Article Text

Abstract
Objectives To propose a data-driven definition for structural changes of sacroiliac (SI) joints in the context of axial spondyloarthritis (axSpA) imaging on a large collective of CT datasets.
Methods 546 individuals (102 axSpA, 80 non-axSpA low back pain and 364 controls without back pain) with SI joint CTs were evaluated for erosions, sclerosis and ankylosis using a structured scoring system. Lesion frequencies and spatial distribution were compared between groups. Diagnostic performance (sensitivity (SE), specificity (SP), positive predictive values, negative predictive values and positive and negative likelihood ratios) was calculated for different combinations of imaging findings. Clinical diagnosis served as standard of reference.
Results Ankylosis and/or erosions of the middle and dorsal joint portions yielded the best diagnostic performance with SE 67.6% and SP 96.3%. Inclusion of ventral erosions and sclerosis resulted in lower diagnostic performance with SE 71.2%/SP 92.5% and SE 70.6%/SP 90.0%, respectively.
Conclusions Sclerosis and ventrally located erosions of SI joints have lower specificity on CT of the SI joint in the context of axSpA imaging. Ankylosis and/or erosions of the middle and dorsal joint portions show a strong diagnostic performance and are appropriate markers of a positive SI joint by CT.
- erosion
- ankylosing spondylitis
- ankylosis
- low back pain
- sclerosis
Data availability statement
Data are available upon reasonable request. Data is available from the corresponding author upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
CT is an imaging modality with emerging importance in the diagnosis of axial spondyloarthritis (axSpA). However, evidence-based criteria for defining structural lesions in this modality have been lacking to date.
What does this study add?
Sclerosis is not useful in CT imaging and should no longer be used to define structural damage to the sacroiliac (SI) joints.
The imaging criteria proposed in this study in the definition of structural lesions of the SI joints in axSpA allow a definition of the disease state based on CT data.
The exact anatomical assignment of structural lesions within the SI joint is relevant and one should evaluate lesions differently in different joint positions.
How might this impact on clinical practice or further developments?
After further validation, the criteria proposed here may be used in future cross-sectional or longitudinal studies to classify patients based on CT data.
Furthermore, our data can be used to sharpen the description of a positive MRI in axSpA.
Introduction
The impact of imaging on diagnosis and classification of patients with suspected axial spondyloarthritis (axSpA) is paramount and reflected in the dedicated imaging arm of the Assessment of Spondyloarthritis international Society (ASAS) classification criteria.1 However, there is still debate about the question what constitutes a positive image of the sacroiliac (SI) joints in terms of structural lesions on CT and MRI. This question is of importance, as the significance of structural lesions has been strengthened by the latest revision of the ASAS imaging criteria.2 Additionally, data-driven approaches to define positivity on imaging have gained traction among experts in the field.3 4
When structural lesions are assessed, several recent studies have used CT scans of the SI joints as a standard of reference,5–7 which is explained by CT’s unparalleled capacity to directly depict cortical bone and, therefore, erosions. Historically, the use of CT in axSpA imaging has been hindered by its high radiation exposure. Recent technical advances in scanner technology and acquisition protocols have decreased effective radiation close to the level of plain radiography and low-dose CT can thus be considered a practicable method in rheumatologic imaging.8 A recent investigation by our group confirmed CT as a highly specific imaging alternative whenever MRI is inconclusive or unavailable.9
To date, there is a widely accepted definition of positivity for sacroiliitis on CT in the context of axSpA. Our study aimed to define imaging features of structural damage by comparing patients with axSpA and those with low back pain or without symptoms. Based on the presence and location of structural changes on CT, we aimed to develop a data-based definition of positive sacroiliitis.
