Article Text

Abstract
Objective To determine the risk of herpes zoster (HZ) in Korean patients with rheumatoid arthritis (RA) receiving Janus kinase inhibitors (JAKis).
Methods We performed a nested case–control study with 1:10 matching for sex and age using single-centre prospective cohorts of patients with RA receiving targeted therapy in Korea. Then we performed conditional logistic regression analyses to determine the risk associated with JAKi use compared with biologic disease-modifying antirheumatic drug (bDMARD) use, with adjusting for various factors. We also used logistic regression analysis to identify other risk factors for the development of HZ in JAKi users.
Results From a total of 1147 patients, 61 cases and 610 matched controls were selected. In conditional logistic regression analysis, JAKi use did not increase the risk of HZ development (OR 1.35, 95% CI 0.70 to 2.61) after adjusting for other factors. Rather, duration of RA less than 10 years (OR 0.54, 95% CI 0.30 to 0.97) and having had three or more previous targeted therapies (OR 5.29, 95% CI 1.45 to 19.31) were risk factors for HZ. Among JAKi users, higher disease activity score 28-erythrocyte sedimentation rate (DAS28-ESR) (OR 1.44, 95% CI 1.06 to 1.97) was identified as a risk factor in addition to three or more previous targeted therapies (OR 10.12, 95% CI 1.92 to 53.49).
Conclusions The number of previous targeted therapies, but not JAKi use, was identified as a risk factor for HZ development in Korean patients with RA in a real-world setting. High disease activity was an additional risk factor for JAKi users.
- arthritis
- rheumatoid
- biological therapy
- antirheumatic agents
Data availability statement
Data are available upon reasonable request. Data are available upon request as it contains sensitive and potentially identifying patient information. Any request regarding data and the study itself should be directed to the corresponding author.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Patients with rheumatoid arthritis (RA) treated with Janus kinase inhibitors (JAKis) were at increased risk of herpes zoster (HZ) development in Korea.
What does this study add?
. After adjusting for other factors, JAKi use was not a significant risk factor for HZ development compared with biologic disease-modifying antirheumatic drug use.
Having had three or more previous targeted therapies was found to be a risk factor for HZ development in patients with RA. Among JAKi users, high disease activity was identified as an additional risk factor.
How might this impact on clinical practice or further developments?
Patients with RA receiving JAKis require careful monitoring for HZ development, especially those with high disease activity or those with a history of three or more previous targeted therapies.
Further study is necessary to determine the preventive effect of vaccination against HZ.
Introduction
The introduction of targeted therapy has provided new treatment opportunities for patients with rheumatoid arthritis (RA) who showed inadequate responses to conventional synthetic disease-modifying antirheumatic drugs (csDMARDs) including methotrexate (MTX).1 In addition to biologic DMARDs (bDMARDs) which have been used for a longer time, Janus kinase inhibitors (JAKis) have increased the achievement of clinical remission or, at least, low disease activity.1 2
Many studies have been conducted to assess the safety of targeted therapy with a focus on infections.3–5 Even if RA disease activity is well-controlled by targeted therapy, serious infection can interfere with the continuity of treatment and increase the risk of an RA flare by causing drug cessation.6 For example, many studies have shown an association between increased risk of tuberculosis (TB) development and bDMARDs, especially for tumour necrosis factor (TNF) inhibitor users.7 8 Hence, screening for latent TB infection is recommended for patients with RA before initiating targeted therapy.9
Herpes zoster (HZ) is another rising concern with the use of JAKis.2 10 HZ is caused by reactivation of varicella zoster virus (VZV) and induces severe pain, such as postherpetic neuralgia, degrading the quality of daily life for several months to years.11 JAKis including tofacitinib, baricitinib and upadacitinib are currently available for RA treatment in Korea. Tofacitinib was the first approved JAKi in 2015, followed by baricitinib in 2017 and upadacitinib in 2020. The use of these agents raised the possibility of an association with increased risk of HZ.2 Clinical trials suggested that the incidence rate (IR) of HZ was higher in patients taking JAKis than placebo group or in those taking bDMARDs.5 12 This IR was especially higher in Asian patients, including those in Korea and Japan, in whom the IR was approximately doubled.13 Furthermore, recent studies on patients with RA receiving upadacitinib conducted in Japan reported an approximately twofold to threefold higher IR of HZ than global trials, and the exact reason was unknown.12 14 However, in Korea, few studies have been performed to identify any increased risk of HZ in JAKi users compared with bDMARD users in a real-world setting.
