Article Text

Abstract
Background Scanty data on the immunogenicity of the BNT162b2 vaccine in patients with psoriatic arthritis (PsA) on Tumor Necrosis Factor inhibitors (TNFi) have been published.
Objective To investigate the humoral response to BNT162b2 vaccination patients with PsA on TNFi, comparing immunogenicity with healthy controls.
Methods Forty patients with classified PsA on TNFi undergoing vaccination with the BNT162b2 mRNA SARS-CoV-2 vaccine (BioNTech/Pfizer) were enrolled. Fifteen days after the second shot, serum IgG levels against SARS-CoV-2 (Abbott ARCHITECT i2000SR, positivity cut-off 50 AU/mL) were assayed in all patients. Clinimetrics and treatment data were gathered. TNFi treatment was not discontinued throughout the whole period, whereas methotrexate (MTX) was discontinued for 1 week after each shot in those on combination therapy. Sera from healthcare professionals were considered as healthy controls for 1:1 propensity score matching; any of them was taking medication.
Student’s t-test and logistic regression were used for investigating differences in immunogenicity between groups and predictors of antibody response.
Results Clinical Disease Activity Index did not change before and after vaccination (7.06±5.23 to 7.10±5.27, p=0.92).
Patients with PsA achieved a positive anti-SARS-CoV-2 IgG level with a mean (±SD) of 13794.44±15 815.42 AU/mL. Although lower, the antibody level was not significantly different from matched controls (19227.4±11.8460.45 AU/mL, p=0.08). In the overall sample, those on MTX (12/80, 15%) had a trend toward lower immune response (p=0.07); glucocorticoid therapy (11/80, 13.8%) predicted lower antibody levels (p=0.04).
Conclusions Continuing TNFi in patients with PsA throughout the vaccination did not hamper immunogenicity.
- vaccination
- arthritis
- psoriatic
- tumor necrosis factor inhibitors
Data availability statement
Complete dataset is available upon request and provided local Ethics Committee approval for sharing.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
Vaccination against COVID-19 should be strongly considered for most patients with psoriatic arthritis (PsA). Growing evidence suggests that disease-modifying antirheumatic drugs should be continued before and after vaccination.
This study confirms that TNF inhibitors (TNFi) in patients with PsA during vaccination with BNT162b2 are safe and are not associated with hampered immune response.
TNFi may not be discontinued in patients with PsA during vaccination with BNT162b2.
Introduction
Psoriatic arthritis (PsA) is an immune-mediated inflammatory disease typically involving peripheral joints, enthesis, spine and skin.1 Several studies reported an increased risk of infection in patients with rheumatic diseases, mainly due to untreated disease activity, comorbidities and/or long-term use of immunosuppressants.2 Patients with inflammatory diseases, including psoriasis and PsA, when analysed as a combined group, might have a slightly increased risk of death from COVID-19 compared with healthy people.3 Continuing treatment may help to prevent hospitalisation due to COVID-19, possibly by keeping disease activity in check.4 5 Vaccination against COVID-19 is a valid strategy for most patients with rheumatic diseases, including PsA.5 6 Nevertheless, the immune response to vaccination can be somewhat reduced in patients with several disease-modifying antirheumatic drugs (DMARDs).5 Of note, patients on immunosuppressive medications were excluded from phase III clinical trials of mRNA vaccines,7 so it is unclear whether DMARDs should be continued before and after vaccination. Despite several real-world studies showing successful immunogenicity of mRNA vaccine in immunocompetent people, a recent report suggested that either TNF inhibitors (TNFi) or methotrexate (MTX) might hamper immune response to anti-SARS-CoV-2 in patients with inflammatory diseases.6 8 To date, scanty data on the immunogenicity of the BNT162b2 mRNA vaccine in patients with PsA on TNFi have been published. Notably, recent reports are characterised by within-cohort heterogeneity about the timing of the anti-SARS-CoV-2 IgG test after the second shot.6 9 Furthermore, the wide variability of the protocols of discontinuation of csDMARDs and steroid therapy at vaccination also is noticeable.
Our study aimed at investigating the humoral immune response to BNT162b2 vaccination in a cohort of patients with PsA on TNFi with homogeneous disease characteristics and treatment comparing vaccine immunogenicity with healthy controls.
