Article Text

Abstract
Objective To comprehensively assess multimorbidity burden in patients with rheumatoid arthritis (RA) in order to unify the multimorbidity definition for RA research and clinical practice.
Methods In this population-based study, residents of eight Minnesota counties with prevalent RA on 1 January 2015 were identified. Age, sex and county-matched non-RA comparators were selected from the same population. Diagnostic codes were retrieved for 5 years before 1 January 2015. Using two codes ≥30 days apart, 44 previously defined morbidities and 78 non-overlapping chronic disease categories based on Clinical Classification Software were defined. Prevalence of each morbidity in the RA versus non-RA cohorts was compared using false discovery rate to adjust for multiple comparisons. Morbidities more common in RA than non-RA and those with prevalence ≥5% were retained.
Results 1643 patients with RA and 1643 non-RA subjects (72% women; mean age 63.1 years) were studied. Using the 44 morbidities, multimorbidity (defined as 2+ morbidities) was present in 1411 (86%) of RA and 1164 (71%) of non-RA subjects (p<0.001) with 5+ morbidities present in 907 (55%) of RA and 619 (38%) of non-RA (p<0.001). Patients with RA had significantly higher prevalence of 24 of the 44 morbidities compared with non-RA, especially interstitial lung disease, fibromyalgia, osteoarthritis and osteoporosis. Among the additional 78 categories, 7 were significantly higher in RA than non-RA, including organic sleep disorders, vitamin D deficiency and foot ulcers.
Conclusion Patients with RA have a higher prevalence of multimorbidity compared with non-RA subjects. These results confirm the list of 44 morbidities and add several other morbidities of interest in RA.
- rheumatoid arthritis
- epidemiology
- cardiovascular diseases
Data availability statement
Data are available upon reasonable request. Mayo Clinic Institutional Review Board (IRB) policy does not allow full access of patient information to be provided to a third party without prior approval from the IRB committee overseeing this study. However, access to the complete de-identified data can be made available following approval. Requests for additional study-related data can be sent to Cynthia S. Crowson at crowson@mayo.edu.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Multimorbidity is more common in patients with rheumatoid arthritis (RA) than in those without RA.
Multiple existing definitions of multimorbidity make comparisons between cohorts difficult.
What does this study add?
This study provides a comprehensive assessment of morbidities in patients with RA compared with those without RA.
This study demonstrates that multimorbidity may have been underestimated in studies with younger RA populations, a limited set of morbidities or a limited time frame to identify morbidities.
How might this impact on clinical practice or further developments?
This comprehensive assessment of morbidities with convenient International Classification of Diseases (ICD)-9/10 code sets will facilitate easy adoption by other researchers.
Additional identified morbidities that impact patients with RA include vitamin D deficiency, hypercalcaemia, thrombocytopenia, leucopenia, restless legs, sinusitis, allergic rhinitis, erectile dysfunction, skin ulcers, foot deformities and sleep apneoa.
Introduction
Multimorbidity is common in patients with rheumatoid arthritis (RA), and it is associated with increased mortality, poorer quality of life and increased healthcare utilisation.1 2 The concept of multimorbidity, which is patient-centric instead of focused on the index disease, is important for patients with RA due to the systemic nature of the disease.3 Patients with RA have increased risks for a myriad of comorbidities that may result from the systemic inflammation that characterises RA or from adverse effects of RA treatments. This results in greater complexity that requires coordination of care across multiple providers. Furthermore, comorbidities complicate RA treatment decisions as evidence is lacking regarding how to treat patients with comorbidities that were excluded from clinical trials or are contraindications for RA therapies.
Existing literature on multimorbidity suffers from numerous definitions that make comparisons between cohorts difficult.4–8 Multimorbidity instruments developed for the general population may not include all the morbidities that are common in patients with RA. A consistent list of morbidities for patients with RA would facilitate future research. Another issue that deserves attention is the length of the lookback period to determine the morbidities. A chronic condition was defined by the US Agency for Healthcare Research and Quality (AHRQ) as a condition that lasts ≥12 months and places limitations on self-care, independent living, and social interactions; and/or requires ongoing intervention with medical products/services/equipment. Thus, a minimum of 1 year for lookback is necessary but may not be sufficient.
