 April 2021.
Acknowledgments
The authors thank all physicians and personnel involved in the documentation of the cases in our registry: Dr Fredrik Albach, Dr Annette Alberding, Dr Tobias Alexander, Professor Dr Rieke Alten, Dr Susanne Amann, Dr Christopher Amberger, Dr Michaela Amberger, Dr Bianka Andermann, Nils Anders, Ioana Andreica, Dr Jan Andresen, Dr Nikolaos Andriopoulos, Dr Peer Aries, Professor Dr Martin Aringer, Dr Uta Arndt, Sarah Avemarg, Professor Dr Marina Backhaus, Professor Dr Christoph Baerwald, Dr Erich Bärlin, Dr Nora Bartholomä., Dr Hans Bastian, Dr Michael Bäuerle, Dr Jutta Bauhammer, Dr Christine Baumann, Professor Dr Heidemarie Becker, Dr Klaus Becker, Dr Michaela Bellm, Dr Sylvia Berger, Dr Gerhard Birkner, Professor Dr Norbert Blank, Daniel Blendea, Dr Hans Bloching, Dr Stephanie Böddeker, Dr Susanne Bogner, Dr Martin Bohl-Bühler, Sebastian Böltz, Dr Ilka Bösenberg, Nicole Böttcher, PD Dr Jan Brandt-Jürgens, Dr Matthias Braun, Dr Matthias Braunisch, Dr Jan Phillip Bremer, Dr Matthias Broll, Dr Andreas Bruckner, Dr Veronika Brumberger, Dr. Martin Brzank, Dr. Sahra Büllesfeld, Sandra Burger, Dr Gamal Chehab, Dr Michaela Christenn, Dr Anne Claußnitzer, Professor Dr Kirsten de Groot, Dr Elvira Decker, Dr Frank Demtröder, Dr Jacqueline Detert, Dr Rainer Dörfler, Dr Ines Dornacher, Dr Elke Drexler, Dr Edmund Edelmann, Dr Roman Eder, Dr Christina Eisterhues, Dr Andreas Engel, Dr Joachim Michael Engel, Dr Brigitte Erbslöh-Möller, Dr Miriam Feine, PD Dr Martin Feuchtenberger, Professor Dr Dr Christoph Fiehn, PD Dr Rebecca Fischer-Betz, Professor Dr Martin Fleck, Dr Stefanie Freudenberg, Dr Christian Fräbel, Dr Petra Fuchs, Dr Regina Gaissmaier, Dr Ino Gao, Oliver Gardt, Dr Georg Gauler, Dr Katrin Geißler, Dr Joachim Georgi, Dr Jasmin Gilly, Yannik Gkanatsas, Dr Cornelia Glaser, Agnes Gniezinski-Schwister, Dr Rahel Gold, Dr Norman Görl, Dr Karl-Heinz Göttl, Dr Beate Göttle, Dr Anett Gräßler, Dr Ricardo Grieshaber-Bouyer, Dr Gisela Grothues, Dr Mathias Grünke, Dr Elizabeth Guilhon de Araujo, Dr Florian Günther, Mirjam Haag, Dr Linda Haas, Dr Anna Haas-Wöhrle, Dr Denitsa Hadjiski, PD Dr Hildrun Haibel, Till Ole Hallmann-Böhm, Dr Urs Hartmann, Dr Charlotte S. Hasenkamp, Dr Maura-Maria Hauf, Dr Matthias Hauser, Dr Nicole Heel, Dr Liane Hein, Dr Reinhard Hein, Dr Claudia Hendrix, Professor Dr Jörg Henes, Dr Karen Herlyn, Dr Walter Hermann, Professor Dr Peter Herzer, Dr Andrea Himsel, Dr Guido Hoese, PD Dr Paula Hoff, Marie-Therese Holzer, Dr Johannes Hornig, Melanie Huber, Dr Georg Hübner, Dr Georg Hübner, Ole Hudowenz, PD Dr Axel Hueber, Dr Verena Hupertz, Dr Elke Iburg, Dr Annette Igney-Oertel, Dr Steffen Illies, PD Dr Annett M. Jacobi, Ilona Jandova, Dipl.