Materials and methods
Patients
Included in this analysis were patients from three study cohorts: the SacroIliac MAgnetic resonanace and Computed Tomography study (SIMACT) (n=110)5 6 10 and the Virtual Non-Calcium - Susceptibility Weighted Imaging-study (n=72),11 both prospective studies on patients with chronic LBP and possible axSpA, as well as the SacroIliac Changes in the Normal Population (SICC-NP) study, a retrospective investigation, including 818 patients from the general population.12 All patients from the two prospective cohorts received standardised laboratory testing (including HLA-B27 and C reactive protein) and clinical questionnaires (eg, Bath Ankylosing Spondylitis Disease Activity Index) as described in detail in the respective publications. For these patients, the final clinical diagnosis assigned by an expert rheumatologist served as the standard of reference. Patients from the SICC-NP study served as representative sample of the general population—this sample did not contain patients with documented LBP, known rheumatological disease, hyperparathyroidism, malignant disease of the skeleton (primary of metastatic), known infection of the skeleton or (status post) trauma of the pelvis, as laid out in the original publication. Patients with LBP were matched for age and sex with non-LBP controls in a ratio of two controls to one patient. A diagram of patient flow and clinical characteristics is provided in figure 1.

Patient flow and clinical characteristics. Significantly higher values/proportions compared with non-axSpA LBP group are marked with an asterisk (*). P values derived from Fisher’s exact test or unpaired t-tests. axPsoA, axial psoriatic arthritis; BASDAI, Bath Ankylosing Spondylitis Disease Activity Index; CRP, C reactive protein; LBP, low back pain; Nr-axSpA, non-radiographic axial spondyloarthritis; ns-LBP=non-specific low back pain; OA, osteoarthritis; OC, osteitis condensans; r-axSpA, radiographic axial spondyloarthritis (formerly ankylosing spondylitis); HTO, Hyperostosis triangularis.
Patient and public involvement
There was no specific patient or public involvement in this investigation.
Imaging procedure, scoring system and lesion definition
Patients from the two prospective cohorts received low-dose CT scans of the pelvis, while non-LBP patients received standard dose CT scans for other indications, as laid out in detail in the respective publications. All images were analysed using a semi-quantitative scoring system established in previous investigations.5 The SI joint was divided into 12 regions on each side (ventral, middle and dorsal portion) and in each portion, the