England et al recently reported on 44 morbidities of interest in patients with RA (online supplemental table 1).4 A confirmation of this list of morbidities and a comprehensive assessment of possible additional morbidities could aid in achieving the goal of unifying the literature on multimorbidity in patients with RA. We aimed to confirm the previously published list of 44 morbidities and comprehensively assess additional morbidities in patients with RA compared with those without RA as well as to determine the appropriate length of the lookback period.
Supplemental material
Methods
The study included residents of eight counties in Minnesota (Olmsted, Dodge, Mower, Goodhue, Wabasha, Freeborn, Steele and Waseca) with prevalent RA on 1 January 2015. The complete inpatient and outpatient medical records for each potential case were manually reviewed by experienced abstractors using the resources of the Rochester Epidemiology Project (REP), and all incident patients fulfilled the 1987 American College of Rheumatology classification criteria for RA.9 For those who moved to the region with pre-existing RA, physician diagnosis with disease modifying antirheumatic drug use was accepted if documentation of criteria fulfilment at the original diagnosis of RA was unavailable. The REP is a unique medical record linkage system that provides complete access to all medical records of all residents of the 27 county region from all local healthcare providers, as described in detail elsewhere.10 11 For each patient with RA, a subject without RA of similar age, sex and county of residency on 1 January 2015 was randomly selected to form the non-RA cohort. This study was approved by institutional review boards of Mayo Clinic (IRB number 17-0 02 593) and Olmsted Medical Center (IRB number 017-OMC-17). Patients and the public were not involved in this study.
Data on demographics, smoking history, body mass index (BMI) and length of medical history (defined as time from first medical contact as a resident of the region to 1 January 2015) were abstracted. Diagnostic codes from all healthcare providers in the counties of interest were retrieved for up to 5 years prior to the prevalence date. Using two codes ≥30 days apart and the list of ICD-9 codes provided by England et al, the 44 morbidities were defined. Obesity was defined as subjects having either two codes ≥30 days apart or having a BMI ≥30 kg/m2 on 1 January 2015. The Clinical Classification Software (CCS) from the AHRQ was used to obtain a comprehensive list of additional morbidities. First, ICD-9 codes without chronic condition indicators were eliminated, which reduced the list from 285 to 190 CCS categories. Second, categories for miscellaneous, residual and other codes were manually examined, and modified subcategories were created for diseases of potential interest, including organic sleep apneoa, polymyalgia rheumatica and eating disorders. Categories for aftercare and medical visits were removed. Third, the CCS category for RA was excluded to ensure comparability between the RA and non-RA cohorts. Similarly, four categories (ie, lupus, connective tissue disease, unspecified autoimmune disorder and polymyalgia rheumatica) that may indicate diagnostic uncertainty prior to RA diagnosis were also removed. Fourth, categories that overlapped with the 44 primary comorbidities were excluded. The resulting 78 categories will be referred to as secondary morbidities. Multimorbidity was defined as the presence of two or more morbidities (MM2+), and substantial multimorbidity was defined as the presence of five or more morbidities (MM5+).
Statistical methods
Descriptive statistics (means, percentages, etc) were used to summarise the data. Comparisons between cohorts were performed using χ2 and rank-sum tests. Logistic regression models adjusted for age and sex were used to estimate an effect size for comparing the prevalence of each comorbidity in those with RA to those without RA. Using all 44 primary plus 78 secondary morbidities, Q values were determined using false discovery rate methods to adjust for multiple comparisons. Q values <0.05 were considered statistically significant. Sensitivity analyses included a comparison of multimorbidity prevalence for a 1-year compared with the 5-year lookback. Obesity was excluded from this sensitivity analysis. Analyses were performed using R V.3.6.2 (R Foundation for Statistical Computing).
Results
The study included 1643 patients with RA and 1643 non-RA subjects (table 1). Both cohorts had a mean age of 63.1 (SD: 14.5) years, were 72% women and 91%–92% white. The median length of prior history (truncated at 5 years) was 5.0 for both cohorts with 96% of RA and 91% of non-RA having a full 5 years of prior medical history.
