Article Text

Abstract
Background A positive family history (PFH) of spondyloarthritis (SpA) consists of five SpA-related entities, of which a PFH of axial spondyloarthritis (axSpA) is most common in European patients with axSpA. Moreover, a PFH of axSpA is associated with human leucocyte antigen B27 (HLA-B27) positivity in these patients. It is unknown if this holds true in patients with axSpA in other parts of the world.
Objective To investigate the geographical prevalence of a PFH of SpA and its association with HLA-B27 positivity in patients with axSpA worldwide.
Methods Cross-sectional analyses included patients from the ASAS peripheral involvement in Spondyloarthritis (PerSpA) study from 24 countries worldwide with an axSpA diagnosis, known HLA-B27 status and family history. Logistic regression models were built to assess the effect of HLA-B27 status on the occurrence of PFH. This was repeated for each of the five SpA entities in a PFH.
Results Among 2048 patients, axSpA was the most common SpA entity in a PFH in all geographical regions (Asia 28%, Europe and North America 27%, Latin America 20%, Middle East and North Africa 41%). A PFH of axSpA was associated with HLA-B27 positivity in Asia (OR 4.19), Europe and North America (OR 2.09) and Latin America (OR 3.95), but not in the Middle East and North Africa (OR 0.98), which has a lower prevalence of HLA-B27 positivity. A PFH of other SpA entities was less prevalent and not consistently associated with HLA-B27 positivity.
Conclusion In patients with axSpA worldwide, axSpA was consistently the most common SpA entity in a family history and was associated with HLA-B27 positivity in all geographical regions but one.
- spondylitis, ankylosing
- epidemiology
- patient reported outcome measures
Data availability statement
No data are available. For this study we used data from the ASAS-PerSpA data set. Therefore we kindly refer interested parties to the first author of the original ASAS-PerSpA publication.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
In patients with axial spondyloarthritis with a positive family history, a positive family history of axial spondyloarthritis is the most common.
What does this study add?
Worldwide, in axial spondyloarthritis, the association between positive family history and HLA-B27 is largely driven by family history of axial spondyloarthritis.
A positive family history of uveitis, psoriasis, inflammatory bowel disease and reactive arthritis was less common and not consistently associated with HLA-B27 carriership in patients with axial spondyloarthritis across the globe.
How might this impact on clinical practice or further developments?
Future research should focus on a refined definition of a positive family history in patients with axial spondyloarthritis.
Introduction
The Assessment in SpondyloArthritis international Society (ASAS) has defined a positive family history (PFH) of spondyloarthritis (SpA) as a family history of axial spondyloarthritis (axSpA), psoriasis, reactive arthritis (ReA), acute anterior uveitis (AAU) or inflammatory bowel disease (IBD) in a first-degree or second-degree relative,1 and in this definition no distinction has been made between a PFH of axSpA or a PFH of another SpA entity (ie, psoriasis, ReA, AAU or IBD).
PFH can be used for different purposes: (1) as one of the clinical criteria in the ASAS classification criteria; (2) as a proxy for human leucocyte antigen B27 (HLA-B27) positivity in situations where HLA-B27 testing is not useful or not possible; and (3) as a risk factor for the development of axSpA.
The definition of PFH was based on consensus of experts and was not tested nor validated prior to its use as one of the SpA features and inclusion in the ASAS classification criteria for axSpA. Data from predominantly Western European cohorts have shown that in patients with axSpA the most common SpA entity in a family history is axSpA. Additionally, an association between PFH and HLA-B27 positivity was found. This association was driven by a PFH of axSpA and possibly AAU, but not by other SpA entities.2 3 While PFH has been regarded useful for identifying patients with back pain at risk of axSpA, research has shown that the diagnostic value of PFH is limited once the HLA-B27 status is known.4 However, these studies were limited to mostly Western European patients.
These findings suggest that, in the currently used classification criteria for axSpA, PFH may be overvalued—as both HLA-B27 and PFH are similarly weighted—and that its definition is likely too broad by including five SpA entities when classifying patients for scientific research. Furthermore, as axSpA was the most prevalent SpA entity and the association between HLA-B27 and PFH was driven by axSpA, the current definition of PFH might be too broad for identifying at-risk patients. Should the definition of PFH be revised in the future, a new definition must be applicable to patients all around the world. Additionally, it should be tested in different settings, as a different definition may be required for the different purposes described above. As PFH was defined based on experts’ opinion, the first step is to investigate the prevalence of PFH in each geographical region. Thereafter, it should be investigated whether the same association between PFH and HLA-B27 positivity exists in other parts of the world (eg, Latin America or Africa).