iliac and sacral side were further divided into a superior and an inferior portion; erosion and sclerosis were assessed in each of these regions, while ankylosis was assessed per side. A detailed description of the scoring system is given in figure 2. All images were read by a radiological resident with 6 years of experience in musculoskeletal imaging (KZ). A subset of 50 randomly selected cases was scored by a senior radiologist with expertise in SI joint imaging (TD). For erosions, a patient was defined as positive, if more than one region exhibited unequivocal erosions. A patient was considered positive for sclerosis if extensive sclerosis was observed in more than one region. Partial or complete ankylosis on either or both sides constituted positivity for joint space alterations.
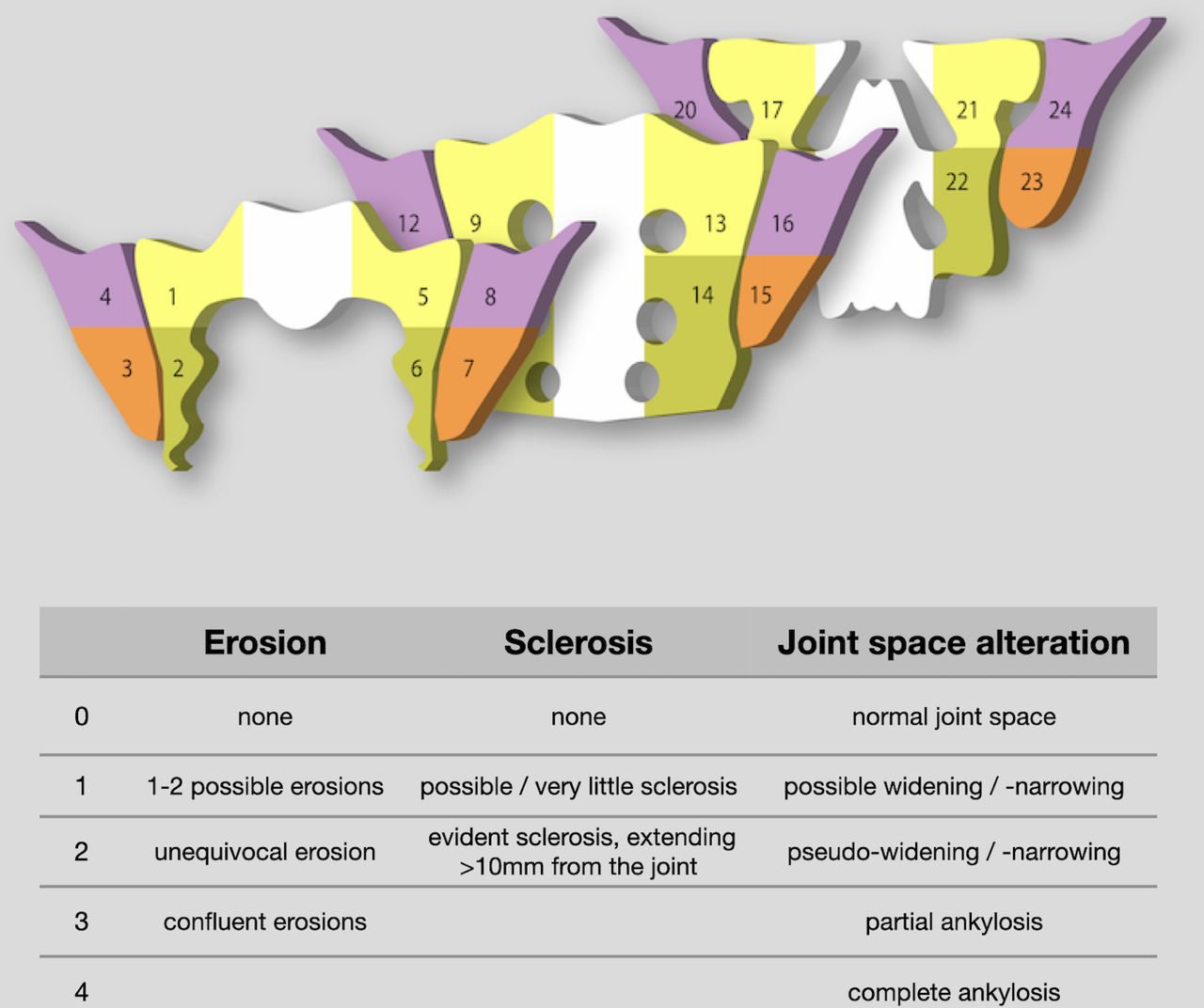
Scoring system. Segmentation of joint in ventral, middle, and dorsal parts, based on oblique coronal imaging, parallel to the second sacral vertebra. Ventral part (regions 1–8): no neural foramina visible. Middle part (regions 9–16): sacral foramina are depicted. Dorsal part (regions 17–24): sacral nerve roots and spinal canal are depicted. Erosion means hypodense disruption of the cortex of at least 1 mm, excluding tubular structures such as bone canals. Sclerosis means well demarcated increase of density of periarticular bone. Ankylosis means growth of bone across the joint space; partial ankylosis means some areas of visible joint space remain; complete ankylosis means no joint space is discernible. Graphic adapted from Diekhoff et al.5 6 10
Statistical analysis
Patients with LBP were matched with non-LBP controls in a ratio of 2 controls per patient using a propensity score matching for age and gender with a tolerance of 0.01. In a first step, comparison of lesion frequencies between three groups (non-LBP controls, non-axSpA LBP and axSpA) were performed with Fisher’s exact test. In a second step, cross-tabulations were used on symptomatic patients (non-axSpA LBP and axSpA) to compute markers of diagnostic performance, that is sensitivity, specificity, positive and negative predictive values and likelihood ratios; final clinical diagnosis served as the reference standard. Inter-reader reliability was assessed using intraclass correlation coefficients (ICC) with a two-way mixed model. All analyses were carried out using SPSS V.26 with a two-tailed significance level of p<0.05; significance levels for comparisons of lesions’ frequencies per region were adjusted for multiple comparisons (n=24) with a Bonferroni correction resulting in an adjusted significance level of p<0.002.
