Article Text

Abstract
Background Considering non-classical environmental risk factors for osteoarthritis (OA), a systematic literature review (SLR) was performed to summarise existing knowledge on associations between OA and pollutants.
Methods PubMed was used to identify studies reporting data on OA and pollutants in humans (examples of MeSH terms: “Pesticides” or “Polychlorinated Biphenyls” or ‘Lead’). Reports included epidemiological clinical studies, pollutant assessments in ex vivo OA joint, and in vitro effects of pollutants on chondrocytes.
Results Among the 193 potentially relevant articles, 14 were selected and combined with 9 articles obtained by manual search. Among these 23 articles there were: (1) 11 epidemiological studies on the relationship between OA and pollutants exposure, (2) 8 on pollutant concentrations in ex vivo OA joint, (3) 4 on the in vitro effects of pollutants on human chondrocytes. Epidemiological studies investigating mainly chlorinated and fluorinated pollutants suggested a possible link with OA. In cross-sectional studies, radiographic knee OA prevalence increased with higher serum lead levels. There was also a relationship between serum lead levels and serum/urine joint biomarkers. A high concentration of heavy metals in the cartilage tidemark was found in ex vivo joints. In vitro, the viability of chondrocytes was reduced in presence of some pollutants. However, the level of knowledge currently remains low, justifying the need for new methodologically sound studies.
Conclusions This SLR supports the hypothesis of a possible involvement of pollutants in OA disease risk. Large-scale epidemiological and biological studies and ideally big-data analysis are needed to confirm that pollutants could be risk factors for OA.
- osteoarthritis
- chondrocytes
- epidemiology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
There is increased prevalence of arthritis in population exposed to mass poisoning.
There is an association between pollutant serum concentration and osteoarthritis (OA) status in large cohorts.
Heavy metals like lead and zinc have been found in ex vivo OA joint but no comparison was made with healthy joint.
There is evidence of some pollutants inducing diminution of cell viability in cultured cell.
Introduction
Osteoarthritis (OA) is the most common joint disease worldwide affecting 250 million people. Symptomatic knee OA prevalence varies from 9% to 27% in women and from 3% to 11% in men according to a systematic review in 2011.1
Risk factors of OA such as obesity, ageing and joint injury are well known, and may explain why we can expect an increase burden and incidence of OA, due to the epidemiology of these risk factors. More recently, other less obvious risk factors have been suggested to be involved in OA risk or severity, including metabolic disease independently of obesity (eg, type 2 diabetes mellitus).2–4
Recently, an anthropologic study raised the possibility of involvement of other unexpected environmental risk factors for OA. This study investigated knee OA bony features on cadaveric adults from different era (prehistoric hunter-gatherers, early industrial era (1800s–1900s), modern postindustrial (since 1976)). They showed that the prevalence of knee OA has doubled between the modern postindustrial and early industrial era even after controlling for age and body mass index (BMI) suggesting the involvement of modern environmental risk factors for OA, beyond the classical risk factors that became ubiquitous within the past half-century.5 6
Chemical pollution could be a potential environmental risk factor for OA. Chemical pollution has now reached unprecedented levels, with mixtures of chemicals contaminating wild life and humans.7 Some chemicals are already known to have a major impact on health. Persistent organic pollutants (POPs), especially organochlorine (OC) pesticides or non-dioxin-like polychlorinated biphenyls (PCBs) have a role on endocrine dysfunction or brain development.8 The impact of pollutants has been observed for several chronic diseases with low-grade inflammation such as diabetes mellitus, obesity and Alzheimer’s disease.9–12 Several pollutants have accumulated since the industrial revolution, increasing non-infectious disease risk.13
Accordingly, we raised the hypothesis of a potential role of chemical pollutants in the initiation or progression of OA either directly or indirectly through effects on risk factors for OA (mainly components of the metabolic syndrome). We have carried out a systematic literature review (SLR) with the aim to search what type of pollutant has been already studied, what link could exist between our exposition to pollutants and the development/worsening of OA.