The ASAS peripheral involvement in Spondyloarthritis (ASAS-PerSpA) study was conducted in 24 countries around the world and provides a unique opportunity to verify the findings of previous research in populations outside of Western Europe. The availability of worldwide data on PFH provides a unique opportunity to assess the prevalence of PFH in various geographical regions, including populations outside of Western Europe. Furthermore, the worldwide representation of patients in the ASAS-PerSpA study allows us to investigate the association between PFH and HLA-B27 across the globe. With this study, we aim to assess whether the association between PFH and HLA-B27 that was found in previous research applies to patients outside of Western Europe. Additionally, we aim to investigate whether this association is driven by a specific SpA entity.
Materials and methods
Data from the ASAS-PerSpA study were used in this study, of which detailed information can be found in the original publication.5 In brief, ASAS-PerSpA was an observational study conducted in 24 countries around the world, in which data were collected cross-sectionally between 1 March 2018 and 29 February 2020. The countries were grouped in four geographical regions identical to the original publication: (1) Asia, (2) Europe and North America, (3) Latin America and (4) Middle East and North Africa (see online supplemental table S1). Its primary aim was to assess the prevalence of clinical peripheral rheumatological features in consecutively included patients with a diagnosis of SpA worldwide and to evaluate the validity of outcome measures of peripheral rheumatological features.5
Supplemental material
Patients
For our analyses only patients with a definite axSpA diagnosis, as defined by the treating rheumatologist, from the ASAS-PerSpA study were included (radiographic or non-radiographic axSpA).
Patients included in this study had to have a known family history according to the ASAS definition1 and a known HLA-B27 status. If information on family history of more than two of the five SpA entities was missing for both first-degree and second-degree relatives, or if family history in first-degree relatives was missing for all SpA entities, family history was considered unknown and patients were excluded (online supplemental table S2 provides insight into the proportion of missing information for each SpA entity). However, if a complete family history of all five SpA entities was available for first-degree relatives only, patients were not excluded. Written informed consent was obtained from participants prior to inclusion.
Outcomes
The primary analysis of this study was to assess family history in all included patients diagnosed with axSpA and stratified by geographical region. The ASAS definition was used to define a PFH of SpA1; the presence of axSpA, AAU, psoriasis, IBD and/or ReA in first-degree or second-degree relatives was considered as a PFH. In this definition, parents, siblings and children are defined as first-degree relatives and maternal and paternal grandparents, aunt, uncle, niece and nephew as second-degree relatives. In this study, family history was analysed as a PFH of any SpA entity (ie, according to the ASAS definition) as well as a PFH of each specific SpA entity (ie, axSpA, AAU, psoriasis, IBD and ReA). Additionally, the association between a PFH of an extra-musculoskeletal manifestation (EMM) and presence (current or past) of the same EMM was also investigated. PFH was not split according to first-degree or second-degree relatives in the current study.
Other outcomes of interest were (1) the association between HLA-B27 positivity and family history; and (2) whether the association between HLA-B27 positivity and a family history of a specific SpA entity (eg, axSpA) was independent of a family history of the other four SpA entities.
Finally, we aimed to compare the prevalence of PFH in the PerSpA cohort with the prevalence of PFH in patients diagnosed with axSpA and patients with chronic back pain in the ASAS, DESIR DEvenir des Spondyloarthropathies Indifférenciées Récentes) and SPACE (SPondyloArthritis Caught Early) cohorts. Herein, descriptive statistics were used to compare the prevalence of PFH among HLA-B27-positive and HLA-B27-negative patients with an axSpA diagnosis in the PerSpA study with the prevalence of PFH in patients from the other (ax)SpA cohorts.1 6–8
Statistical analyses
The prevalence of PFH of all five SpA entities combined but also for each SpA entity separately was determined among all included patients, as well as stratified by HLA-B27 status per geographical region. Separate logistic regression models were used to assess the association between HLA-B27 status and each SpA entity in PFH in the total included axSpA population as well as stratified for each geographical region. Finally, multivariable logistic regression models were built to investigate if a family history of each specific SpA entity was associated with HLA-B27 positivity, independently of the other four SpA entities. These multivariable models were built for the total included study population as well as stratified per geographical region. In the models investigating the association of a PFH of axSpA and HLA-B27 positivity, a PFH of AAU, psoriasis, IBD and ReA was included as covariates.