Results
Distribution of lesions
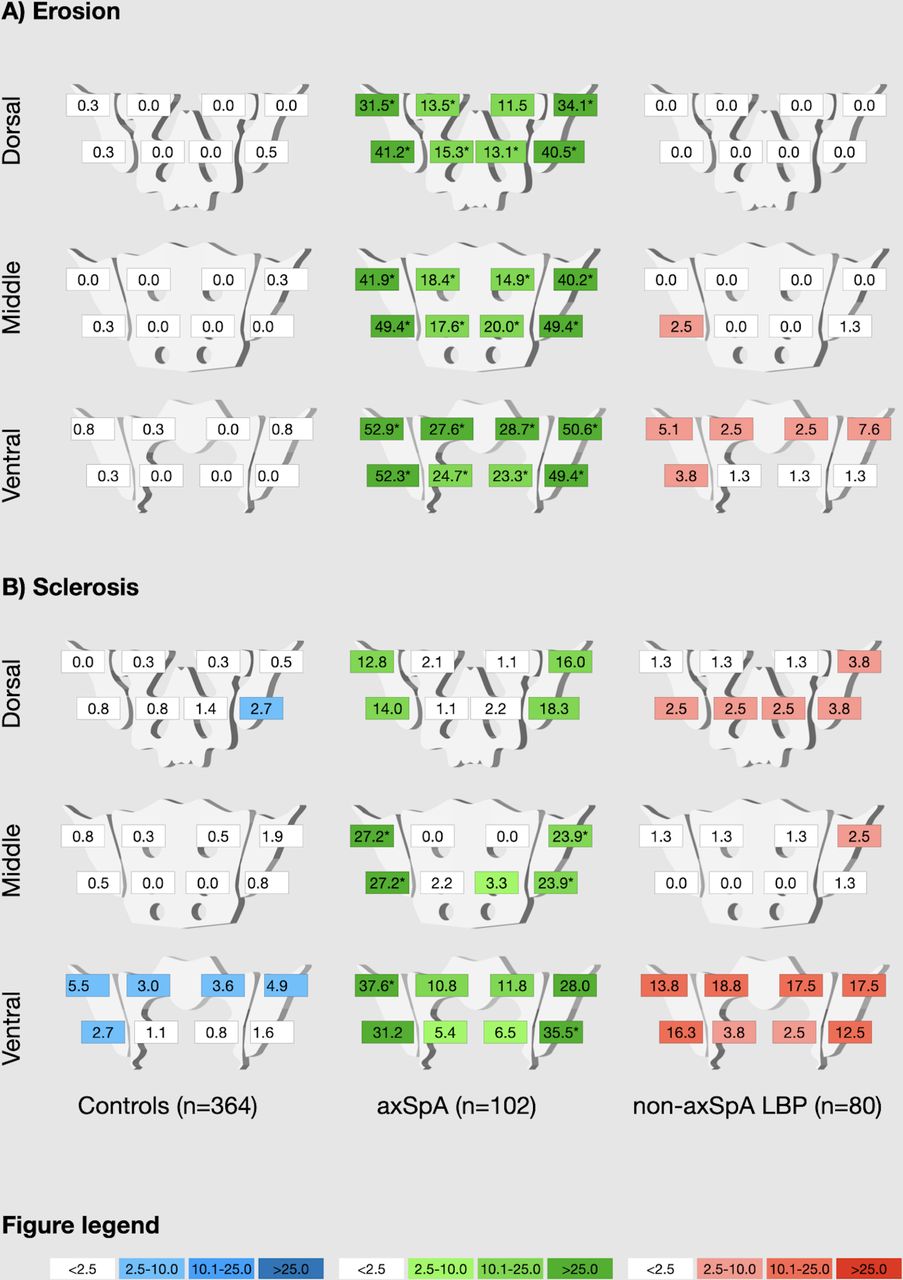
Spatial distribution of sclerosis and erosions differed significantly between patients with axSpA, non-axSpA LBP and non-LBP controls; a graphical illustration is given in figure 3 and a table of pairwise comparisons is provided as online supplemental file 1. Sclerosis was common in patients with both axSpA and non-axSpA LBP in the ventral quadrants; in the middle and dorsal quadrants, sclerosis was common in patients with axSpA and rare in patients with non-axSpA. In non-LBP controls, sclerosis was altogether rare, but most common in the ventral quadrants. Erosions were very rare in non-LBP controls and patients with non-axSpA LBP—in the latter group, however, there were some erosions observed in the ventral quadrants, especially in the ilium. Ankylosis was observed in 24.5% (25/102) of patients with axSpA but only 1.3% (1/80) of patients with non-axSpA LBP; none of the included non-LBP controls exhibited either partial or complete ankylosis.
