Article Text

Abstract
Objectives To estimate the frequency of reporting composite indices evaluating axial spondyloarthritis (axSpA) disease activity in daily practice and to assess its impact on the secukinumab (SEC) retention rate.
Methods Study design: Retrospective, multicentre. Data collected: (1) Recommended composite indices: Bath Ankylosing Spondyltitis Disease Activity Index (BASDAI) +C reactive protein or Ankylosing Spondylitis Disease Activity Score (ASDAS) at the time of initiation of SEC and at least once during the first year of follow-up; (2) Drug retention rate: percentage of patients still on SEC over time according to whether at least one recommended composite index had been optimally reported.
Results A recommended composite index has been collected in 22% of the 906 enrolled axSpA patients. The percentage of patients still on treatment after 1, 2 and 3 years of follow-up was greater in those for whom at least one composite index had been optimally reported (respectively, 64% (57–71) vs 57% (54–61), 55% (48–62) vs 41% (38–45) and 52% (44–59) vs 38% (34–42), log rank test, p=0.016) with a lower risk of SEC discontinuation for these patients (HR: 0.70 (95% CI 0.5 to 0.88), Cox model, p=0.003).
Conclusion This study suggests that reporting of recommended composites indices for monitoring axSpA might be associated with higher retention rates of biological therapies.
- spondylitis
- ankylosing
- outcome and process assessment
- health care
- quality indicators
- health care
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
International and national scientific societies strongly recommend the collection and the report in the patients’ medical files of validated composite indices evaluating disease activity of axial spondyloarthritis.
Previous studies have suggested a low-report of these indices in daily practice.
What does this study add?
This study confirms the low reporting of these composite indices.
This study shows a link between the report of these composite indices and a better retention rate of biologics suggesting that the report of these composite indices might be considered as a marker of Good Clinical Practice.
How might this impact on clinical practice?
The data observed in this study might be an argument to convince the rheumatologists to collect and report these composites indices in their daily practice.
Introduction
Recommendations from international scientific societies advocate for a regular monitoring of disease activity in patients suffering from chronic inflammatory rheumatic diseases and, in particular, axial spondyloarthritis (axSpA).1–3 The recommendation is to evaluate periodically composite indices reflecting optimally the level of disease activity (eg, BASDAI +C reactive protein (CRP) or ASDAS) for axSpA4–6 and even more frequently in case of an active disease necessitating the initiation of a biological disease modifying anti-rheumatic drug (bDMARD). These recommendations are mainly based on evidence showing that high disease activity is one of the main predisposing factors of subsequent structural progression and negative impact on the functional status of the patients.7–9
Although this recommendation is obviously strictly followed in the context of clinical trials, there is a huge gap in its implementation in daily practice.10 11 One of the reasons of this gap might be the lack of clear evidence at the individual level that the assessment and reporting in the medical records of these disease activity outcome measures are of real benefit for the patients. However, it is quite challenging to show that there is such benefit. One might consider that a positive strategy trial in which the treatment decision is driven by the value of a composite index (eg, the assessment of ASDAS in the TIght COntrol in SPondyloArthritis (TICOSPA) trial12) is an argument for the assessment and reporting of these composite indices in daily practice. However, one could also debate that the results of these strategy trials have been obtained in a quite rigorous clinical context and are mainly driven by the intensification of the treatment in case the value of the composite index is above a certain threshold (e., an ASDAS value >2.1 in the TICOSPA trial).