Characteristics of patients with and without rheumatoid arthritis on 1 January 2015
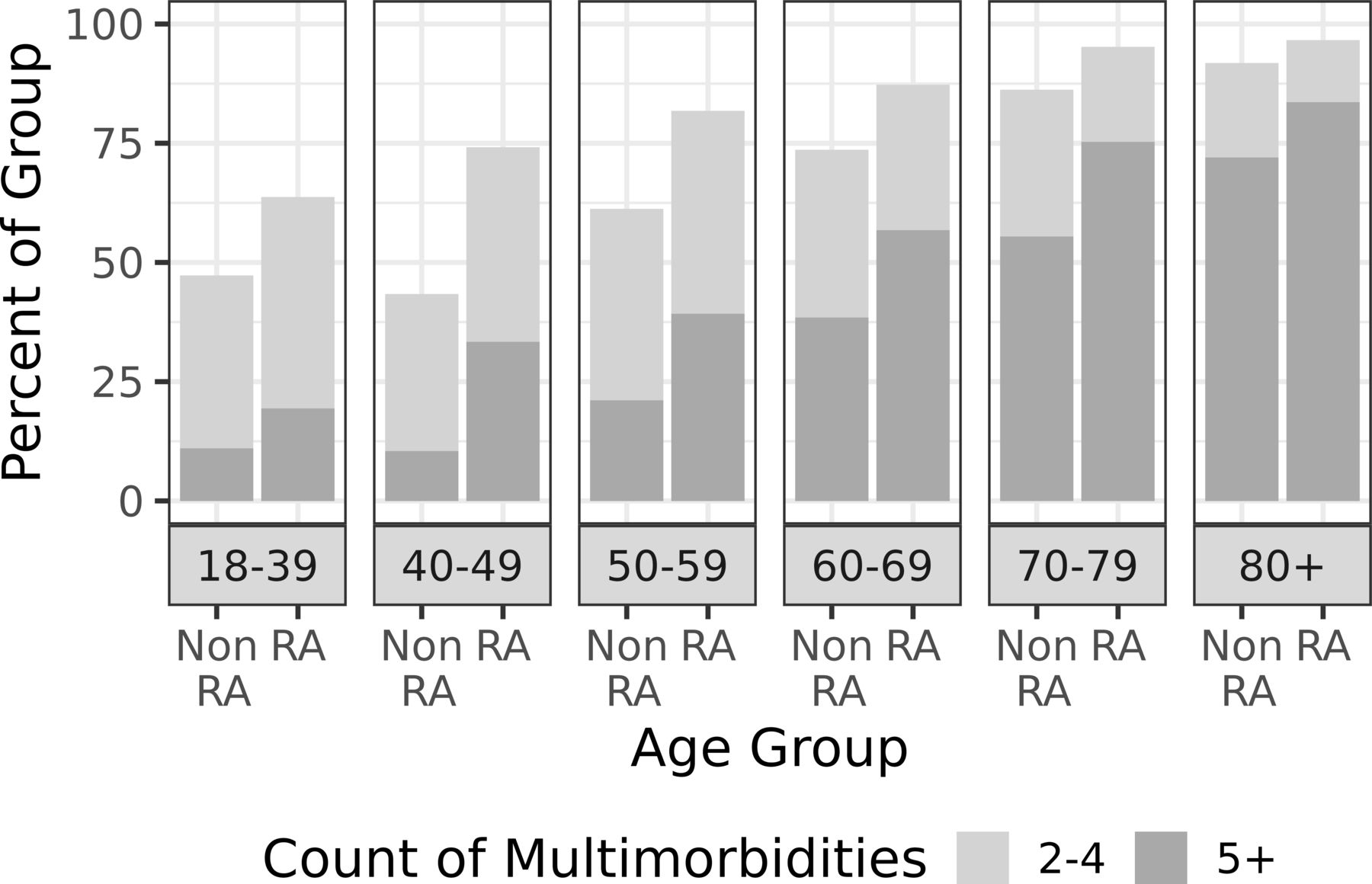
Using the 44 primary morbidities, significantly more patients with RA had MM2+ (1411 (86%) versus 1164 (71%); OR: 2.80; 95% CI 2.33 to 3.38) and MM5+ (907 (55%) vs 619 (38%); OR: 2.37; 95% CI 2.03 to 2.77; table 2). While the absolute levels of MM2+ and MM5+ increased with age, the relative risk of MM5+ comparing RA to non-RA decreased with age from twofold in the youngest age group to 1.2-fold in the oldest age group (figure 1).