-Med. Christiane Jänicke, Dr Sebastian T. Jendrek, Dr Anne Johannes, Dr Aaron Juche, Dr Sarah Kahl, Dr Ludwig Kalthoff, Dr Wiebke Kaluza-Schilling, Dr Eleni Kampylafka, Dr Antje Kangowski, Dr Andreas Kapelle, Dr Kirsten Karberg, Dr Dorothee Kaudewitz, Dr Bernd Oliver Kaufmann, Professor Dr Gernot Keyßer, Dr Nayereh Khoshraftar-Yazdi, Dr Matthias Kirchgässner, Dr Matthias Kirrstetter, Dr Birgit Kittel, Dr Christoph Kittel, Julia Kittler, Dr Arnd Kleyer, Dr Claudia Klink, Dr Barbara Knau, Professor Dr Christian Kneitz, Anna Knothe, Dr Katrin Köchel, Dr Benjamin Köhler, Dr Peter Korsten, Dr Magdolna Kovacs, Dr Dietmar Krause, Dipl.-Med. Gabi Kreher, Dr Rene Kreutzberger, Dr Eveline Krieger-Dippel, Professor Dr Klaus Krüger, Dr Brigitte Krummel-Lorenz, Dr Martin Krusche, Dr Holger Kudela, Dr Christoph Kuhn, Dr Kerstin Kujath, Dr Reiner Kurthen, Dr Rolf Kurzeja, Peter Kvacskay, Professor Dr Peter Lamprecht, Sabine Langen, Dr Heiko Lantzsch, Dr Petra Lehmann, Dr Nicolai Leuchten, PD Dr Christian Löffler, Dr Dorothea Longerich-Scheuß, Dr Gitta Lüdemann, Dr Thomas Lutz, Vanessa Maerz, Dr Hartmut Mahrhofer, Dr Ingeborg Maier, Professor Dr Karin Manger, Professor Dr Elisabeth Märker-Hermann, Dr Anette Märtz, Dr Anette Märtz, Hanin Matar, Dr Johannes Mattar, Dr Sebastian Maus, Dr Ursula Mauß-Etzler, Dr Regina Max, Dr Florian Meier, Dr Adelheid Melzer, Carlos Meneses, Dr Hans-Jürgen Menne, Dr Helga Merwald-Fraenk, Dr Claudia Metzler, Dr Sabine Mewes, Dr Harriet Morf, Dr Harald Mörtlbauer, Dr Markus Mortsch, Dr Burkhard Muche, PD Dr Niels Murawski, Dr Antoine Murray, Dr Jana Naumann, Dr Anabell Nerenheim, Dr Joachim Neuwirth, Phuong Nguyen, Dr Stine Niehus, Dr Martin Nielsen, Dr Matthias Noehte, Dr Dirk Nottarp, Dr Dieter Nüvemann, Dr Wolfgang Ochs, Dr Sarah Ohrndorf, Dr Jürgen Olk, Dr Silke Osiek, Dr Filiz Özden, Dr Bettina Panzer, Dr Alina Patroi, Dr Ulrich Pfeiffer, Dr Dorothea Pick, Dr Marta Piechalska, Dr Matthias Pierer, I. Pohlenz, Dr Mikhail Protopopov, Dr Almut Pulla, Dr Michael Purschke, Dr Judith Rademacher, Dr Wolf Raub, PD Dr Jürgen Rech, Dr Sabine Reckert, Dr Sabine Reckert, Dr Anke Reichelt de Tenorio, Dr Christiane Reindl, Dr Annja Reisch, Professor Dr Gabriela Riemekasten, PD Dr Markus Rihl, Dr Viale Rissom, Dr Karin Rockwitz, Dr Maike Rösel, Dr Markus Röser, Dr Christoph Rossmanith, PD Dr Ekkehard Röther, Dr Fabian Röther, Dr Maria Roth-Szadorski, Professor Dr Martin Rudwaleit, Dr Petra Saar, Jasemine Saech, Dr Oliver Sander, Dr Eva Sandrock, Dr Ertan