In this study, we aimed to determine the risk of HZ in Korean patients with RA using JAKis compared with those using bDMARDs. Additionally, we aimed to identify the risk factors for HZ development among JAKi users.
Methods
Data source
We extracted data from the prospective cohorts of patients with RA receiving targeted therapy conducted in an academic referral hospital in Korea. The cohort named Hanyang University Medical Centre Arthritis Network-BIOlogics Registry for RA (HUMAN-BIORRA) included patients with RA receiving bDMARDs, and the HUMAN-Small Molecule Inhibitor Registry for RA (SMIRRA) included those receiving JAKis. Patients aged 19 or older who met the 1987 American College of Rheumatology (ACR) classification criteria or 2010 ACR/EULAR classification criteria for RA and who signed the informed consent were registered in those cohorts. Patients were followed up every 6 months with blood tests and interviews for the assessment of disease activity, drug compliance, adverse events (AEs) and quality of life. Information about the development of opportunistic infections was prospectively collected in the form of AEs, including HZ, TB, pneumonia and so on. To minimise the possibility of missing information, medical records of patients on AEs were reviewed together.
Study population
All patients with RA registered in either cohort for bDMARD or JAKi users were included in this study. The HUMAN-BIORRA started in June 2011 and the HUMAN-SMIRRA started enrolment in March 2017. The observation period began when the patient was enrolled in the cohort, that is, when the patients started their targeted therapy. The observation was terminated at the time of HZ development, discontinuation of targeted therapy, or May 2020. Therefore, patients included in this analysis were on-treatment status. In cases where patients switched type of targeted therapy—mainly from bDMARD to JAKi—the drug used at the time of HZ development or used most recently was considered to be the current medication.
Matching HZ cases and controls
HZ cases
Data from patients reported to have been diagnosed with HZ were extracted during the observation periods, and these were selected as cases. The diagnosis of HZ was based on clinician’s diagnosis, regardless of whether or not a patient received antiviral therapy. To determine the effect of targeted therapy on the development of HZ, the data collected immediately before the date of diagnosis of HZ were used in the case group.
Controls
Patients without a history of HZ during the observation periods were selected as controls. In the control group, the last data collected before the end of the observation periods were used.
Matching cases with controls
Using data from the prospective cohorts, a nested case–control study was performed. We randomly selected up to ten controls for each case matched by sex and age. The division into age groups was based on the ages of 50 and 60. To minimise the loss of sample size, only the most basic characteristics, sex and age, were used for matching.
Risk factors for HZ development
The leading risk factors we considered were demographic characteristics; comorbidities; disease-related factors; and medication, including targeted therapy. Demographic information such as sex, age, height, weight and body mass index was collected. The presence of comorbidities was defined as having been diagnosed at least once during the observation periods. Duration of RA and blood tests including those for rheumatoid factor, anti-citrullinated protein antibody, erythrocyte sedimentation rate (ESR) and C reactive protein were also collected. Disease activity was assessed by Disease Activity Score (DAS) 28-ESR and physician’s global assessment in addition to patient-reported outcomes such as Health Assessment Questionnaire-Disability Index and visual analogue scale (VAS) of sleep and fatigue. The doses of MTX and glucocorticoid were based on the prescription being used on the date when data were collected. The number of csDMARDs, bDMARDs or JAKis ever used was counted using cumulative data. Since the information about HZ vaccination was collected exclusively in the JAKi users, this variable was only used for analysis in patients using JAKi.