Results
Of the 2675 patients in the ASAS-PerSpA study diagnosed with radiographic or non-radiographic axSpA, 627 patients were excluded due to unknown HLA-B27 status (n=546) or unknown family history (n=81), as defined a priori. For the current analysis a total of 2048 patients from four geographical regions (Asia n=545, Europe and North America n=840, Latin America n=202 and Middle East and North Africa n=461) were included (online supplemental table S1). The median (IQR) age of the patients was 40 (31–50) years, 31% were female, with a median disease duration of 11 (5–20) years and a mean (SD) of 3 (2) SpA features (online supplemental table S3). Overall, there were only a small percentage of missing data (<5% unless indicated otherwise).
HLA-B27 positivity was 89% in Asia, 65% in the Middle East and North Africa, 78% in Europe and North America and 81% in Latin America. Patients in Latin America more often had concomitant peripheral symptoms—as shown by the higher proportions of peripheral arthritis, enthesitis and dactylitis compared with the other geographical regions—whereas psoriasis was more common in Europe and North America. Uveitis was the most common EMM and there was a significant association between a PFH of EMM and current or past presence of the same EMM in patients with axSpA: psoriasis: OR 4.95 (95% CI 3.43 to 7.13, p<0.001); AAU: OR 2.91 (95%CI 1.83 to 4.64, p<0.001); and IBD: OR 5.17 (95% CI 2.72 to 9.81, p<0.001).
Prevalence of family history by geographical region
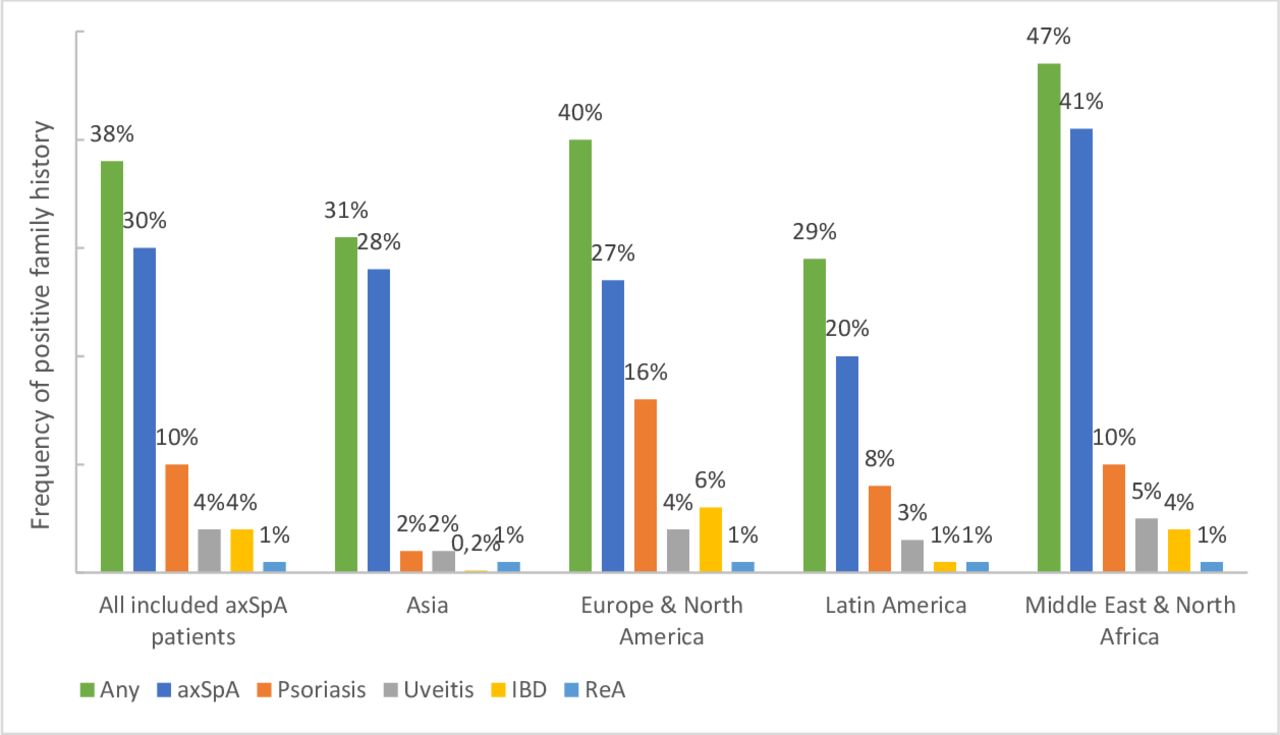
A PFH of any of the SpA entities was most common in the Middle East and North Africa compared with the other geographical regions, which was largely due to a PFH of axSpA (figure 1). Across all geographical regions, a PFH of psoriasis was the second most common entity in a family history and a PFH of IBD, uveitis and ReA was uncommon.