Saracbasi-Zender, Dr Michael Sarholz, Dr Christoph Schäfer, Dr Kerstin Schäfer, Dr Martin Scheel, Dr Stefan Schewe, Dr Hermine Schibinger, Magnus Schiebel, Dr Andreas Schieweck-Güsmer, Dr Susanne Schinke, Dr Ulrike Schlenker, Dr Daniel Schlittenhardt, PD Dr Marc Schmalzing, Dr Verena Schmitt, Dr Matthias Schmitt-Haendle, Dr Sebastian Schnarr, Dr Dieter Schöffel, Dr Michaela Scholz, Dr Jutta Schönherr, Dr Ulrich Schoo, Dr Judith Schreiber, Anna-Sophie Schübler, Dr Florian Schuch, Dr Ilka Schwarze, Dr Carola Schwerdt, Dr Eva Seipelt, Dr Matthias Sekura, Dr Jörg Sensse, Dr Nyamsuren Sentis, Dr Christine Seyfert, Ondrej Sglunda, Dr Naheed Sheikh, Dr Iris Sievert, Dr David Simon, Marta Sluszniak, Dr Katharina Sokoll, Dr Sigrid Sonn, Dr Susanna Späthling-Mestekemper, Dr Lydia Spengler, Gerald Stapfer, Dr Nicolai Steinchen, Dr Mirko Steinmüller, Karen Steveling, Dr Karin Stockdreher, Dr Helga Streibl, Professor Dr Johannes Strunk, Dr Mechthild Surmann, Dr Ingo H. Tarner, Dr Stefanie Tatsis, Dr Astrid Thiele, Dr Jan Thoden, Dr Anika Tuleweit, Professor Dr Peter Vaith, Dr Inka Vallbracht-Ackermann, Dr Susanne Veerhoff, Dr Susanne Veerhoff, Professor Dr Nils Venhoff, Dr Anita Viardot, Lisa Vinnemeier-Laubenthal, Dr Markus Voglau, Dr Marcus von Deimling, Dr Cay-Benedict von der Decken, Dr Heike von Löwis, Dr Marisa Walther, Dr Sven Weidner, Dr Martin Weigelt, Professor Dr Stefan Weiner, Dr Jutta Weinerth, Dr Angela Weiß, Dr Martin Welcker, Dr Stephanie Werner, Dr Dirk Wernicke, Dr Franziska Wiesent, Professor Dr Peter Willeke, Dr Lea Winau, Dr Hans Wisseler, Dr Matthias Witt, Dr Stefan Wolf, Dr Nina Wysocki, Dr Panagiota Xanthouli, Dr Monika Zaus, Dr Markus Zeisbrich, Dr Silke Zinke
References
Footnotes
Twitter @rheuma_doktorin, @ChSpecker
ACR and RH contributed equally.
Contributors ACR, RH, MS and UM-L had access to the study data, developed the figures and tables, and vouched for the data and analyses. MS performed the statistical analyses and contributed to data quality control, data analysis and data interpretation. ACR, RH, BFH, AK, HM-L, AP, JR, TS, AS, HS-K, REV, CS and UM-L contributed to data collection, data quality control, data analysis and data interpretation. All authors contributed to the intellectual content during the drafting and revision of the work and approved the final version to be published. ACR and RH act as guarantors.
Funding The registry is funded, in part, by the German Society for Rheumatology. RH is funded, in part, by a JLU Career grant of the Justus-Liebig-University Giessen, Germany.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.