The percentage of patients with and without rheumatoid arthritis (RA) who had 2–4 or 5+ morbidities in the primary list of 44 morbidities by age group.
Prevalence of 44 previously published morbidities in patients with and without rheumatoid arthritis
Patients with RA had significantly higher prevalence in 24 of the 44 morbidities compared with non-RA. The morbidities with the greatest increase in prevalence (OR >2.9) in RA compared with non-RA were interstitial lung disease, fibromyalgia, osteoarthritis and osteoporosis. The others included circulatory diseases (ie, cardiac arrhythmias, congestive heart failure, coronary artery disease, hypertension, pulmonary circulation disorders, peripheral vascular disease/aneurysm), respiratory diseases (ie, asthma, chronic obstructive pulmonary disease), anaemia, chronic back pain, depression, drug use, gastrointestinal reflux disease, headache, hypothyroidism, liver disease, neuropathy, skin disorders, inorganic sleep disorders and severe vision reduction. The prevalence was >5% among patients with RA in 11 of the remaining 20 morbidities (ie, anxiety, cancer, diabetes mellitus, gynecologic disorders, hearing loss, prostatic hyperplasia, hyperlipidaemia, obesity, renal disease, cerebrovascular disease and valvular disease), demonstrating their importance, although they were not more common in patients with RA compared with non-RA.
Using only the 78 secondary morbidities, significantly more patients with RA had MM2+ (433 (26%) vs 292 (18%)) and MM5+ (46 (3%) vs 18 (1%)). Combining both the primary and secondary morbidities yielded modest increases in the number of patients with MM2+ (1452 (88%) for all vs 1411 (86%) for primary alone in RA; 1208 (74%) for all vs 1164 (71%) for primary only in non-RA). Likewise, combining both lists increased the number of patients with MM5+ in both cohorts (1014 (62%) for all vs 907 (55%) for primary alone in RA; 725 (44%) for all vs 619 (38%) for primary only in non-RA).
Only 7 of the 78 secondary morbidities were significantly more common in patients with RA than in non-RA: organic sleep disorders, vitamin D deficiency, chronic skin ulcers, foot deformities, thrombocytopenia, leucopenia and other upper respiratory infections (eg, sinusitis)(table 3). Only four additional morbidities had >5% prevalence in patients with RA: hypercalcemia, restless legs, allergic rhinitis and erectile dysfunction (among men).
Prevalence of 78 additional morbidities in patients with and without rheumatoid arthritis
In sensitivity analyses, solid and haematologic malignancies were examined separately. More patients with RA had haematologic cancers (35 (2.1%) vs 21 (1.3%)), but this did not reach statistical significance (OR: 1.69; 95% CI 0.99 to 2.97). In contrast, there was no difference in the occurrence of solid cancers (101 (6.1%) in RA vs 124 (7.5%) in non-RA; OR: 0.80; 95% CI 0.61 to 1.05). Overlap of patients with both solid and haematologic cancers was minimal (3 (0.2%) in RA and 5 (0.3%) in non-RA).