Methods
Systematic literature search and selection of the relevant studies
To obtain all published articles reporting association between any pollutants and OA, we performed an SLR. We used the PubMed Medline database on 15 January 2019 (no limitation of year far back) with the following keywords: ((“Pesticides”[Mesh]) OR “Environmental Pollution”[Mesh]) OR “Benzene”[Mesh]) OR “Household Products”[Mesh]) OR “Nanostructures”[Mesh]) OR “Endocrine Disruptors”[Mesh]) OR “Xenobiotics”[Mesh]) OR “Triclosan”[Mesh]) OR “Bisphenol A-Glycidyl Methacrylate”[Mesh]) OR “DDT”[Mesh]) OR “Hexachlorobenzene”[Mesh]) OR “Chlorpyrifos”[Mesh]) OR “Polychlorinated Biphenyls”[Mesh]) OR “Flame Retardants”[Mesh]) OR Phthalic Acids”[Mesh]) OR “Fluorocarbons”[Mesh] OR “Lead”[Mesh] OR organic pollutant)) AND “Osteoarthritis”[Mesh] for humans in English or French. The results of this search included articles from 1963 to 2019. Abstracts from international congresses were reviewed for the past 2 years, combined with manual curation (screening of the reference list of the included studies). All types of publications were accepted. All types of population, age range and OA were included. The types of pollutants chosen for the Mesh term on PubMed were identified according to the advices of experts in pollutants and endocrine disruptors (J-BF, M-SC-F and BD), but we did not exclude a pollutant for the selection of studies.
Data collection
Data were collected using a predetermined form: author, year of publication, country, year of study, type of study, number of participants, type of OA, site of OA, type of pollutant and method to determine exposure. We collected data on link between pollutant and OA: prevalence of OA in pollutant exposure, rate of pollutants in patients with OA, OR (OR; 95% IC) or relative risk, prevalence, conclusion on an association, concentration of pollutant, grade of OA if available. Two investigators (CD, KL) have independently participated to the selection of articles (title/abstract/full text) and data extraction. Results were compared during meetings between the two data extractors. If there was a discordance, a third investigator (JS) had to decide. This SLR is a narrative synthesis of study findings.
Results
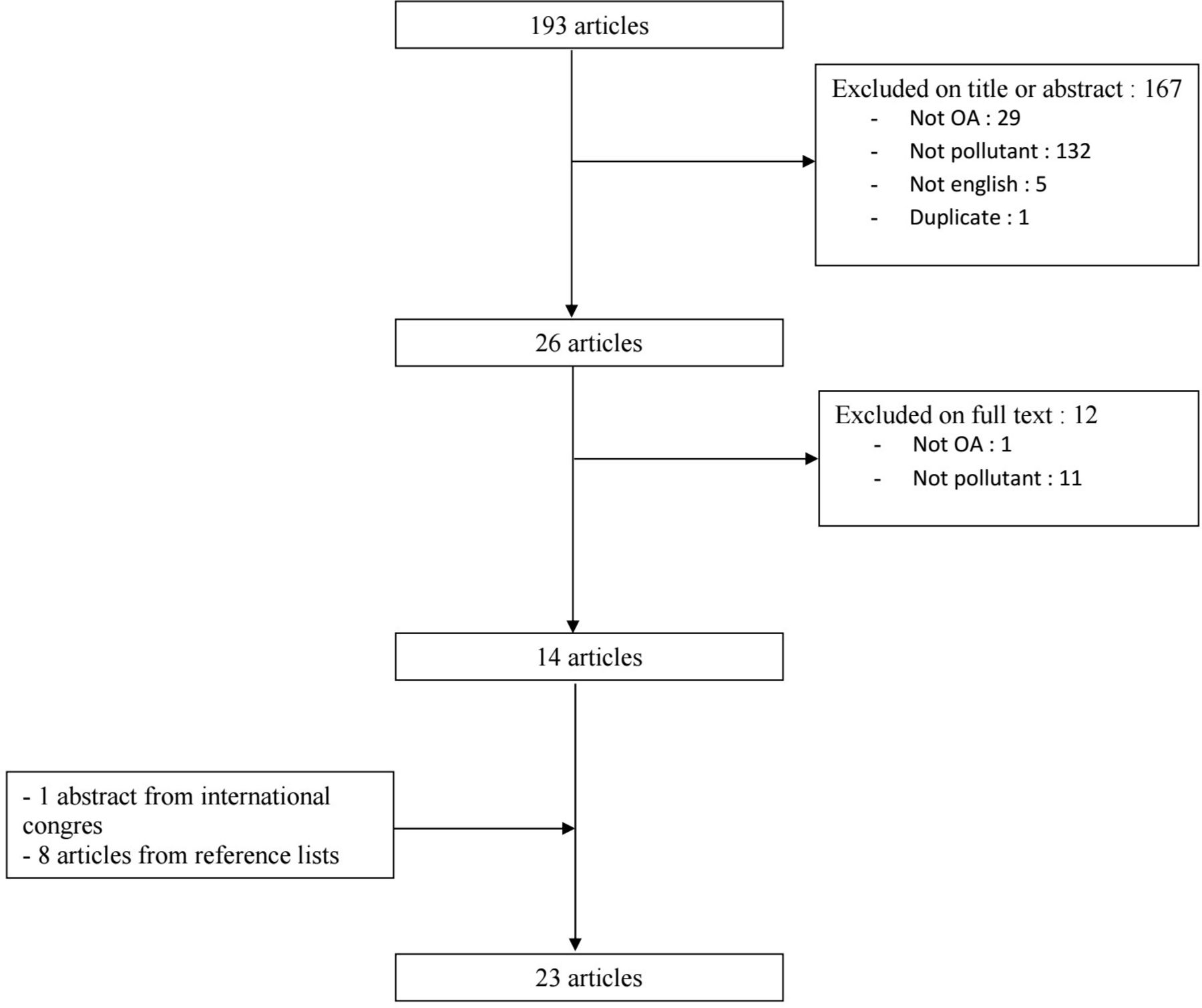
Of the 193 publications identified by the literature search, 14 fulfil the selection criteria. One hundred sixty-six were excluded on title and abstract (including 132 because there was no concept of pollutant), and 12 after full text examination (including 11 because there was no concept of pollutant). Nine articles were added (1 abstract from international congress, 8 articles from references). Finally, a total of 23 articles were included in the analysis. A flow chart is given in figure 1.
