Article Text

Abstract
Despite the heterogeneity of the giant cell arteritis (GCA) at the level of clinical manifestations and the cellular and molecular players involved in its pathogenesis, GCA is still treated with standardised regimens largely based on glucocorticoids (GC). Long-term use of high dosages of GC as required in GCA are associated with many clinically relevant side effects. In the recent years, the interleukin-6 receptor blocker tocilizumab has become available as the only registered targeted immunosuppressive agent in GCA. However, immunological heterogeneity may require different pathways to be targeted in order to achieve a clinical, immunological and vascular remission in GCA. The advances in the targeted blockade of various molecular pathways involved in other inflammatory and autoimmune diseases have catalyzed the research on targeted therapy in GCA. This article gives an overview of the studies with targeted immunosuppressive treatments in GCA, with a focus on their clinical value, including their effects at the level of vascular inflammation.
- giant cell arteritis
- biological therapy
- glucocorticoids
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
The interleukin-6 receptor blocker tocilizumab is the only registered targeted immunosuppressive agent in giant cell arteritis (GCA), being effective in about the half of the treated patients.
The targeted inhibition of various immunological pathways are currently being tested in GCA.
Future studies with targeted immunosuppressive agents in GCA should include both evaluation of clinical and immunological parameters in addition to multiple vascular imaging modalities.
Introduction
Giant cell arteritis (GCA) is the most prevalent inflammatory disease of medium size and large arteries affecting almost exclusively people older than 50 years of age. GCA is regarded as a spectrum of diseases, from cranial (C)-GCA, to large vessels (LV)-GCA and combinations thereof, with or without features of polymyalgia rheumatica (PMR).1 GCA can be a serious debilitating disease, with acute ischaemic complications such as sight loss and stroke due to vascular inflammation and stenosis, and dissection of aorta due to formation of an aneurysm.
Despite the huge impact of the disease on the quality of life of the patients with GCA, the therapeutic options available for GCA are yet very limited. Standardised treatment of GCA consists of high dose glucocorticoids (GC) to induce remission, followed by a long-term, gradual tapering regimen to maintain remission. Despite of chronic GC use with their well-known side effects2 vascular inflammation is not always adequately controlled3 and up to 75% of GCA patients experience relapses.4 Powerful GC-sparing medication and a better control of the disease activity and secondary damage with disease modifying drugs remain thus important unmet needs in GCA.
Several attempts have been made to achieve a GC-sparing effect using conventional synthetic immunosuppressive agents. The pooled analysis of individual patient data5 of three randomised controlled trials (RCTs) (a total of 161 patients) comparing addition of a low to moderate dose of methotrexate (7.5–15 mg/week) vs placebo, revealed a modest decreased risk of relapses in the patients receiving methotrexate, higher rates of GC-free remission and lower cumulative GC doses. In this meta-analysis, the number of patients needed to treat with methotrexate to prevent a first relapse is 3.6. Therefore, methotrexate may be used as an adjunctive therapy in GCA patients at high risk of GC toxicity or relapsing patients.6 There is until now insufficient evidence for efficacy of any other conventional synthetic immunosuppressive agent.6 The advances in the pathophysiological knowledge regarding GCA and the plethora of targeted drugs becoming available for other autoimmune diseases, have catalysed the research on targeted therapy in GCA. This article gives an overview of the studies with targeted biological and synthetic immunosuppressive agents in GCA.