Statistical analyses
The χ2 test or Fisher’s exact test was used for categorical variables, and the Mann-Whitney U test was used for continuous variables in comparisons between cases and controls.
Then, a conditional logistic regression analysis was performed to identify risk factors associated with HZ, especially exposure to JAKis. All the risk factors of interest and those with p<0.2 in the univariable analysis were included in the multivariable logistic regression analysis, and the adjusted OR with 95% CIs was calculated. We conducted an additional unconditional logistic regression analysis to identify risk factors for HZ development among JAKi users only, because their number was insufficient for matching. Listwise deletion was used for handling missing values in the multivariable logistic regression analysis.
All analyses were performed using SAS V.9.4 (SAS Institute), and p values <0.05 were considered statistically significant.
Results
Baseline characteristics of patients with or without HZ infection
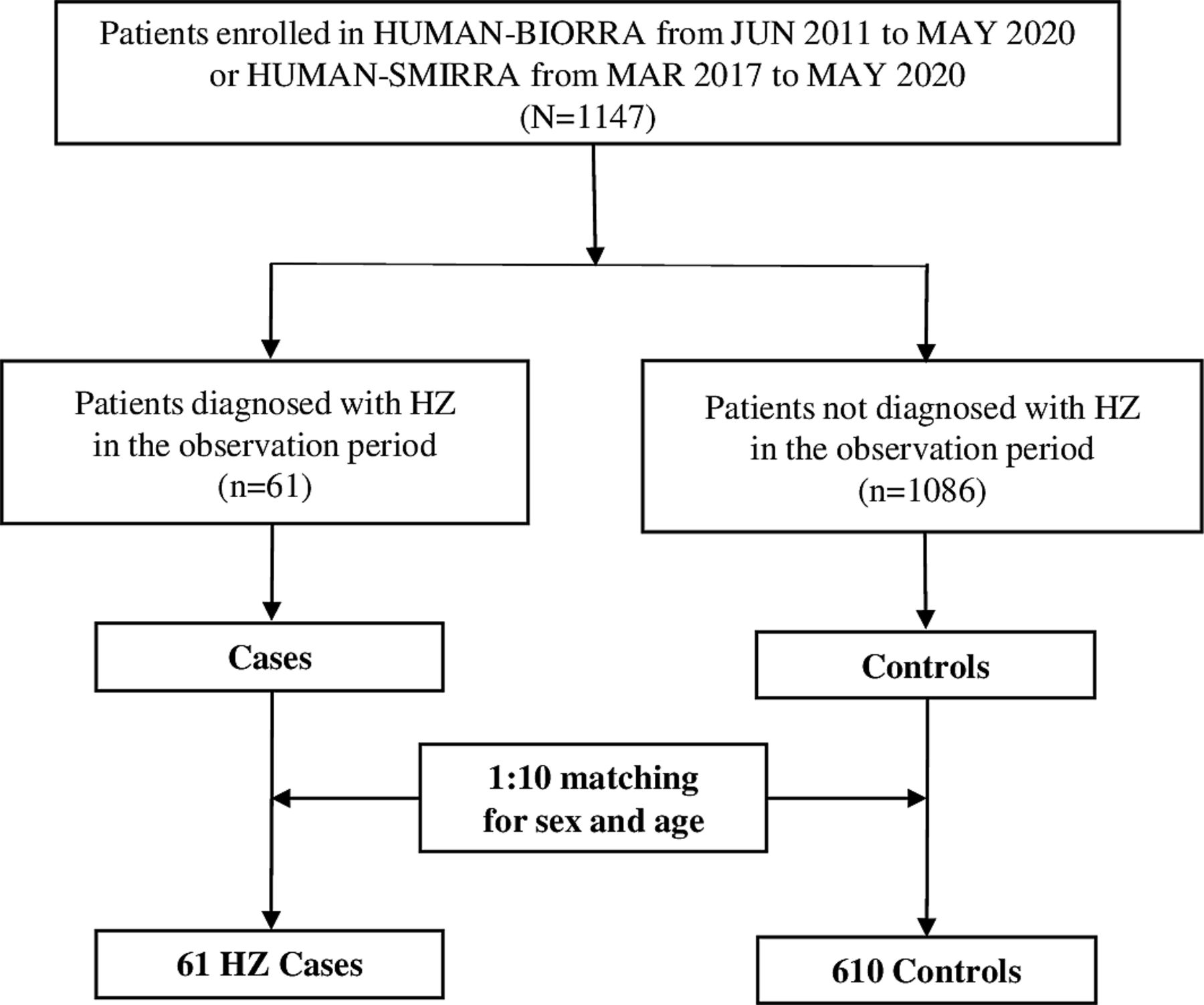
A total of 1147 patients were included in this study: 223 JAKi users and 924 bDMARD users (figure 1). There were 61 patients diagnosed with HZ during the observation period, and there were 1086 controls that did not develop HZ. After 1:10 matching for sex and age, 61 cases and 610 controls were selected as the population sampled.