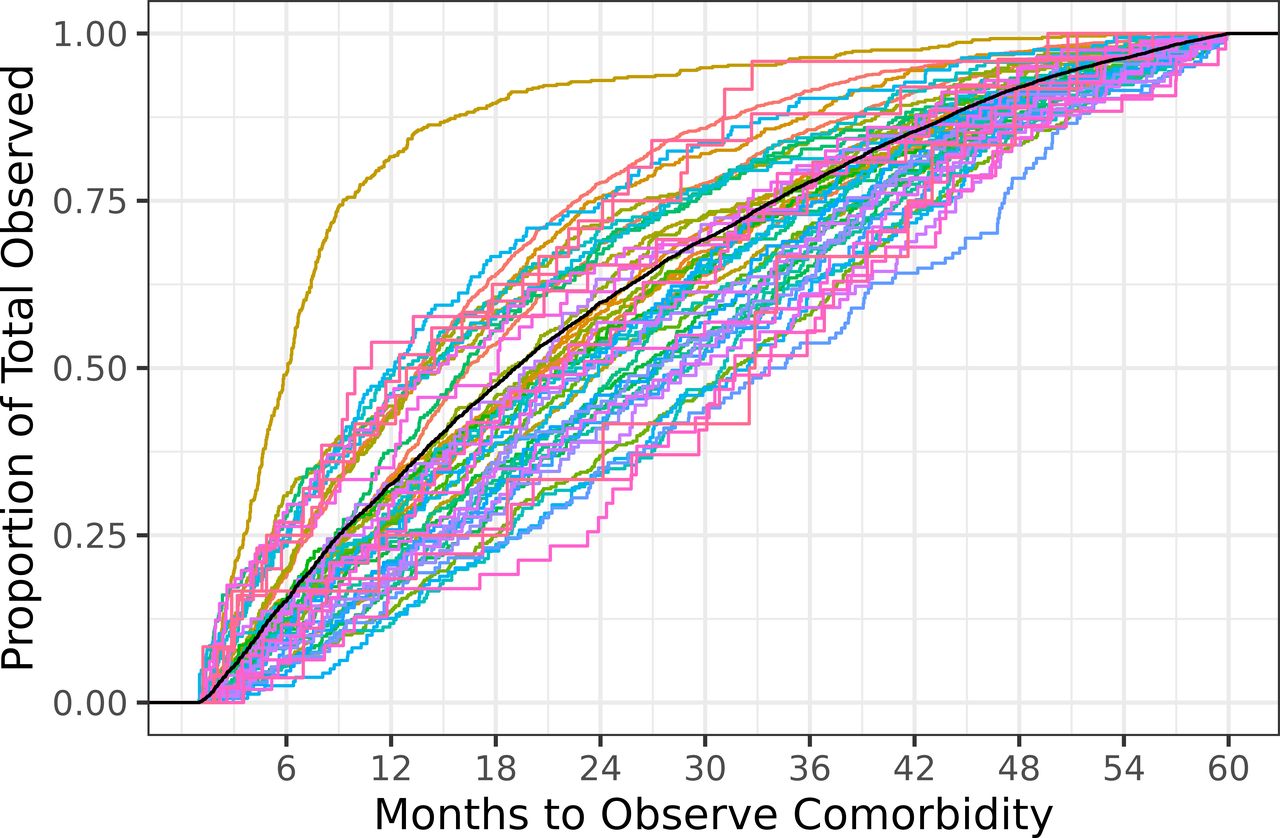
The lookback period to identify morbidities includes both the time from 1 January 2015 back to the first diagnostic code for each morbidity and the time from the first to the second diagnostic code required to define each morbidity. The length of lookback necessary to capture at least 50% of subjects with the comorbidity ranged from 6 to 33 months with an average across all comorbidities of 18 months (figure 2). Only two comorbidities (bipolar disorder and diabetes mellitus) had 50% sensitivity at 12 months and only 14 had 50% sensitivity at 18 months (compared with a 5-year lookback). Comparisons between cohorts showed no evidence of differences in the lookback for all but four of the primary morbidities (ie, hypertension, hypothyroid, osteoarthritis and back problems), which were identified sooner (difference in medians of less than 6 months) in the RA than the non-RA.
{kind=link}
{kind=link}
The proportion of morbidities identified by number of months prior to 1 January 2015 in the combined rheumatoid arthritis (RA) and non-RA cohorts. Coloured lines show each of the 44 primary and 11 additional secondary morbidities; the highest coloured line depicts diabetes, which has a shorter median than the others. The black line shows the overall average, demonstrating that 18 months are needed to identify 50% of these chronic morbidities.
Our final list of recommended morbidities for inclusion in investigation of multimorbidity in patients with RA is listed in online supplemental table 1. These ICD-9/10 code lists will facilitate common definitions across studies.
Discussion
Patients with RA had a higher prevalence of multimorbidity compared with non-RA subjects. These results confirmed the previously published morbidities and identified several additional morbidities of interest in patients with RA including vitamin D deficiency, hypercalcemia, thrombocytopenia, leucopenia, restless legs, sinusitis, allergic rhinitis, erectile dysfunction, skin ulcers, foot deformities and sleep apneoa. Patients with RA were disproportionately affected by multimorbidity at younger ages than their non-RA counterparts. In addition, a 1-year lookback substantially underestimated multimorbidity and a minimum of 2 years is needed to identify most morbidities.