Potential cellular and molecular targets of immune intervention in GCA
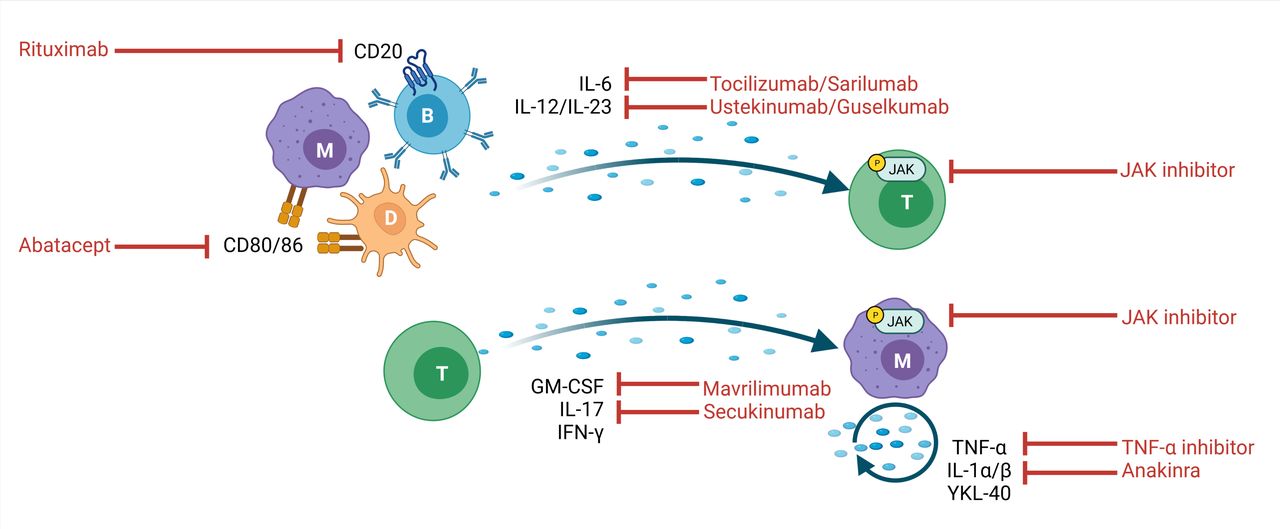
GCA is a granulomatous vasculitis that is postulated to start with the activation of the resident adventitial dendritic cells (DC).7 This results in a chemokine-mediated influx of T cells, monocytes and B cells in the vessel wall that perpetuate and amplify the local inflammatory cascade (figure 1). Through interaction with the resident vascular cells which trigger remodelling and neoangiogenesis, this uncontrolled immune process will eventually jeopardise the architecture of the vessel wall. DC stimulate T cells with their cognate peptides bound to MHC class II molecules, costimulatory molecules (ie, CD80/CD86) and cytokines. Among these cytokines, interleukin (IL)-12 promotes the CD4 +T helper 1 (Th1) cell response with production of interferon (IFN)-γ, whereas IL-1β, IL-6 and IL-23 favour the expansion of CD4 +T helper 17 (Th17) cells which produce IL-17.8 9 The Janus kinase-signal transducer and activator of transcription (JAK-STAT) signalling plays an important role in multiple cytokine pathways, including the Th1 and Th17 response.10 Another key cellular player in GCA is the macrophage. Macrophages are activated by IFN-γ producing T cells and produce tumour necrosis factor (TNF)-α and IL-6.11 12 An important factor controlling the macrophage phenotype is granulocyte-macrophage colony-stimulating factor (GM-CSF). GM-CSF is actively produced in temporal artery (TA) biopsies of GCA patients.13 GM-CSF-skewed, CD206+MMP9+ macrophages in the TA express high levels of YKL-40 which may stimulate tissue destruction and angiogenesis through IL-13receptor α2 signalling.14 Targeting GM-CSF or YKL-40 may thus inhibit macrophages that are currently insufficiently suppressed by GC. B cells are present in the adventitia and media of both TA and aorta GCA, where they can organise in tertiary lymphoid organs.15 16 B cells themselves can produce several pro-inflammatory cytokines such as IL-6, TNF-α and GM-CSF.17
{kind=link}
Schematic representation of the most important cellular players in the immunopathogenesis of giant cell arteritis (GCA) (D, dendritic cell, M, monocyte/macrophage, T, T cell, B, B cell), their cytokine/soluble products and the potential targets and tools of therapeutic intervention in GCA. Created with BioRender.com. CD, cluster of differentiation; IFN, interferon; IL, interleukin; JAK, Janus kinase; GM-CSF, granulocyte-macrophage colony-stimulating factor; TNF, tumour necrosis factor.
Taken together, GCA is a heterogeneous disease, not only clinically but also at the level of pathogenic cellular and molecular pathways,18 possibly requiring different immunosuppressive agents in order to achieve a clinical, immunological and vascular remission.