Frequency of a positive family history (any and for each SpA entity) stratified by geographical region. axSpA, axial spondyloarthritis; IBD, inflammatory bowel disease; ReA, reactive arthritis.
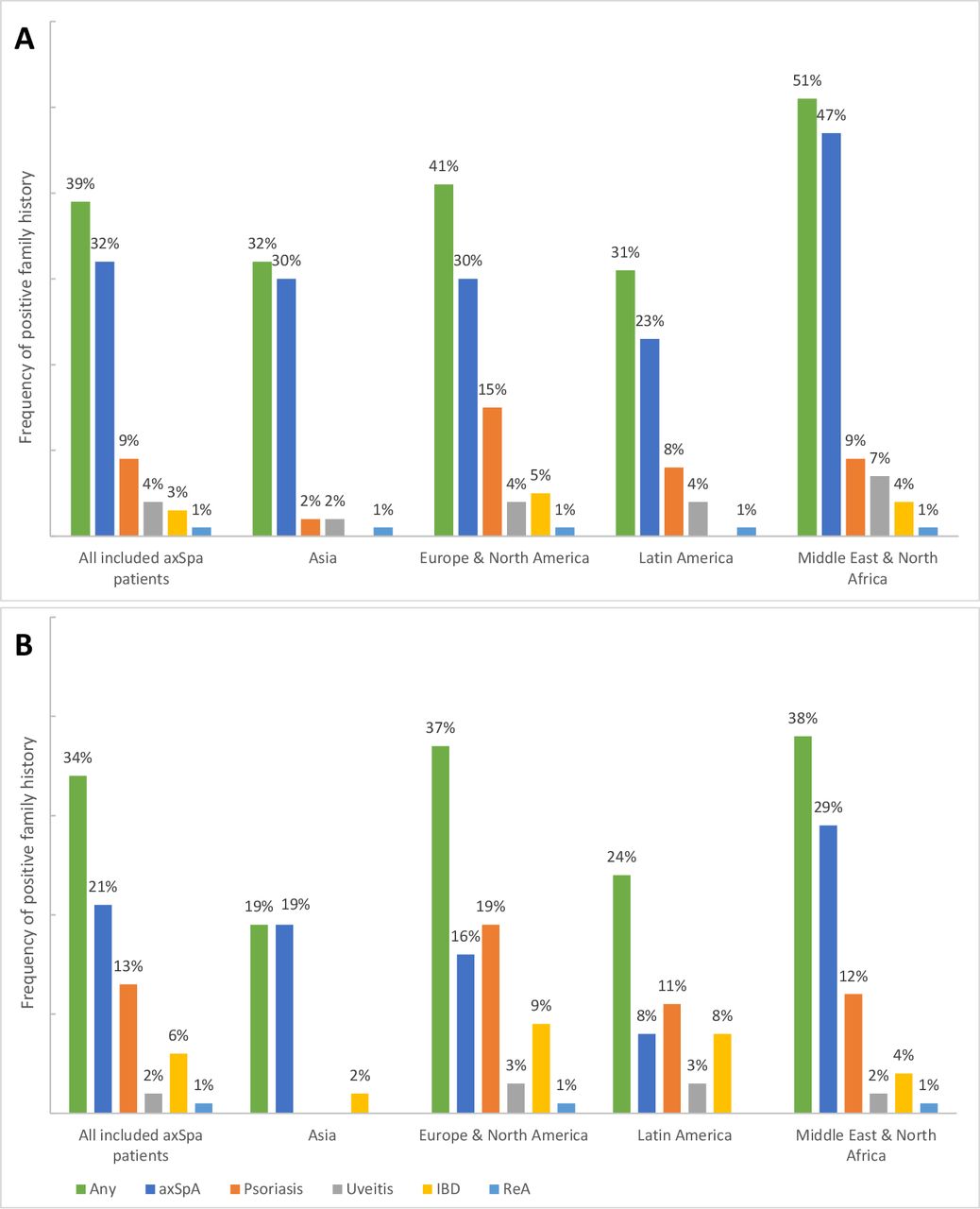
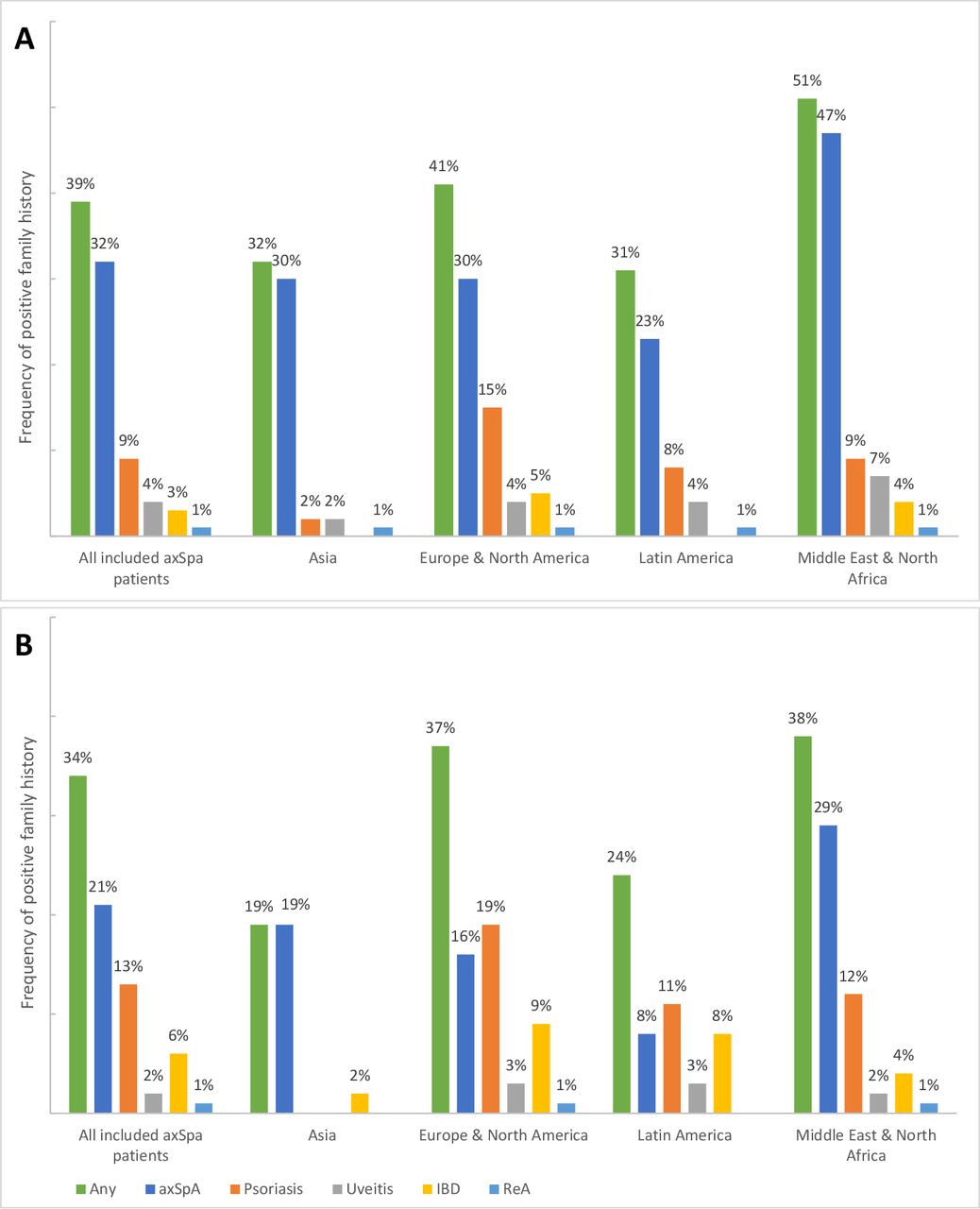
Similar results were found when the data were stratified on HLA-B27 status (figure 2 and table 1); a PFH of axSpA was the most common regardless of HLA-B27 status in each geographical region, except for HLA-B27-negative patients in Europe and North America and Latin America in whom a PFH of psoriasis occurred the most. A PFH of psoriasis and IBD occurred more frequently in HLA-B27-negative patients than in HLA-B27-positive patients in all geographical regions.