Using the 44 morbidities from England et al, our study found 86% of patients with RA had MM2+, while England et al reported only 34% of patients with RA in a Marketscan commercially insured population had MM2+. In patients with prevalent RA enrolled in Brigham and Women’s Rheumatoid Arthritis Sequential Study (BRASS), Radner et al reported that 62% had MM2+ using a list of 40 morbidities.5 Differences in multimorbidity prevalence are multifocal, including differences in the list of conditions used, the age distribution of the population and the lookback period for identifying morbidities. Adding more conditions can not only increase the percentage of patients with multimorbidity, which may result in a more accurate assessment of multimorbidity burden, but also increase the burden of assessment. Multimorbidity increases dramatically with age, so even small differences in the mean age of the cohorts could lead to very different proportions of patients with multimorbidity. For example, the Marketscan and BRASS had average ages of 56–57 years compared with an average age of 63.5 years in our cohort. Given the average age at RA incidence is 55 years, the average age of a representative prevalence cohort should be older than 56–57 years.12 The Marketscan cohort likely under-represented patients of age ≥65 years with RA, since they were likely on Medicare and were no longer commercially insured. Our study also found that the difference in multimorbidity for RA versus non-RA was more pronounced in younger age groups, and older patients with RA had similar proportions of patients with MM2+ to those without RA. This finding implies that cohorts which underrepresent older ages may exaggerate the overall differences in multimorbidity between patients with and without RA. Regarding lookback period, Yoshida et al argue that some intermittent conditions should use a 1-year lookback period (eg, diverticulitis/diverticulosis and peptic ulcer).6 However, a strict 365-day lookback period may be insufficient for conditions that require yearly renewal of prescription medications, as often intermittent non-adherence extends the prescription supply. Our 5-year lookback was much longer than the average prior history of 1.5 years in the Marketscan cohort. Since the median lookback to identify morbidities using two diagnostic codes was ~2 years for most morbidities, a lookback of 1.5 years might miss over half of the morbidities.
Confirmation of the 44 morbidities used by England et al requires demonstration of increased occurrence in RA compared with non-RA or demonstration that the morbidity affects enough patients to be important. While England et al reported significantly increased occurrence in RA compared with non-RA for 41 of the 44 morbidities in the large Marketscan cohort, the large sample size would easily achieve statistically significant results despite small differences that may not be clinically meaningful. Our study found increased prevalences in 24 of the morbidities and importance (based on 5% prevalence) for 11 additional morbidities. Notably, the lack of an increased prevalence of diabetes is concordant with previous investigations in our cohort, despite reports from other cohorts of increased diabetes prevalence in patients with RA.13 14 The remaining nine morbidities (ie, alcohol abuse, bipolar disease, dementia, diverticulitis/diverticulosis, gout, Parkinson’s disease, post-traumatic stress disorder, peptic ulcer disease and urinary incontinence) were rare and the older age of our cohort may have reduced the magnitude of differences between RA and non-RA. All of these rare conditions are unarguably important, as evidenced by the weights applied to these morbidities in multimorbidity indices designed to predict outcomes (eg, quality of life and mortality).5 15 16 Thus, we retained them. The lack of an increased prevalence of cancer in our cohort was surprising and warrants further investigation to determine whether cancer risk has improved in RA in recent years. We proposed separate categories for solid cancers and haematologic cancers for investigations of biologic mechanisms, but subdivision is not necessary when counting morbidities as few patients have both solid and haematologic cancers.
The majority of the additional morbidities that were found to be increased in RA in our study were already known to be more common in patients with RA (ie, sleep disorders, vitamin D deficiency, chronic skin ulcers and foot deformities).17 18 Some morbidities (ie, thrombocytopenia, leucopenia, other upper respiratory infections) could result from immunosuppression. Importantly, morbidities in patients with RA may result from different underlying mechanisms (eg, RA itself or inflammation, and adverse effects of RA therapies including glucocorticoids and non-steroidal anti-inflammatory drugs) than morbidities in the general population. Additional morbidities with >5% prevalence in patients with RA included hypercalcemia, restless legs, allergic rhinitis and erectile dysfunction (among men).19
Yoshida et al used a multimorbidity index that included 61 conditions collected in the Nurses’ Health Studies.6 Additional morbidities considered by Yoshida et al included several non-chronic conditions (ie, colon polyp, hepatitis not specified as chronic, pancreatitis, interstitial cystitis, kidney stones, hip and vertebral fractures and hip and knee replacements), several rare conditions that did not meet our criteria of increased occurrence in RA or >5% prevalence in RA (ie, inflammatory bowel disease, acquired immune deficiency syndrome, amyotropic lateral sclerosis, multiple sclerosis, and seizure disorder), periodontal disease and ‘other diagnoses’. Additional conditions considered by Radner et al were learning disability, anorexia/bulimia, chronic sinusitis, constipation and dyspepsia. Chronic sinusitis was increased in RA compared with non-RA in our study, and constipation approached our threshold at 4.5% in RA. Our study provides the first comprehensive assessment of all chronic conditions identified by AHRQ in a population-based cohort of patients with RA.