Targeted therapy in GCA
Table 1 gives an overview of the prospective clinical trials with targeted immunosuppressive agents in GCA.
Overview of the prospective studies with targeted immunosuppressive agents in giant cell arteritis (GCA)
Cytokine-targeting
TNF-α inhibitors
In a phase 2 RCT including 44 new-onset GCA patients infliximab therapy did not increase the proportion of patients without relapse at week 22 compared with placebo.19 An RCT including 70 new-onset GCA patients treated with adalimumab or placebo also failed to achieve its primary end point of being in remission on less than 0.1 mg/kg of prednisone at week 26.20 An RCT with etanercept in 17 new-onset and relapsing patients did show a GC-sparing effect,21 however, the primary outcome being GC-free remission at 12 months was not met.
IL-6 and IL-6 receptor inhibitors
Villiger et al22 reported the results of a single centre, phase 2, RCT with tocilizumab (an IL-6 receptor blocker) in GCA. Patients with new-onset (n=23) or relapsing (n=7) disease received either tocilizumab intravenously or placebo until week 52 in combination with a predefined GC regime. The primary outcome being the complete remission rate at a prednisolone dose of 0.1 mg/kg/day at week 12 was met (85% vs 40% in the tocilizumab and placebo group, respectively, p=0.03). The complete remission rate at week 52 also strongly favoured tocilizumab (85% vs 20%, p=0.001). The treating physicians were not blinded for C reactive protein (CRP)/erythrocyte sedimentation rate (ESR). There were no safety issues. This was the first RCT with tocilizumab in GCA pointing out the efficacy of this drug in combination with GC. In a follow-up study approximately half of the GCA patients (9/17) remained in lasting remission after discontinuation of tocilizumab. The rest of the GCA patients relapsed after a mean time of 6.4 (range 2–14) months during the total 44 months follow-up. In this small study none of the relapses was accompanied by new vascular complications.
This phase 2 study was followed by the Giant Cell Arteritis Actemra (GiACTA) trial in 201723: a multicentre, double-blind, placebo controlled, phase 3 trial with tocilizumab. In this study 251 patients with either new-onset (119) or relapsing GCA (132) were randomly assigned, in a 2:1:1:1 ratio, to one of the following arms: (1) subcutaneous (s.c.) tocilizumab (162 mg) 1 x/week combined with 26-week GC taper; (2) tocilizumab s.c. 1 x/2 week combined with 26 week GC taper; (3) placebo combined with a 26-week GC taper; (4) placebo combined with a 52-week GC taper. The primary outcome, being the rate of sustained GC-free remission at week 52 in arm 1 and 2 as compared with arm 3 was clearly achieved (56% and 53% in arm 1 and 2, respectively, vs only 14% in arm 3, p<0.001). The treating physicians were blinded for CRP/ESR. In a sensitivity analysis that excluded the requirement for a normalised CRP from the definition of sustained remission, the percentage of GC-free remission was 59% vs 20% in the first and third arm, respectively. The relapse rate was 23% and 26% in arm 1 and 2 as compared with 68% and 49% in arm 3 and 4, respectively. The number of GCA patients needed to treat with tocilizumab 1×/week during 52 weeks in order to prevent one relapse is 2.2. Most GCA relapses (72%) occurred while patients were still receiving GC, with more than one-fifth of relapses occurring in patients receiving >10 mg/day prednisolon.24 In the 2-year follow-up of the GiACTA study,25 215 of the initial 251 patients were included. No new adverse event(AE) were reported over the 3-year follow-up period. Of the 59 patients in GC-free remission in arm 1 at the end of GiACTA, 25 (42%) maintained tocilizumab-free and GC-free clinical remission, as compared with 8 of the 36 (29%) in the follow-up of arm 2. After 3 years of total follow-up, the use of GC was 33% lower in the patients initially treated in arm 1 as compared with arm 2. In relapsing patients, tocilizumab-based regimens restored clinical remission after (median): 15 days for tocilizumab alone, 16 days for tocilizumab +GC and 54 days for GC alone. Whether a GC-free induction of remission was possible with tocilizumab was not yet clear. To address this question, a recent investigator-initiated, single-arm, open-label trial included 18 new-onset GCA patients who received 500 mg methylprednisolone intravenously for three consecutive days, combined with a single infusion of tocilizumab (8 mg/kg), followed by tocilizumab s.c. 1x/week.26 The primary endpoint of an early remission at 4 weeks was not reached. Anterior ischaemic optic neuropathy occurred in one patient with extensive atherosclerosis at day 15. This proof-of concept study does not support an induction of remission with tocilizumab monotherapy.