Methods
Patients with classified PsA according to ClASsification criteria for Psoriatic ARthritis (CASPAR)10 on TNFi followed at a PsA clinic of our tertiary centre were longitudinally observed from April to June 2021. Our institution set up a vaccination campaign during which patients with PsA received two shots of the BNT162b2 mRNA SARS-CoV-2 vaccine (BioNTech/Pfizer) on 24 April and 15 May. Our study included all consecutive patients who underwent vaccination during such a campaign. Fifteen days after the second shot, all patients with PsA underwent IgG test against the S1 domain of the spike protein of SARS-CoV-2 (Abbott ARCHITECT i2000SR, positivity cut-off 50 AU/mL); blood samples were collected and analysed at the same institution’s laboratory. TNFi treatment and non-MTX csDMARDs were not discontinued throughout the whole period. In all patients, MTX was held the week after each shot, in observance of the American College of Rheumatology Guidance to the timing of vaccination, adopted in our hospital.11 Patients were contacted to record when they took the last MTX dose before vaccination.
Demographic and clinical characteristics, including disease phenotypes, Disease Activity in PsA (DAPSA), Psoriasis Area Severity Index (PASI), Clinical Disease Activity Index (CDAI), Morisky Medication Adherence Score on 4 Items (MMAS-4) and PsA Impact of Disease (PsAID12),12 were recorded at baseline consultation before vaccination. At the same time, patients were asked for prior COVID-19 and/or related symptoms.
The assessment of CDAI was also repeated at the time of anti-SARS-CoV-2 IgG testing. We also recorded any vaccine reaction and/or adverse event during the observation period.
Sera from 59 healthcare professionals employed at our institution, gathered 15 days after the second BioNTech/Pfizer vaccine shot from January 2021 to February 2021, were considered as healthy controls for 1:1 nearest-neighbour Propensity Score (PS) matching.13 PS is an epidemiological tool used for the adjustment of non-randomised longitudinal studies. It is a conditional probability of being exposed to a disease given a set of covariates. In brief, this was carried out using the patients' age and gender, with a selected calliper of 0.2. A proper assessment of postmatching balance was also carried out as previously described.13 As a result of PS matching, 19 controls were lost, leading to a postmatched sample of 80 individuals, consisting of 40 patients in the PsA group and 40 patients in the control group.
We assessed the difference in anti-SARS-CoV-2 IgG levels between groups with Student’s t-test. Paired t-test and McNemar’s test were used to determine the difference between mean CDAI Score and remission rate at different time points, respectively. Associations of recorded covariates with IgG levels and CDAI scores after vaccination were investigated using linear regression.
Results
Mean age (±SD) of patients with PsA was 52.85±10.41 years; 22/40 (55%) were female, with a mean disease duration of 11±9.0 years. Oligoarticular involvement was the prevalent phenotype (22/40, 55%), with a minority of patients being affected with axial disease (6/40, 15%). By first shot, 12/40 patients with PsA (30%) were on MTX combotherapy at a mean dose of 14.79±3.27 mg weekly. Patients took the last MTX dose a median of 3 days (min–max 1–6) before vaccination. Overall, 11 out of 40 (27.5%) were on glucocorticoids at a mean dose of 4.66±1.67 prednisone equivalent. Mean DAPsA was 11.34±7.81. Patients with PsA in our cohort had mild skin involvement with a mean PASI of 0.56±1.01 and moderate life impact (mean PsAID12 3.94±2.40). Patients with PsA declared high medication adherence (median MMAS-4 0, min–max 0–1). None of them reported prior COVID-19 or SARS-CoV-2 infection-related symptoms.
Mean age of PS-matched controls was 50.80±12.16 years (p=0.42) with similar gender distribution (female 18/40 45%, p=0.37). Patient characteristics are detailed in table 1. None of the controls was taking immunosuppressants or glucocorticoids at vaccination. At the first shot, fever was the most frequent symptom accompanying vaccination (7/40, 17.50%), followed by arthralgia and lymphadenopathy (2/40, 5%, for both). At the second shot, the percentage of patients experiencing joint pain was significantly higher (9/40, 22.50%, p=0.007), with the fever still occurring in the 17.50% (7/40) of the cohort (table 2).