{kind=link}
Flow chart of patient selection. HUMAN-BIORRA, Hanyang University Medical Centre Arthritis Network-BIOlogics Registry for Rheumatoid Arthritis; SMIRRA, Small Molecule Inhibitor Registry for RA; HZ, herpes zoster.
Table 1 shows the demographic and clinical characteristics of the study population before and after matching for sex and age. Of the 1147 participants, 86.9% were female and the mean age was 55.2 (±13.5) years. Cases tended to be older than controls (58.1 vs 55.0 years), and most of the patients in the case group were in their 50s and 60s (online supplemental figure 1). The average duration of RA was 11.2 (±8.5) years in the total population. Tofacitinib was the most commonly used agent for targeted therapy in the case group (23.0%), and there was a significant difference between cases and controls (p=0.037). Number of previous targeted therapies was also significantly different (p=0.009). DAS28-ESR was marginally higher in cases than controls (4.1±1.8 vs 3.7±1.6, p=0.056), and fatigue VAS was significantly higher in cases than controls (4.2±2.7 vs 3.5±2.7, p=0.029).
Supplemental material
Characteristics of study population before and after matching for sex and age
After matching for sex and age, the sampled population was composed of 90.2% female patients, and the mean age was 58.5 (±11.4) years. Duration of RA was significantly shorter in the case group (p=0.017). There were no significant differences in comorbidities, current medication use and disease activities between cases and matched controls. Number of previous targeted therapies remained significantly different (p=0.038).
Risk factors for HZ development
In the conditional logistic regression analysis of cases and matched controls, duration of RA, number of previous targeted therapies, JAKi use, oral glucocorticoid use, DAS28-ESR and fatigue VAS were with p<0.2 (table 2). In the multivariable analysis, the number of previous targeted therapies was a significant risk factor for HZ; patients who received three or more kinds of targeted therapies before the current agent experienced increased risk of HZ development (OR 5.29, 95% CI 1.45 to 19.31). Duration of RA was also significantly different (OR 0.54, 95% CI 0.30 to 0.97). However, JAKi (OR 1.35, 95% CI 0.70 to 2.61) and oral glucocorticoid use (OR 1.36, 95% CI 0.76 to 2.45) did not increase the risk for HZ after adjusting for other risk factors. When additional conditional logistic regression analyses were performed using models adjusting for different variables, risk of HZ was still not increased by JAKi use (table 3).
Risk factors associated with HZ development
Conditional logistic regression analysis for HZ risk in JAKi users compared with bDMARD users
There were 17 HZ cases among the 223 JAKi users, so only age, number of targeted therapies, DAS28-ESR and HZ vaccination, which were variables of interest, were included in the multivariable analysis (table 4). The analysis confirmed that three or more previous targeted therapies increased the risk of HZ development (OR 10.12, 95% CI 1.92 to 53.49), and disease activity of RA presented as DAS28-ESR (OR 1.44, 95% CI 1.06 to 1.97) was identified as an additional risk factor. There was no significant association between vaccination against HZ and HZ development among JAKi users (OR 0.39, 95% CI 0.08 to 1.93). Detailed characteristics of cases among JAKi users are presented in online supplemental table 1.