In GiACTA, tocilizumab improved clinical outcomes regardless of the clinical phenotype (C-GCA only, PMR only or both).27 Baseline parameters predicting treatment failure in the tocilizumab/GC group included female sex, lower GC doses and worse patient reported outcome measures.28 In a daily practice study, tocilizumab improved GCA clinical outcomes significantly and demonstrated effectiveness in the subgroups of patients with PMR symptoms and GCA-related visual manifestations at GCA diagnosis.29
Trials with the anti-IL-6 monoclonal antibody sirukumab30 and another anti-IL6 receptor monoclonal antibody sarilumab (NCT03600805) were prematurely terminated due to sponsor decision or slow inclusion rate caused by COVID-19 pandemic, respectively.
The clear positive results of the GiACTA study set the stage for the rapid approval of tocilizumab for the treatment of GCA by both US and European regulatory authorities in 2017. The use of tocilizumab in GCA is currently recommended by clinical guidelines especially in patients at high risk of GC toxicity or relapsing patients6 31 but more recently also in new-onset GCA.32 Less clear is what is the optimal duration of tocilizumab treatment in GCA. The available follow-up data25 33 show that approximately half of the patients in clinical remission after 1 year of treatment maintain long-term treatment-free remission. Based on these data we recommend discontinuation of tocilizumab treatment after 1 year, followed by close monitoring especially during the first 6 months. Alternatively, the dosage of tocilizumab may be gradually decreased. In relapsing patients, combined tocilizumab-GC-based regimens are expected to restore clinical remission within 2–3 weeks.
As tocilizumab is not effective in half of the treated patients and as there are also contra-indications for or relevant side effects of tocilizumab (especially serious infections, leucopenia but also hypercholesterolaemia),22 23 25 the search for alternative treatments in GCA is ongoing.
IL-1 inhibitors
Anakinra is a blocker of the interleukin-1-type 1 receptor (IL-1R1), whereby the biological activity of IL-1α and IL-1β is inhibited. Two case series including a total of nine patients with refractory GCA34 35 showed efficacy of anakinra 100 mg/day as reflected by clinical and biochemical improvement accompanied by either resolution or decrease of vascular inflammation on 18F-fluorodeoxyglucose positron emission tomography (18FDG-PET) scan.34 35 The GCA and Anakinra Trial (GiAnT, NCT02902731) is currently recruiting patients. An RCT with the IL-1β blocker gevokizumab initiated in 2014 was prematurely discontinued due to the slow inclusion rate.
IL-17 inhibitors
Recently, a multicentre, phase 2 RCT exploring the efficacy and safety of secukinumab compared with placebo in combination with an open label GC taper regimen was completed. Fifty patients were randomised (1:1) to either 300 mg secukinumab or placebo s.c. during 52 weeks combined with a 26-week GC taper regimen. The primary endpoint, being the proportion of patients in sustained remission until week 28 in secukinumab vs placebo was met (70.1% vs 20.3%, respectively). At 52 weeks, 59.3% vs 8.0% of the patients were still in sustained remission.36 Secukinumab was well-tolerated. A phase 3 study with secukinumab (NCT04930094) was designed but not started recruiting yet.