Patient characteristics
Vaccine reactions
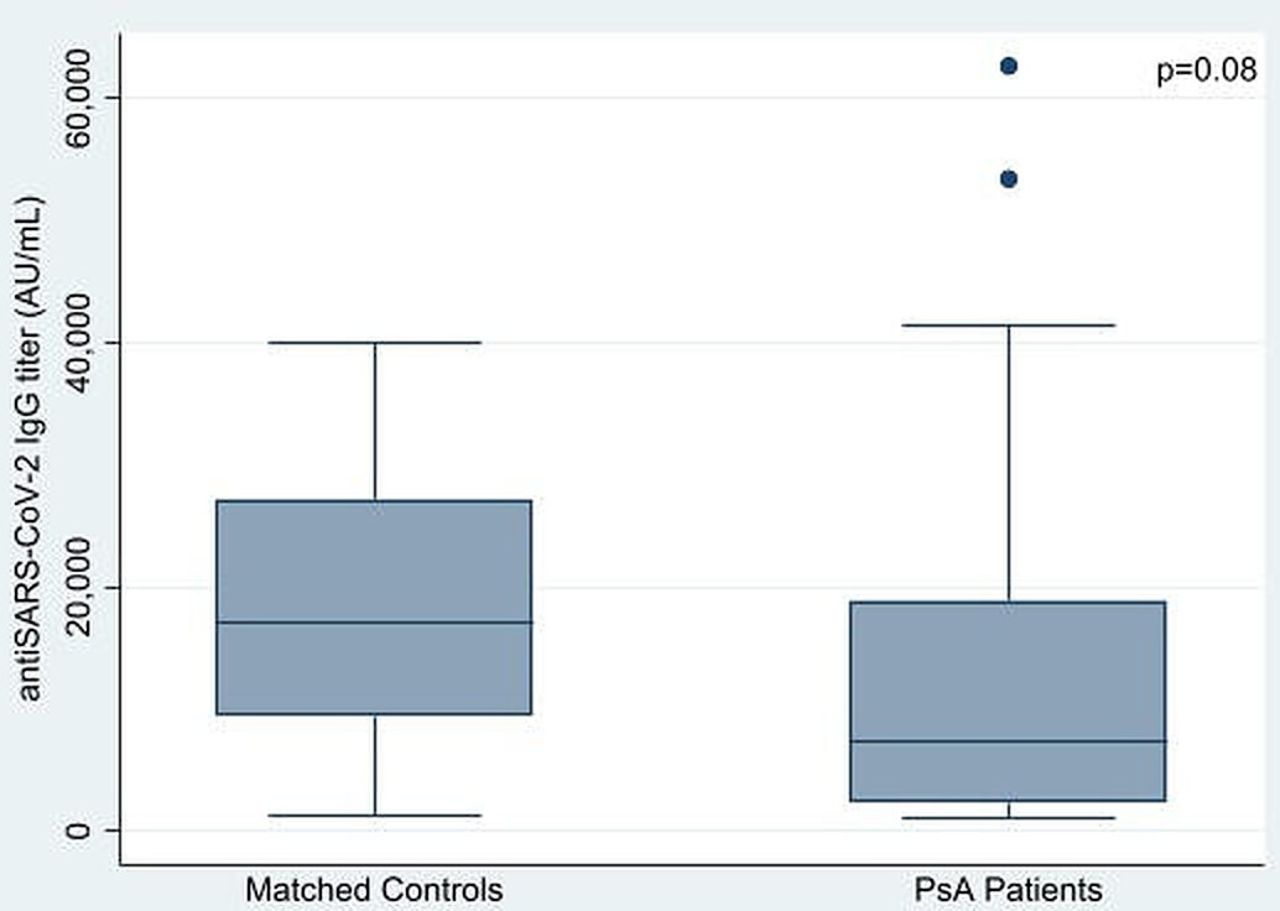
No changes of clinical disease activity between baseline (CDAI 7.06±5.23) and after the complete vaccination (CDAI 7.10±5.27, p=0.92) were detected. Consistently, the CDAI-based remission rate remained similar (28/40 vs 23/40, p=0.31). All patients with PsA showed a positive immune response with a mean anti-SARS-CoV-2 IgG level of 13794.44±15 815.42 AU/mL. Although quantitatively lower, this was not significantly different from matched controls’ titre, which was 19227.4±11.8460.45 AU/mL (p=0.08, figure 1).