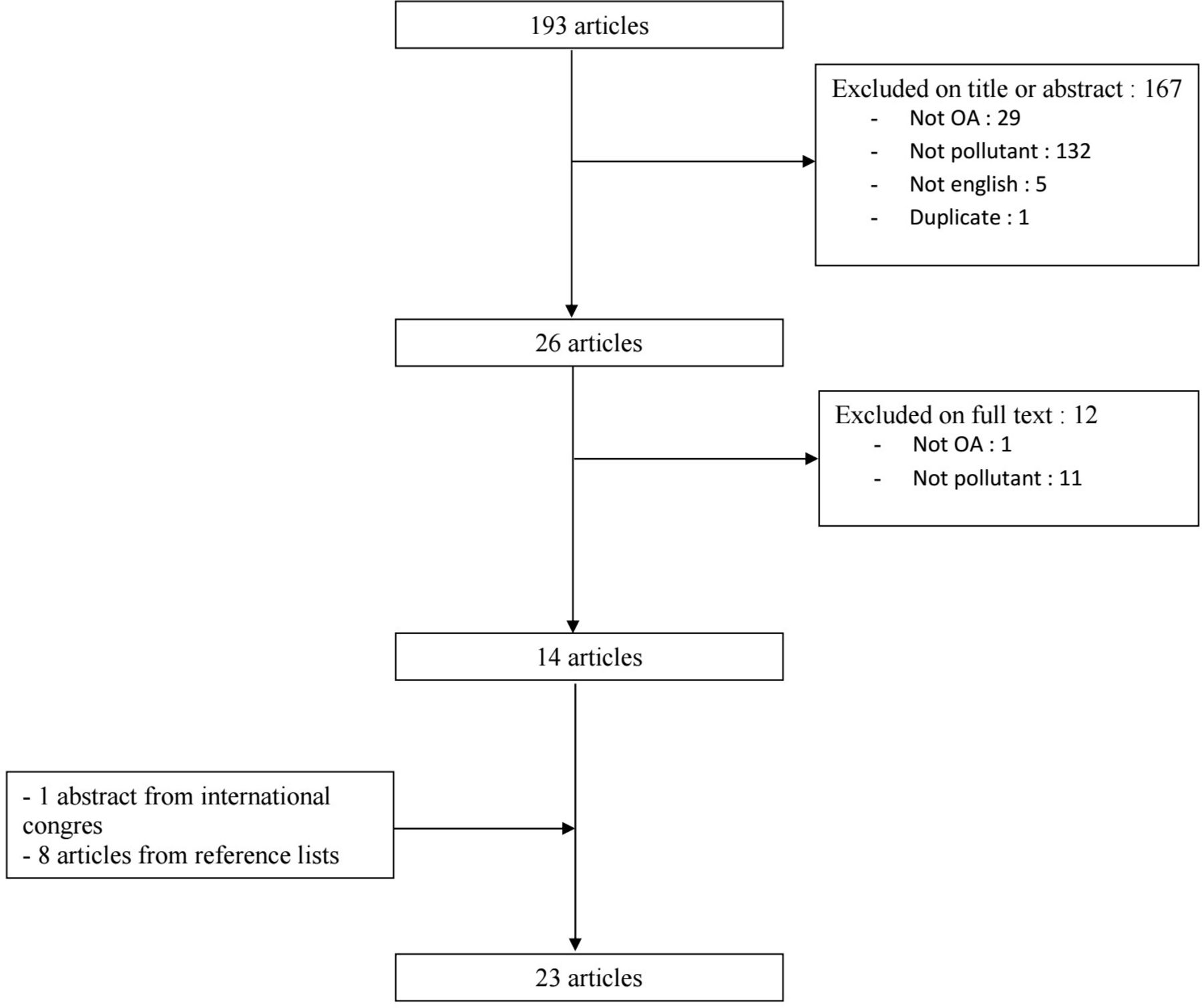
Flow chart of the systematic literature review. OA, osteoarthritis.