Risk factors associated with HZ development in JAKi users
Discussion
This study was a nested case–control study aimed at determining if an increased risk of HZ development exists in patients with RA receiving JAKi. We also determined the risk factors for HZ, especially among JAKi users. There were significantly more tofacitinib users in the case group, but JAKi use was not a risk factor for HZ development after adjusting for other factors in a conditional logistic regression analysis. Cases had a significantly shorter duration of RA than matched controls. Patients having had three or more previous targeted therapies were found to be at greater risk for HZ development. Among JAKi users, higher disease activity was identified as an additional risk factor. Vaccination against HZ did not show a protective effect in this study.
The occurrence of HZ is associated with the reactivation of VZV from a latent infection in sensory neurons of the cranial nerves and/or the dorsal root ganglia.11 15 The decline of the cellular immune response is a critical risk factor for HZ development and is related to ageing, immunodeficiency disorders and immunosuppressive medications.11 Accordingly, RA, as a chronic disorder with immunological dysfunctions, increases the risk of HZ.16 In previous studies, patients with RA showed an almost twofold higher risk of HZ compared with the general population, and there were no apparent regional or racial differences.17 18 In addition, previous HZ, chronic pulmonary disease and oral glucocorticoid use were also significant risk factors for HZ development.17 In the era of biological agents, there were arguments about the relationship between HZ and targeted therapy because the infection was a major concern of targeted therapy.19 However, both TNF inhibitors and non-TNF inhibitors were not associated with HZ development.17 20 In terms of JAKis, however, many studies reported an increased risk of HZ in patients with RA treated with tofacitinib.10 13 21 Older age, use of oral glucocorticoids, and the Asian population were reported to be associated with a higher risk of HZ in those studies. In addition to tofacitinib, other JAKis including baricitinib and upadacitinib showed an increased risk for HZ development in clinical trials.12 22
In our study, cases tended to be older than controls before matching. The most prevalent ages were 50s and 60s, comparable to the most prevalent ages in the general population in Korea.23 The Korean Society of Infectious Diseases (KSID) has recommended the administration of HZ vaccines to adults aged ≥60 years.24 However, a new practice guideline for vaccination developed by the Korean College of Rheumatology (KCR) and KSID in 2020 recommends that HZ vaccines should be considered for patients with autoimmune inflammatory rheumatic diseases who are aged ≥50 years.24 Considering that most patients diagnosed with HZ were in their 50s or 60s and within a year from initiating JAKis, the new guideline seems reasonable.
In the multivariable logistic regression analysis of the matched population, duration of RA was significantly shorter in the case group than in the control group. This might not mean that shorter duration of RA is a risk factor for HZ development, but rather that HZ development tends to occur during the early period of targeted therapy. In this study, more than the half of HZ cases receiving JAKi had had less than 1 year of JAKi use. This suggests that careful monitoring for HZ development is necessary for patients in the early period of targeted therapy.
Through our study, three or more previous targeted therapies were also identified as a risk factor of HZ development. This does not seem to be caused by the immunomodulatory effects of previous medications because one or two previous targeted therapies were not a significant risk factor. Rather, the change in targeted therapy is usually due to inadequate response or AEs; therefore, several changes in targeted therapy suggest insufficiently controlled disease activity of RA. The results of multivariable analysis among JAKi users revealed this more clearly. The disease activity presented as DAS28-ESR was an additional risk factor for HZ development, suggesting the importance of controlled disease activity.