{kind=link}
Anti-SARS-CoV-2 IgG titers of patients with Psoriatic Arthritis (PsA) and matched healthy controls.
No difference was shown between patients with PsA with or without MTX (9331.80±12 131.09 vs 15707±16 991.04 AU/mL respectively, p=0.24; 95% CI −17 368.82 to 4618.42), also after adjusting for sulfasalazine treatment (p=0.51; 95% CI −20 997.61 to 10 682.96). The same findings were also observed when patients with PsA taking glucocorticoids were compared with those without (9974.282±12 357.45 vs 15 243.47±16 909.93 AU/mL, p=0.35; 95% CI −16 623.61 to 6085.24). Considering the whole PS-matched sample, hence including healthy controls, MTX use was not associated with a lower anti-SARS-CoV-2 IgG titre (p=0.07; 95% CI −17 116.44 to 224.69); the same was true for sulfasalazine (p=0.67; 95% CI −8738.55 to 5652.92). In contrast, glucocorticoid use was a predictor of lower immunogenicity (p=0.04; 95% CI −8800.32 to −118.76). We also investigated whether disease activity flared because of MTX discontinuation after vaccination shots. In this regard, MTX discontinuation did not predict a higher CDAI Score (p=0.09; 95% CI −2.16 to 5.41).
Discussion
This study analyses the immunogenicity of the BNT162b2 vaccine in patients with PsA on TNFi, comparing them to PS-matched controls. An arbitrary IgG serum level representative of vaccine efficacy that was not defined as robust evidence has not been provided yet. To clearly depict the effect of TNFi on vaccine immune response, only MTX was discontinued for 1 week after each shot. Like recent reports,9 the immunogenicity of BNT162b2 was not hindered in patients with PsA on TNFi compared with healthy controls. In a recent report from Mahil et al on patients with psoriasis, the rate of serological conversion of those on MTX was quite low, contrasting with our results and with a previous study in which patients who were taking MTX showed adequate humoral responses after the first shot of BNT162b2.9 14
Unlike our cohort, adherence to MTX was confirmed in all patients in the study by Mahil et al,9 without any pause in the vaccination period. On this basis, we can argue that MTX not leading to decreased IgG titers might be a consequence of its discontinuation 1 week after each shot. We also showed that neither vaccination nor MTX discontinuation impacted PsA disease activity, which remained stable. Consistently with recent literature,15 glucocorticoid use at vaccine administration might lead to lower IgG titers.
Among study limitations, we acknowledge the small sample size. Additionally, we cannot exclude the fact that a few patients got asymptomatic SARS-CoV-2 infection at any time before vaccination, as immunisation status was not assessed. Furthermore, we did not perform a postvaccination serum viral neutralising test.
Notably, our analysis was neither intended nor powered to show the difference between patients assuming or not assuming background MTX mainly for the lack of comparator group continuing treatment.
Our study has some strengths. First, PS matching on prospectively gathered data, together with homogeneous treatment management, allowed to mitigate bias due to non-randomisation. Moreover, the timing of sera sampling was the same for all patients, and to reduce the within-cohort variability, an anti-SARS-CoV-2 IgG assay was run once for all the samples at the same laboratory.
In conclusion, continuing TNFi therapy in patients with PsA throughout the vaccination period was not associated with hampered immune response and it was safe. Although MTX was not associated with decreased IgG titers, more data are needed to clarify whether holding MTX after vaccination may lead to optimal immunogenicity.
Supplemental material
Data availability statement
Complete dataset is available upon request and provided local Ethics Committee approval for sharing.
Ethics statements
Patient consent for publication
Ethics approval
This study follows the Declaration of Helsinki and received local ethics committee approval (Comitato Etico Interregionale Policlinico di Bari) as part of BIOPURE Study (Approval n.5940). Participants gave informed consent to participate in the study before taking part.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
VV and PS are joint first authors.
Twitter @vincevenerito
Contributors Study design: VV, GL, PS and ST. Data gathering and manuscript editing: VV, GL and PS. Data analysis: VV, PS and ST. Supervision: FI and ST.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.