Data from daily practice might be more relevant at least in countries/regions/settings where such assessments and reporting are not mandatory and/or not financially supported by health authorities, which is the case for France. Moreover, the definition of a ‘benefit at the individual level’ is also challenging. When evaluating the use of bDMARDs, one might consider that the retention rate to therapy over time is reflecting a better effectiveness of the respective bDMARD.13–17
These considerations prompted us to evaluate the impact of reporting disease activity outcome measures in the medical files of axSpA patients on drug retention rate by exploring the data on the use of secukinumab (SEC) in daily practice in France.18
Patients: methods
Study design
This was a retrospective, multicentre study conducted in France. In order to avoid a bias due to the non evaluation of patients who had to stop their treatment very soon after its initiation, we have included in this initiative only the centres (47 out of the 54 selected centres) who were able to provide an exhaustive list (issued from their electronic health record system or from their own specific databases) of their patients for whom a treatment with SEC has been initiated between August 2016 and August 2018. For each patient, the information collected in their medical records has been captured by either a physician/ research nurse of the centre or by an independent clinical research assistant. Four categories of information have been collected in relation to (1) the centre (eg, number of patients enrolled) (2) SEC treatment and in particular its line of administration as a bDMARD, the date of initiation and discontinuation (3) the patients: demographics (age, gender), disease duration, presence of objective sign of inflammation, (either increased CRP or presence of MRI-SIJ/spine inflammation), past or present extra spinal and extrarheumatological manifestations and (4) the composite indices: BASDAI, CRP and ASDAS at baseline and 3±1, 6±2, 12±2 months later and also during the second year of follow-up or elements permitting their calculation.
Statistical analysis
Optimal report was predefined as reporting of a recommended composite index evaluating the axSpA disease activity in the medical records at the time of the initiation of SEC and at least once during the first year of follow-up. The percentage of patients still on treatment over time was estimated by the Kaplan Meier method and then was compared with the predefined optimal report of the recommended composite indices by log rank test.
Preselected predictive factors of the SEC retention rate which have been investigated were, apart from the predefined optimal report of a recommended composite index, size of the centre (<10 vs ≥10 enrolled patients), age (above vs below the median of 46 years), sex, HLA B27 positive versus negative, diagnosis of non-radiographic versus radiographic SpA, past or present uveitis confirmed by an ophthalmologist, past or present inflammatory bowel disease/psoriasis/arthritis or synovitis/enthesitis diagnosed by a physician, disease duration above vs below the median of 6.4 years, presence of at least one objective sign of inflammation, SEC line of biological therapy (1st/2nd vs ≥3rd line).
Predictive factors with less than 20% of missing data have been entered in a multivariate model using a stepwise selection (significance level for entering variables=20%; significance level for removing variables=10%).
For factors with less than 20% of missing data, a multiple imputation approach was applied using the method developed by Rubin.19 Smoking, Body mass index and objective sign of inflammation were not included in the model because of a percentage of missing data above the a priori defined threshold of 20%. The variable « sex » was excluded during the stepwise regression analysis because of a p>0.10.18
Results
In total, SEC was initiated in 906 axSpA patients in the 47 participating centres.
The report of at least one recommended composite index was documented only in 22% of the patients with a higher frequency of BASDAI +CRP than the ASDAS composite index (18% vs 12%, respectively). During the first year of follow-up, one recommended composite index was documented in 35%, 17%, 18% and 12% at baseline, 3±1, 6±2 and 12±2 months later. During the second year, this reporting was also documented at least once in 14%.
The characteristics of the patients with regard to the optimal report of the recommended composite indices are summarised in table 1.