IL-12/IL-23 inhibitors
In a proof-of concept, prospective, open-label study, ustekinumab showed a GC-sparing effect in 14 patients with refractory GCA.37 In a prospective, open-label study, 25 patients with relapsing-refractory GCA received ustekinumab 90 mg every 12 weeks.38 Ustekinumab significantly reduced the GC dose from a median of 20 mg (15 25) to 5 (2.5, 5) mg daily at week 52 (p<0.001). There were no relapses in the ustekinumab group. Approximately one-fourth of the patients was able to stop the GC completely. There were no unexpected AE. Two of five patients who stopped the treatment had subsequently a PMR relapse without apparent GCA relapse. In another prospective, open-label trial, inclusion of 20 patients with either new-onset or relapsing GCA treated with ustekinumab was initially planned. All patients received a 24-week GC taper and ustekinumab 90 mg till week 52.39 Surprisingly, only three patients achieved the primary endpoint which was GC-free remission rate at week 52. The study was prematurely terminated after 7 of the initial 10 patients had relapsed. One serious AE (SAE) occurred. The discrepancy of the outcome of these two trials may be related to differences in the study design. Currently, the Ustekinumab for the Treatment of Relapse of Refractory Giant Cell Arteritis trial is recruiting patients (NCT03711448). The IL-23 receptor blocker guselkumab is currently also being investigated in a phase 2 trial (NCT04633447).
GM-CSF inhibition
The preliminary results of a phase 2 RCT with mavrilimumab (an anti-GM-CSF-Rα monoclonal antibody) were recently presented.40 Seventy active GCA patients received either 150 mg mavrilimumab (n=42) or placebo (n=28) s.c. every 2 weeks. Primary endpoint was the time to first adjudicated flare by week 26. Median time to flare by week 26 could not be estimated (NE) in the mavrilimumab group due to too few events, NE vs 25.1 week in mavrilimumab and placebo group, respectively, p=0.0263. Sustained remission at week 26 occurred in 83.2% vs 49.9% (mavrilimumab vs placebo, p=0.0038). Results were consistent across disease type subgroups. No vision loss occurred. AE and SAE did not differ between the groups.
Targeting JAK-STAT signalling
In a recent phase two, open-label study, 15 patients with relapsing GCA were treated with 4 mg baricitinib daily for 52 weeks in addition to a standardised GC taper.41 The primary endpoint was the safety of treatment. At week 52, 14/15 (93%) patients had at least one AE, mostly infections. Only 1 of 14 (7%) patients relapsed during the study. The remaining 13 patients achieved stable GC-free remission at week 52. Another RCT with upadacitinib (NCT03725202) is ongoing.
Targeting T cell activation
Abatacept is a soluble CTLA4Ig fusion protein that binds to CD80 and CD86 on antigen-presenting cells, thereby inhibiting the activation of T cells. Forty-nine GCA patients were initially all treated with abatacept 10 mg/kg intravenously on days 1, 15 and 29 and week 842 in combination with a 28-week GC taper. At week 12, patients in remission (n=41) were assigned to either abatacept monthly (n=20) or placebo (n=21). The primary end point, being the relapse-free survival rate at 12 months was met (48% abatacept vs 31% placebo; p=0.049). There were no safety issues. A longer duration of remission was seen in abatacept vs placebo group (median duration 9.9 vs 3.9 months; p=0.023). These promising results led to the design of the ABAGART trial (NCT04474847) which is ongoing.
In a prospective, open-label study, 33 biopsy-proven GCA patients were randomised to receive either tocilizumab (intravenously 8 mg/kg/month or s.c. 162 mg/week) or abatacept (s.c. 125 mg/week) in addition to GC.43 All patients in the tocilizumab intravenously group experienced a response (57% complete response and 43% partial response) vs tocilizumab s.c. 83% and abatacept 62%. After 12 months of therapy, 100% of patients in the tocilizumab groups and 43% of abatacept group were receiving doses of prednisone lower than 7.5 mg/day.
Targeting B cells, rituximab (anti-CD20)
There is one case report describing efficacy of B-cell depletion therapy in a patient with relapsing GCA.44 Another case report describes the use of rituximab in a neutropenic patient with GCA, however, no data on the effectiveness of rituximab is provided.45 There is yet no clinical trial with rituximab in GCA.
In summary, from the targeted immunosuppressive agents employed in clinical studies in GCA, strong evidence for a beneficial clinical effect exists so far only for tocilizumab. Secukinumab, ustekinumab, anakinra, mavrilimumab, abatacept, the JAK-STAT inhibitors and rituximab remain promising therapeutic tools but they still have to prove their value before finding their way to the daily clinical practice in GCA. The TNF-α blockers have failed that path.