{kind=link}
{kind=link}
Frequency of a positive family history (any and per disease) stratified by geographical region for HLA-B27-positive (A) and HLA-B27-negative (B) patients with axSpA. axSpA, axial spondyloarthritis; HLA-B27, human leucocyte antigen B27; IBD, inflammatory bowel disease; ReA, reactive arthritis.
Frequency of positive family history among patients with axSpA in the ASAS, DESIR, ASAS-PerSpA and SPACE cohorts
Prevalence of PFH compared with other cohorts
We compared the prevalence of PFH found in the ASAS-PerSpA cohort with those in HLA-B27-positive and HLA-B27-negative patients with an axSpA diagnosis and patients with chronic back pain (ie, no axSpA diagnosis) in other axSpA cohorts. Table 1 shows that a PFH of each specific SpA entity occurs in both HLA-B27-positive and HLA-B27-negative patients diagnosed with axSpA. This was not only apparent in the ASAS-PerSpA cohort, but also in the ASAS, DESIR and SPACE cohorts. Furthermore, across all cohorts the prevalence of a PFH of axSpA and uveitis was higher in HLA-B27-positive patients, whereas the prevalence of a PFH of psoriasis and IBD was higher in HLA-B27-negative patients. The ASAS and SPACE cohorts also show that a PFH of almost all SpA entities is present in similar frequencies among patients with chronic back pain suspected of axSpA who were eventually not diagnosed with axSpA.
Association between HLA-B27 positivity and family history
Univariable logistic regression models showed a positive association between HLA-B27 positivity and a PFH of axSpA in the total included axSpA population (OR 1.84) and when stratified by region, in Asia (OR 4.19), Europe and North America (OR 2.09) and Latin America (OR 3.95), but such an association was not found in the Middle East and North Africa (OR 0.98; table 2). A negative association with HLA-B27 was found for patients with a PFH of IBD in Europe and North America (OR 0.52) only; for patients with a PFH of psoriasis, such an association was found in the Middle East and North Africa (OR 0.39) only. No associations between HLA-B27 positivity and a PFH of uveitis and ReA were found.
Univariable associations between HLA-B27 and positive family history stratified by geographical region
Multivariable model
Multivariable logistic regression models showed that a PFH of axSpA was positively associated with HLA-B27 positivity independent of the presence of a PFH of other SpA entities in all included patients with axSpA (OR (95% CI) 1.95 (1.49 to 2.55), p<0.001). This association was also found in all geographical regions (Europe and North America: OR 2.37 (1.52 to 3.70), p<0.001; Latin America: OR 5.00 (1.13 to 22.06), p=0.034; Middle East and North Africa: OR 2.17 (1.40 to 3.35), p<0.001)), except for Asia which did show the same trend (OR 1.90 (0.93 to 3.87), p=0.077).
An inverse association with HLA-B27 positivity was found for patients with a PFH of IBD and psoriasis independent of the presence of a PFH of any of the other SpA entities in the total included axSpA population (IBD: OR 0.37 (0.22 to 0.61), p<0.001; psoriasis: OR 0.66 (0.46 to 0.93), p=0.018). When stratified by geographical region, a similar association was only found in Europe and North America for a PFH of IBD (OR 0.45 (0.24 to 0.84), p=0.012). In other geographical regions the same trend was seen, but a PFH of IBD and psoriasis occurred less frequently than in Europe and North America (data not shown).
In multivariable models, no association with HLA-B27 was found for uveitis and ReA in the total included axSpA population (uveitis: OR 1.59 (0.78 to 3.22), p=0.198; ReA: OR 1.45 (0.41 to 5.22), p=0.565).