Supplemental material
{kind=link}
{kind=link}
{kind=link}
Relative frequency of lesions across regions (%). Different colours for patient groups: blue for non-axSpA LBP controls, green for ax-SpA and red for non-axSpA LBP; shade of colour denoting frequency from white (lowest) to dark (highest) for ease of visual interpretation. Significantly higher frequencies (compared with non-axSpA LBP) are marked with asterisks (*).
From these analyses, we concluded that erosions and sclerosis of the ventral quadrants may lack specificity for axSpA and, therefore, decided to investigate lesions overall and lesions in the middle and dorsal quadrants separately for their impact on diagnostic performance.
Accuracy of imaging parameters
First, ankylosis, erosion and sclerosis were each assessed for their individual performance in distinguishing patients with axSpA from patients with non-axSpA LBP. Of these three, ankylosis alone performed the best with a high specificity of 98.8% and a high positive likelihood ratio (LR+) of 19.6; sensitivity of ankylosis, however, was low with only 24.5%. The highest sensitivity was found for erosions (52.0%) with a still very high specificity of 93.8%; when only including erosions of the ventral and middle joint portions, sensitivity decreased to 49.0% while specificity increased to 97.5%. Sclerosis alone exhibited the lowest diagnostic performance, with a sensitivity and specificity of 40.2% and 67.5%, respectively. In a second step, diagnostic performance of different combinations of these parameters was evaluated. Ankylosis and/or erosions yielded a high specificity of 92.5% with a sensitivity of 71.2% (LR+ 9.5/negative likelihood ratio (LR−) 0.31). Eliminating erosions in the ventral quadrants from the criteria for positivity increased diagnostic performance to specificity/sensitivity of 96.3%/67.6% (LR+ 18.3/LR− 0.34). When sclerosis was included, diagnostic performance declined. A full compilation of measures of diagnostic accuracies of different parameter (combinations) is given as table 1.
Diagnostic performance (n=182)
Inter-reader agreement
Inter-reader agreement expressed by ICCs was moderate for erosion (0.574; 95% CI 0.249 to 0.758; p=0.002) and good for sclerosis (0.781; 95% CI 0.644 to 0.869; p<0.001) and ankylosis (0.735; 95% CI 0.532 to 0.849; p<0.002).
Discussion
This is the first large-scale study to examine the diagnostic performance of proposed cut-off values for a positive CT in axSpA in patients with LBP. We found the highest diagnostic accuracy (LR+ 18.3; LR− 0.34; sensitivity 67.6%; specificity 96.3%) for ankylosis (partial or complete) and/or unequivocal erosion in more than one quadrant in the middle or dorsal portions of the joint.