One of the differences between our study and previous studies was the impact of concomitant medication. Oral glucocorticoid use has been reported to be an important risk factor in JAKi users, approximately doubling HZ risk.17 25 In our study, however, neither the concomitant use nor dose of oral glucocorticoids were significant risk factors. The reason for the difference might be that our study investigated glucocorticoid use on the date of data collection only, while previous studies allowed at least a month for extension to exposure. The concomitant use of MTX was not related to increased HZ risk in our study, consistent with results from previous studies.13 25
Vaccination against HZ has been proven to markedly reduce the incidence of HZ and postherpetic neuralgia and to also be protective for patients with autoimmune and inflammatory diseases including RA.26 27 Therefore, guidelines for patients with RA published by ACR, EULAR and KCR recommended HZ vaccines for patients with RA with high risk or plan for targeted therapy.9 24 28 However, vaccination against HZ did not show a protective effect in our study. The low vaccination rate of 18.4% among JAKi users was thought to be the main reason, and this low vaccination rate was caused by the unavailability of the recombinant zoster vaccine in Korea.
Our study had some significant aspects and findings. First, we conducted the nested case–control study using well-constructed prospective cohorts. Detailed variables such as disease activity were investigated in those cohorts. Therefore, there were more advantages for analysing risk factors compared with other data sources. In addition, we considered that current targeted therapy was more influential than previous targeted therapy, which was only included as a covariate. The relatively low incidence rate of HZ was also a reason for requiring a nested case–control design. Second, the study was meaningful in that it was conducted among Korean patients in East Asia, a known high-risk group of HZ incidence. In particular, our study identified the effect of each targeted therapy and clinical features, especially vaccination against HZ.
However, this study had some limitations. First, there is a probable lack of generalisability because this was a single-institution study. Although our hospital has the largest rheumatology centre with patients from all over the country, further studies with larger samples are required to increase the external validity of our study results. Second, history of HZ infection was not investigated in our study, though such history might make patients avoid JAKi use. This could affect the results of multivariable regression analysis, in which JAKi use was not a significant risk factor of HZ development. However, in the clinical setting, previous HZ infection was not a contraindication for JAKi; and other factors such as preference for oral regimen, comorbidities and disease activity could be important for the choice of JAKi or bDMARD. Third, we could not compare matched cases and controls when identifying risk factors for HZ among JAKi users due to the insufficient numbers.
In conclusion, JAKi use did not increase the risk of HZ in two large Korean prospective cohorts. Having had three or more previous targeted therapies was a risk factor for HZ development in patients with RA, and high disease activity was a risk factor in those treated with JAKis. However, further studies with a larger sample size and longer follow-up periods are required to investigate the relationship between JAKi use and HZ development.
Data availability statement
Data are available upon reasonable request. Data are available upon request as it contains sensitive and potentially identifying patient information. Any request regarding data and the study itself should be directed to the corresponding author.
Ethics statements
Patient consent for publication
Ethics approval
This study was approved by the Institutional Review Board of the Hanyang University Hospital (IRB No. HYUH 2020-12-024). We used the existing prospective cohort data that have already been reviewed and approved by the IRB of our institution (No. HYUH 2011-05-008, HYUH 2016-08-037, HYUH 2018-12-024). Informed consent was obtained from all patients at the time of enrolment in each registry.
Acknowledgments
We would like to thank eWorldEditing (www.eworldediting.com) for editing and reviewing this manuscript for English language.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors Y-JS, S-KC, HK and Y-KS designed the study, were responsible for the acquisition, analysis and interpretation of data, and drafted and revised the article. HWK and EN were involved in data analysis and interpretation and revision of the manuscript. C-BC, T-HK, J-BJ, S-CB and DHY were involved in data acquisition and revision of the manuscript. All authors approved the final version of the article. Y-KS accepts full responsibility as guarantor of the study.
Funding This research was supported by a grant of the Korea Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health & Welfare, Republic of Korea (grant number: HI19C0481, HC19C0052). This research was supported by Basic Science Research Programme through the National Research Foundation of Korea (NRF) funded by the Ministry of Education (NRF-2021R1A6A1A03038899).
Competing interests Y-KS has received research grants from Bristol-Myers Squibb, Eisai, Pfizer and JW Pharmaceutical. Other authors declare that there is no conflict of interest.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.