Discussion
Across all geographical regions, axSpA was the most common SpA entity in a PFH while a PFH of ReA was rare, which is in line with previous findings from the ASAS, DESIR and SPACE cohorts.2–4 In univariable stratified analyses, an association with HLA-B27 was apparent for a PFH of axSpA in all geographical regions except for the Middle East and North Africa. The absence of an association between HLA-B27 and a PFH of axSpA in the Middle East and North Africa may be caused by the high prevalence of a PFH of axSpA in HLA-B27-negative patients in that region combined with a lower prevalence of HLA-B27-positive disease.9–11 Multivariable models showed that the association between a PFH of axSpA and HLA-B27 positivity was independent of the presence of a PFH of other SpA entities in all included patients diagnosed with axSpA in each geographical region. These findings confirm that the association between PFH and HLA-B27 status is largely driven by a PFH of axSpA, as was also shown in previous research, but is now confirmed in various regions worldwide.
In our study the associations between HLA-B27 positivity and a PFH of IBD and psoriasis were found to be of opposite direction, and an association was found only in Europe and North America and the Middle East and North Africa, respectively. Similar trends were found in the ASAS, DESIR and SPACE cohorts.2–4 In a large cross-disease genetic study among chronic immune-mediated diseases, several SNPs (Single-Nucleotide Polymorphisms) were found with opposite directions of effect for AS, IBD and psoriasis analogous to the association of HLA-B27 with a PFH of axSpA, IBD and psoriasis in our study.12 It is important to note that in the current study only patients with predominantly axial symptoms were investigated. We would like to emphasise that these results are therefore not applicable to patients with predominantly peripheral symptoms. In these patients a PFH of a different SpA entity such as psoriasis is likely more relevant.13
A predecessor of the ASAS classification criteria was the European Spondylarthropathy Study Group criteria,14 where axSpA was considered part of a group of inflammatory diseases then known as spondylarthropathies. These included ReA, psoriatic arthritis, arthritis associated with IBD, a subgroup of juvenile chronic arthritis and ankylosing spondylitis.14 This criteria set included PFH as a criterion and thus included all these individual SpA entities combined into a single feature for ease of use (ie, reduction of variables). This expert definition was not tested nor validated prior to inclusion in the ASAS classification criteria for axSpA but included on the basis of its performance as a criterion in previous studies.14–21 In these studies, not only patients diagnosed with axSpA but also patients with other forms of SpA were analysed, and in almost all studies only the combined definition of a PFH of SpA (ie, in which a PFH of all SpA entities was combined) was studied.
Building on this, we emphasise that it is important to differentiate between the settings in which PFH is used. Settings can vary from using PFH for identifying patients at risk of axSpA before referral to using PFH for diagnosis and prognosis and to classification of patients with axSpA. The results from our study, but also the other cohorts, point towards adaptations of the definition of PFH in order to improve the sensitivity and/or specificity of PFH. Once this has been achieved, the role of PFH in the classification criteria should be re-evaluated too. Based on our data and three large axSpA cohorts (ASAS, DESIR, SPACE), we propose to investigate redefining a PFH of SpA to a PFH of axSpA (but not the other SpA entities) in a first-degree or second-degree family member to improve its sensitivity and/or specificity and to improve its position in the context of axSpA classification criteria. The CLASSIC study (Classification of Axial Spondyloarthritis Inception Cohort) provides a unique opportunity to investigate the sensitivity and specificity of the classification criteria for axSpA, including this redefined definition, as this is a large worldwide prospective study which has been initiated by ASAS and SPARTAN (SPondyloArthritis Research and Treatment Network) to reassess the performance of the ASAS classification criteria for axSpA.
A major strength of this study is its worldwide character, which enabled us to investigate patients from various geographical regions. This study included patients from Asia, Latin America, and Middle East and North Africa, populations which have been largely neglected in previous research. Another strength is that family history was reported in detail, which allowed us to investigate PFH of each of the five SpA entities separately.
A major limitation is that family history is patient-reported, which could lead to an underestimation and overestimation for obvious reasons (eg, ReA in a distant relative). It requires specific follow-up questions from the healthcare professional collecting the information (eg, uncle with axSpA is only relevant if this is a blood relative). Nonetheless, this is congruent to what is collected in clinical practice and the way the information of PFH is used. The only other way to collect information on SpA entities in the family is extensive family research, which is generally not feasible. Finally, data were collected cross-sectionally and only available data were used in this study. This resulted in a percentage of patients for whom HLA-B27 status was unknown (20%). However, this mirrors clinical practice worldwide too, as these were all patients visiting the rheumatological outpatient clinics where testing HLA-B27 is not always deemed informative or feasible.