Baseline characteristics of axSpA patients treated with secukinumab with regard to the optimal report of a recommended composite index
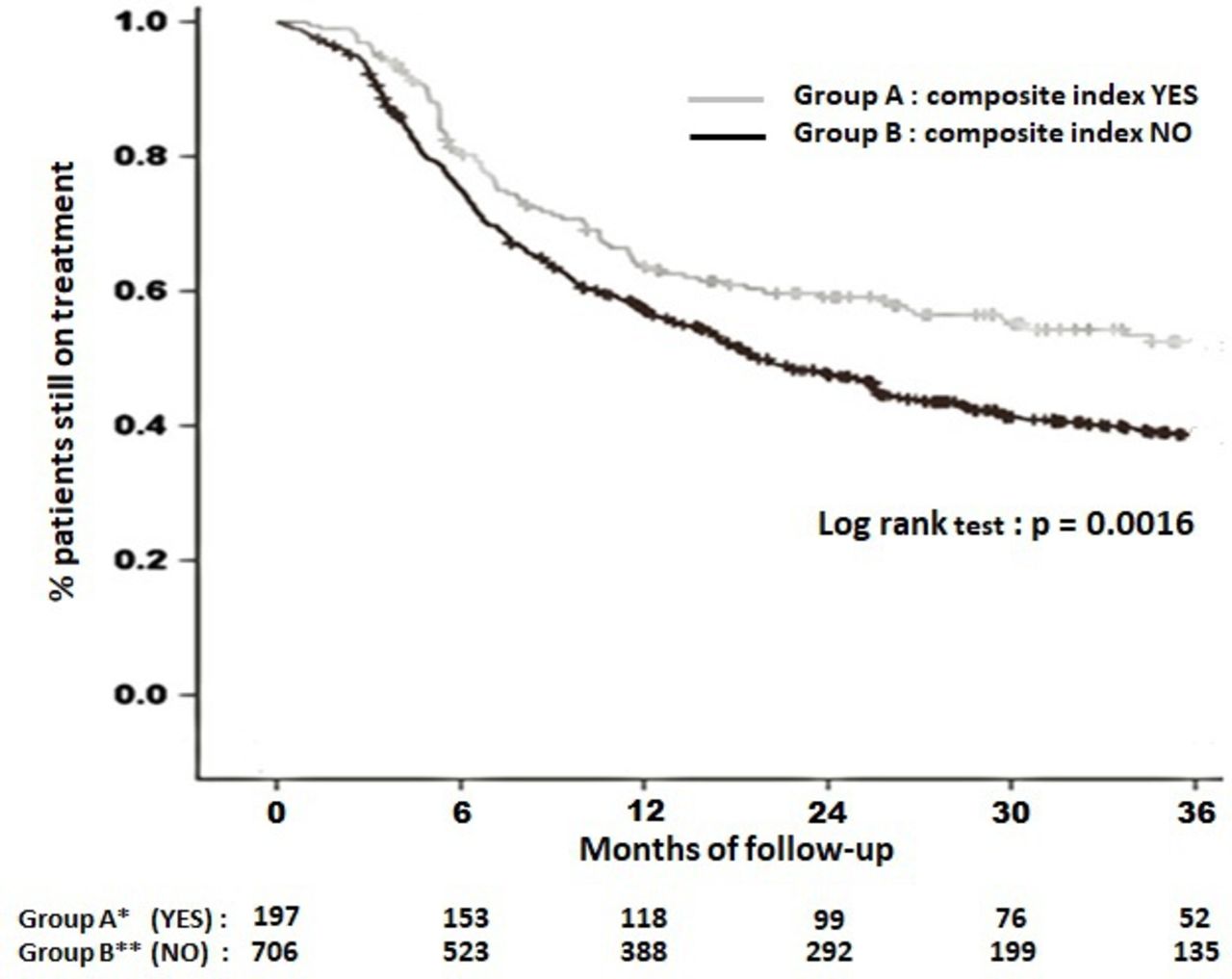
During the study, the estimated percentage of patients who had to discontinue the drug was 29%, 38%, 40% vs 8%, 9%, 10% and vs 39%, 51%, 53% after 1, 2 and 3 years of follow-up because of inefficacy vs side effect and vs any reason respectively.The retention rate of SEC according to the optimal report of a recommended composite index is depicted in figure 1. The estimated percentage of patients still on treatment over time was higher in the group of patients with an optimal report of a recommended composite index in comparison to the group with no optimal report with the following percentages after 1, 2 and 3 years of follow-up: 64% (57–71) vs 57% (54–61), 55% (48–62) vs 41% (38–45) and 52% (44–59) vs 38% (34–42), respectively; log rank test (p=0.0016).
{kind=link}
Secukinumab retention rate according to the optimal report of a composite index evaluating axial spondyloarthritis disease activity. Group YES*=Patients for whom a composite index (either (Bath Ankylosing Spondylitis Disease Acttivity Index (BASDA)I +CRP) or Ankylosing Sondylitis Disease Avtivity Score (ASDAS)) has been optimally (at the time of the initiation of secukinumab and at least once during the first year of follow-up) reported. Group NO*: Patients for whom a composite index (either (BASDAI +CRP) or ASDAS) has not been optimally (at the time of the initiation of secukinumab and at least once during the first year of follow-up) reported. */** Values given at the bottom of the figure are the number of patients at risk at the beginning of each interval in each study group. CRP, C reactive protein.