Effects of targeted immunosuppressive therapy on vascular inflammation
The effect of targeted immunosuppressive therapy on vascular inflammation has been investigated in several prospective studies (table 2).
Prospective, follow-up imaging studies monitoring the therapeutic response of tocilizumab on vascular inflammation in giant cell arteritis (GCA)
Tocilizumab
Adler et al, performed MR angiography (MRA) in all 20 tocilizumab patients at baseline.33 At 52 weeks it was repeated in those patients who showed mural enhancement at inclusion. There was a trend to a reduction of vasculitis areas over time (from 61% to 57%) in patients in stable clinical remission. All patients in lasting remission showed MRA enhancement at follow-up, raising questions about the MRA as follow-up tool (as serum biomarkers did not indicate subclinical activity) and/or the efficiency of tocilizumab on the vascular inflammation. In a real-life, single centre study46 including GCA patients with refractory/relapsing disease treated with tocilizumab, the TA Halo Scores decreased during the follow-up, while the axillary artery Halo Score remained stable. The total vascular score on 18FDG-PET-CT also decreased. In another single centre, observational study47 achievement of clinical remission in 83.3% (25 of 30) (patients with refractory LV-GCA starting treatment with tocilizumab, was accompanied by a reduction of 18F-FDG vascular uptake. However, less than one-third of the patients showed complete normalisation of vascular uptake. Imaging improvement was also found in new-onset LV-GCA patients (n=19) treated with tocilizumab.48 PET Vascular Activity Score (PETVAS) decreased from 19.8 baseline to 7.47 at mean 15.3 months of follow-up. The changes in PETVAS were similar to those found in parallel methotrexate and GC groups. In another study,49 25 patients starting treatment with tocilizumab underwent an FDG-PET-CT scan at the baseline visit and at follow-up every 6 months. In addition to clinical improvement, PETVAS was also significantly reduced over a 2-year treatment period. Repeated FDG-PET scans after tocilizumab discontinuation showed worsening of PET activity in five out of six patients, with two patients subsequently experiencing clinical relapse. In a study exploring a ultrashort GC strategy combined with tocilizumab50 ultrasound evaluation of the intima–media thickness showed a slow and steady decrease in TA but no clear long-term effect on the LV.
Ustekinumab
In line with the clinical data, imaging with CT angiography in 8 patients with LV-GCA also demonstrated improvement of the vasculitis in all patients, with full resolution in 4 patients.38
In summary, follow-up information on vascular activity as reflected by imaging is still limited and hampered by the lack of uniform definitions of clinical and vascular disease activity and chronic vascular damage in GCA. Although the presented studies generally document improvement of the vascular activity after tocilizumab, prospective and head-to-head comparison of different imaging modalities are warranted.
Conclusion
GCs are still central in the treatment in GCA but the arsenal of targeted therapies might expand in the years to come. So far, tocilizumab has been approved showing efficacy in approximately half of the GCA patients. Since multiple immune pathways are involved in GCA, investigation of other targeted therapies and combination with conventional immunosuppressive agents is awaited. Future studies with targeted therapies should include both evaluation of clinical and immunological parameters of GCA activity as well as multiple vascular imaging modalities.
Ethics statements
Patient consent for publication
Ethics approval
This study does not involve human participants.
References
Footnotes
Twitter @sleenyannick
Correction notice This article has been corrected since it was first published online. Kornelis S M van der Geest was incorrectly listed as Niels van der Geest.
Contributors MS: study concept and design, manuscript preparation, manuscript editing, final approval of the article. KSMvdG: study concept and design, manuscript preparation, manuscript editing, final approval of the article. YvS: study concept and design, manuscript preparation, figure preparation, manuscript editing, final approval of the article. EB: study concept and design, manuscript preparation, manuscript editing, final approval of the article.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests NvdG and EB report personal fees from Roche, outside of the submitted work.
Provenance and peer review Commissioned; externally peer reviewed.