This study has multiple strengths, including the population-based cohorts of patients with RA and non-RA, the comprehensive resources of the REP that capture all medical care from all providers in the community and the long length of prior medical history to assess comorbidities. Limitations include the use of diagnostic codes to define morbidities and the retrospective study design. Only diagnoses that came to medical attention and were documented in the medical records were included. While the frequency of medical visits may differ in RA compared with non-RA, the focus on chronic morbidities minimises the risk of missing morbidities of interest in those with fewer medical visits. However, periodontal disease, sarcopenia and cachexia are known to have increased prevalence in patients with RA but were only diagnosed in a few patients in our cohorts. Furthermore, the accuracy of coded diagnoses can be suboptimal. For this reason, we excluded four categories that may overlap with RA due to diagnostic uncertainty (ie, lupus, connective tissue disease, hypergammaglobulinemia and polymyalgia rheumatica). Prospective studies with careful adjudication of morbidities may retain these other rheumatic diseases, but co-occurrence of RA and another rheumatic disease is rare.6 Standard procedures used in administrative claim studies, such as requiring two codes at least 30 days apart, were used to improve reliability of the coded diagnoses.4 In addition, severity of various morbidities and the impact of morbidities on outcomes of interest (eg, quality of life, mortality) have not been assessed. Finally, the limited diversity in the Olmsted County population (90% Caucasian) may limit generalisability of these findings to more diverse populations.
In conclusion, patients with RA have a higher prevalence of multimorbidity compared with non-RA subjects that may have been underestimated in other studies that focused on a younger RA population or had a limited lookback period to identify chronic morbidities. These results confirm the previously published list of 44 morbidities and add several other morbidities of interest in RA. Focusing on the patient-centric viewpoint of multimorbidity investigations, it is clear that the majority of patients with RA are dealing with multiple chronic conditions. These conditions impart a substantial burden of healthcare concerns and make healthcare decision-making more challenging than in patients without RA. Therefore, there is an increasing need for improved coordination of healthcare between multiple providers and for care models that provide support for addressing multimorbidity in patients with RA. This comprehensive assessment of morbidities in RA can help to unify the literature on multimorbidity to help move this field forward. Further research is needed to assess the impact of morbidities on various outcomes, such as quality of life and mortality.
Data availability statement
Data are available upon reasonable request. Mayo Clinic Institutional Review Board (IRB) policy does not allow full access of patient information to be provided to a third party without prior approval from the IRB committee overseeing this study. However, access to the complete de-identified data can be made available following approval. Requests for additional study-related data can be sent to Cynthia S. Crowson at crowson@mayo.edu.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by This study was approved by institutional review boards of Mayo Clinic (IRB number 17-002593) and Olmsted Medical Center (IRB number 017-OMC-17). Informed consent was not required. Patients provided authorization for use of their medical records for research purposes.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @CrowsonCindy, @KronzerMD
Contributors Conceived and designed the experiments: CSC, EM, JMD. Performed the experiments: CSC, TMG, HJD, EM, EJA, VLK, CMC, JMD. Analysed the data: CSC, TMG, HJD, EJA. Wrote and revised the paper: CSC, TMG, HJD, EM, EJA, VLK, CMC, JMD. Guarantor: CSC.
Funding This work was funded by grants from the National Institutes of Health, NIAMS (R01 AR46849) and NIA (R01 AG068192). Research reported in this publication was supported by the National Institute of Aging of the National Institutes of Health under Award Number R01AG034676. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.