Inclusion of sclerosis did not increase diagnostic performance, even when only the middle and dorsal portions of the joint were assessed. This is best explained by the fact that sclerosis is a shared characteristic of both inflammatory and degenerative joint disease and must, therefore, be regarded as non-specific in the absence of erosion. Historically, sclerosis has been considered an important imaging characteristic of axSpA on X-rays13 because of its superior visualisation on radiography compared with the smaller erosions it may accompany. Indeed, extensive sclerosis is currently sufficient to define a grade 2 of radiographic sacroiliitis according to the modified New York criteria.13 However, in a cross-sectional imaging, it is frequently found in differential diagnoses such as osteitis condensans.14 Erosion is considered a highly specific imaging marker of axSpA, and the data presented here confirms this. Both erosion and sclerosis were common in the ventral third of the SI joint in axSpA and control patients; this is best explained by the biophysical load distribution within the joint, which is most intense in the ventral third.15 This fact is supported by the generally observed predilection of this joint region to exhibit sclerotic and erosive lesions in mechanical joint diseases such as osteoarthritis and osteitis condensans.14 Consequently, exclusion of lesions from the ventral third of the joint increased diagnostic performance. Ankylosis is widely regarded as the most specific imaging marker of axSpA and our findings support this claim; however, alternative explanations for ankylosis exist and should be considered during image interpretation (ie, sequelae of septic arthritis, which generally affect only one joint, or diffuse idiopathic skeletal hyperostosis,16 which presents with extensive capsular ossification which may be confused with true ankylosis).17
Despite careful planning, there are limitations to this investigation that warrant critical discussion. To the best of our knowledge, this is the largest published cohort of SI joint CT datasets in a clinically well-characterised population; however, the size of the study population is still limited, and we, therefore, refrained from a validation of our proposed cut-off values. Furthermore, the study population contained a high number of clinically advanced axSpA patients, mirrored in the high rate of ankylosis. Diagnostic performance, especially sensitivity, of these values in less advanced patients may be lower. Only modest agreement regarding erosions was reached between the two readers—this is an important limitation and may be explained by an overcalling of small irregularities as erosions; further refinement of criteria for erosion is needed. Our approach using only SI joint CTs did not allow the analysis of other structural lesions such as periarticular fat metaplasia, which cannot be seen on CT. Lastly, the assessment of individual parameter accuracy remains at least in party artificial, as lesions could not be scored independently of each other.
In conclusion, we believe that the imaging criteria proposed in this study may be useful in defining structural lesions of the SI joints in axSpA. Our data suggest that sclerosis should no longer be used to define structural damage to the SI joints. We further demonstrated that the exact anatomical assignment of structural lesions within the SI joint is relevant and that one needs to evaluate lesions differently in different joint positions. The next step should be further validation on larger cohorts, ideally with additional MRI data, to define structural lesions of the SI joints.
Data availability statement
Data are available upon reasonable request. Data is available from the corresponding author upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by the institutional ethics review board of Charité Universitätsmedizin Berlin prior to respective study commencement (EA1/300/19, EA1/0886/16 and EA1/073/10). Symptomatic patients gave written informed consent; asymptomatic patients were retrospectively recruited from routine imaging in our department of radiology and the institutional ethics review board waived written informed consent to study inclusion.
Acknowledgments
The authors thank the Berlin Institute of Health for providing essential infrastructure for data collection.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
KGAH and KZ are joint first authors.
KGAH and KZ contributed equally.
Contributors KGAH: conception and design of the study, design of scoring system, article draft and critical revision of the manuscript for important intellectual content. KZ: conception and design of the study, image scoring, data evaluation, statistical calculations, article draft and critical revision of the manuscript for important intellectual content. VK and FP: patient acquisition, data collection and critical revision of the manuscript for important intellectual content. DP: patient acquisition, statistical calculations, data collection and critical revision of the manuscript for important intellectual content. DD: patient acquisition and critical revision of the manuscript for important intellectual content. JG: patient acquisition, design of scoring system and critical revision of the manuscript for important intellectual content. JS: conception and design of the study and critical revision of the manuscript for important intellectual content. TD: conception and design of the study, design of scoring system, image scoring, data evaluation and critical revision of the manuscript for important intellectual content.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests KGAH reports lecture fees from AbbVie, MSD and Novartis outside the submitted work. KZ reports funding (research grant) from the Assessment of Spondyloarthritis international Society (ASAS) during the conduct of this study. DP reports grants and personal fees from AbbVie, Eli Lilly, MSD, Novartis, Pfizer and personal fees from Bristol-Myers Squibb, Roche, UCB, Biocad, GlaxoSmithKline, Gilead, Janssen, Samsung Bioepis and UCB outside the submitted work. FP reports grants and personal fees from Novartis, Lilly and UCB, as well as personal fees from AbbVie, AMGEN, BMS, Hexal, MSD, Pfizer and Roche outside the submitted work. JS reports personal fees from AbbVie, Janssen, Merck, Novartis, UCB and Lilly, outside the submitted work. TD reports funding (research grant) from the ASAS and lecture fees from Canon Medical, AbbVie, MSD and Novartis pharma, outside the submitted work. For all other authors, none were reported.
Provenance and peer review Not commissioned; externally peer reviewed.