As shown in table 2, the multivariate analysis (Cox model) confirms that the optimal report of a composite index is an independent factor associated with a lower risk of discontinuation of SEC: (HR=0.70 (95% CI 0.55 to 0.88), p=0.003).
Predisposing factors of discontinuation of secukinumab
Discussion
Optimal report in the medical records of the recommended composite indices evaluating axSpA disease activity was documented for a low percentage of patients in accordance with previous reports10 11 conducted in France, further highlighting the difficulties the scientific community is facing when trying to implement recommendations in daily practice.20 This low reporting rate of recommended composite indices is difficult to explain. One should keep in mind that this report in France is not mandatory and not financially supported by the French health authorities. Another explanation might be that these composite indices have been collected (eg, in a paper format) but not reported in the electronic health record of the patients.
More importantly, optimal report was found to be associated with a better outcome in terms of bDMARD retention rate. Overall, the retention rate of SEC observed in this study is also consistent with previous similar studies conducted in daily practice in western European countries.15
This study has several strengths but also some weaknesses. First, the study was conducted in a country where the collection and reporting of these outcome measures are highly recommended but neither mandatory nor financially supported. Although this setting allowed to optimally answer the research question, the results cannot be generalised to another country. For example, in a country where health authorities are making mandatory these measures before the initiation of biologics, rheumatologists have to report them, anyway. Additionally, the results should have been different in case financial support would have been provided to the rheumatologist reporting these outcome measures.
Another strength of this study is the fact that, a priori, there was no link between the evaluated parameter (eg, the report of the composite index) and the outcome (eg, the SEC retention rate). As others,13–17 we postulated that the retention of a biotherapy might be a relative marker of its effectiveness, and hence the use of SEC in daily practice right after its launch in France18 was a suitable setting to perform this analysis. Although a priori there is no link between the outcome and the independent variable, it should be pointed out that the independent variable (eg, the composite index) contains elements that the clinician can use to assess the efficacy or to decide on the continuation of the drug. So our results argue in favour of the report of a composite index as a marker of good clinical practice. On the other hand, the retention rate of a drug is a complex equation in which many variables come into play as the type of drug, the patient, the disease suffered, etc that the physician has to deal with. Therefore, the results that we observed in this study may give us more clues on the physician (observed bias) who initiated the drug and how she/he managed it than on the true efficacy/safety profile of the drug. Therefore, the choice of this outcome might also be seen as a weakness since other outcome measures such as the impaired functioning or quality of life would have been considered as more relevant. However, this information is rarely collected and reported in daily practice.9
In summary, our study suggests that the assessment and report of recommended outcome measures evaluating the axSpA disease activity might be an argument of a Good Clinical Practice resulting in better outcomes for the patients. Other studies using different study designs and conducted in other environments are required to confirm these results.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants but was not approved by In accordance with the Good Clinical Practices in France, for this kind of study (retrospective collection of information contained in the medical files of the patients), there is no need of an approval of an ethic committee. Participants gave informed consent to participate in the study before taking part.
References
Footnotes
Contributors MD is the principal investigator of the study and designed this ancillary analysis with the help of the other members of the scientific committee (CL, AS, AT, AR-W, DW, PG and PC) ED is the coordinator of the study and participated actively at this ancillary analysis, JL was the biostatistician in charge of the analysis of this ancillary analysis.
Funding NOVARTIS Pharma France financially supported this study.
Competing interests The principal investigator (MD) and the members of the scientific committee of the study (CL, AS, AT, AR-W, DW, PG and PC) have received honorarium fees from NOVARTIS Pharma, France. ED, the study coordinator is an employee of NOVARTIS Pharma France. JL is an employee of RcTs the company in charge of the monitoring of the study and its statistical analysis, this company had a financial contract with NOVARTIS Pharma France.
Provenance and peer review Not commissioned; externally peer reviewed.