In conclusion, across the globe, axSpA is the most common entity of SpA in a family history, expanding what was found in the ASAS, DESIR and SPACE cohorts to a more global perspective. In all geographical regions except the Middle East and North Africa, a PFH of axSpA was associated with HLA-B27 positivity in patients with axSpA. Although the prevalence of HLA-B27 positivity is relatively low in the Middle East and North Africa compared with other geographical regions, a PFH of axSpA was the most common form of PFH in this region identical to the other geographical regions.
Given the consistent findings from this study and other cohorts, the current expert definition of a PFH of SpA may be redefined to a PFH of axSpA, including only the presence of axSpA. This new definition should be re-evaluated by assessing if this definition improves the sensitivity and/or specificity of PFH and its role in the classification criteria for axSpA.
Given the similar pattern of PFH around the world, it is expected that a refined definition will be applicable to all parts of the world.
Data availability statement
No data are available. For this study we used data from the ASAS-PerSpA data set. Therefore we kindly refer interested parties to the first author of the original ASAS-PerSpA publication.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was conducted according to the guidelines for Good Clinical Practice and was approved by the ethical committees in all countries: Comité de Docencia e Investigaciones Hospital de Clinicas Dr Nicolás Avellaneda (Argentina), Health Research Ethics Board of the University of Alberta and Alberta Health Services (Canada), Comité ético Científico Servicio Salud Metropolitano Sur Oriente (Chile), Ethics Committee of the Third Affiliated Hospital of Sun Yat-sen University (China), Comité de Ética en Investigación del Hospital Militar Central (Colombia), Research Ethics Committee of Cairo University Faculty of Medicine (Egypt), Comité de protection des personnes Ile de France III (France), Ethics Committee from the medical council Westphalia-Lippe and the Westphalian Wilhelms University (Germany), Ethics Committee of Semmelweis Egyetem Hospital (Hungary), NHL Institutional Review Board (NHLIRB), SMT NHL Municipal Medical College (India), Comitato Etico Pavia (Italy), Ethics Committee of St Luke’s International University (Japan), Comité d’éthique Hotel Dieu de France (Lebanon), Comité de Investigación Hospital General de México Eduardo Liceaga (Mexico), Comité d’Éthique pour la Recherche Biomédicale de Rabat (Morocco), Commissie Medische Ethiek Leids Universitair Medisch Centrum (the Netherlands), Comissão de Ética para a Saúde do Centro Hospitalar de Lisboa Ocidental (Portugal), Comisia de Etica UMF Iuliu Hatieganu Cluj Napoca (Romania), Ethics Committee of Chonnam National University Medical School from Gwangju (South Korea), Comité de Ética de la Investigación con Medicamentos, Hospital Universitario La Paz (Spain), Chang Gung Medical Foundation Institutional Review Board (Taiwan), Marmara University School of Medicine Clinical Research Ethics Committee (Turkey), and Metrohealth Institutional Review Board (USA). Written informed consent was obtained from the subjects before enrolment. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
This study was conducted under the umbrella of the Assessment of SpondyloArthritis international Society (ASAS). We would like to acknowledge all the patients and investigators who participated in this research. We would like to thank the ASAS-PerSpA Steering Committee members, Clininfo, and the pharma companies supporting this initiative.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
AB and MvL are joint first authors.
AB and MvL contributed equally.
Presented at The initial findings of the work presented in this manuscript have been presented at the EULAR 2021 Conference and ACR 2021 Conference and have been published as conference abstracts (EULAR: Van Lunteren M, Boel A, López-Medina C, et al. POS0240 Geographical prevalence of family history in patients with axial spondyloarthritis and its association with HLA-B27 in the ASAS-PerSpA study. Annals of the Rheumatic Diseases 2021;80:341; ACR: Van Lunteren M, Boel A, López Medina C, Sieper J, van der Heijde D, van Gaalen F. Geographical prevalence of family history in patients with axial SpA and its association with HLA-B27: data from the worldwide ASAS-PerSpA study (abstract). Arthritis Rheumatol. 2021; 73 (suppl 10)).
Funding The ASAS-PerSpA study was conducted under the umbrella of ASAS with unrestricted grant from AbbVie, Pfizer, Lilly, Novartis, UCB, Janssen and Merck.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.