The 23 publications included (1) 11 epidemiological studies that assessed a relationship between OA and reporting exposition to some pollutants, (2) 8 reports on pollutant concentrations in ex vivo OA joint tissues, (3) 4 studies reporting in vitro effects of pollutants on human chondrocyte/cartilage.
The pollutants studied were mainly PCBs (n=5 studies), perfluorooctanoates (PFOA)/perfluorooctane sulfonates (PFOS) (n=2), lead and other heavy metals (n=12).
Epidemiological clinical studies
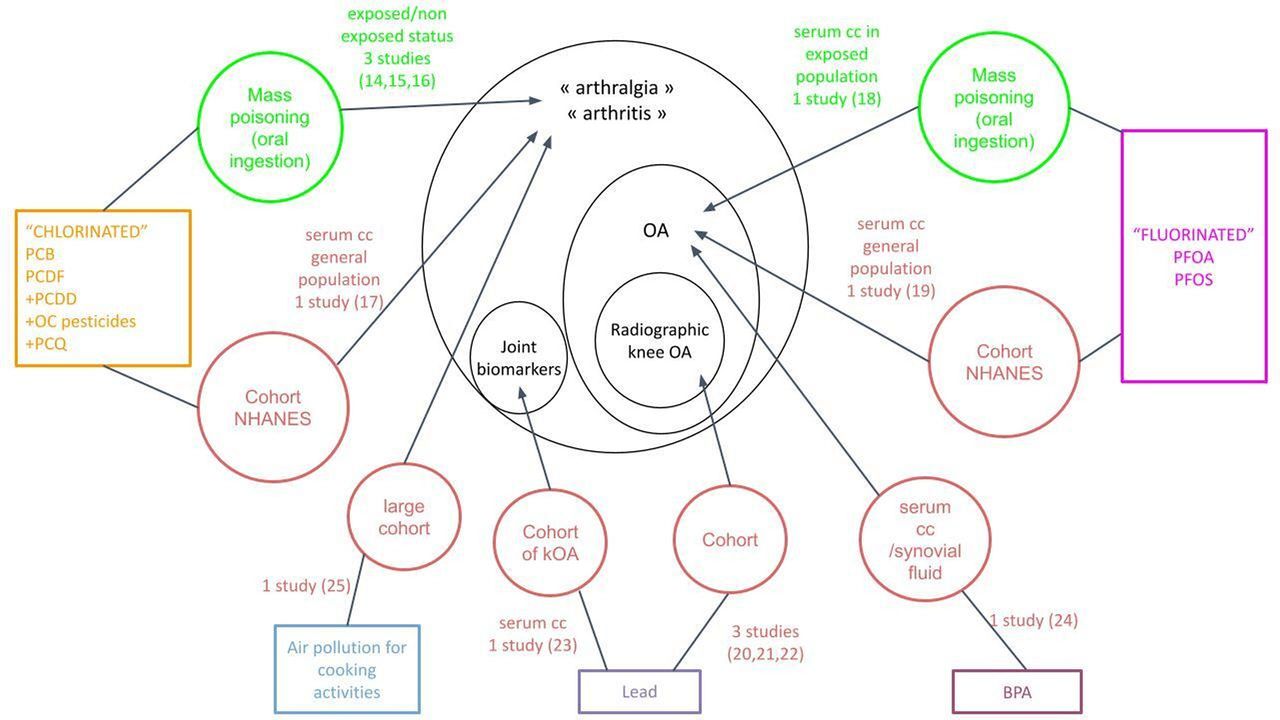
Eleven articles were epidemiological clinical studies (online supplemental table 1 and figure 2) and included 11 523 patients but they are not necessarily unique patients because some studies come from the same cohorts. Gender was available for 6725 patients of whom 4012 were women (59.6%). There were cross-sectional studies from postmass-poisoning cohorts or population-based cohorts.
Supplemental material

Summary of the effects of pollutants in epidemiological clinical studies. kOA, knee osteoarthritis; NHANES, National Health and Nutrition Examination Survey; OA, osteoarthritis; OC pesticides, organo chloride pesticides; PCB, polychlorinated biphenyls; PCDD, polychlorinated dibenzo-p-dioxins; PCDF, polychlorinated dibenzofurans; PCQ, polychlorinated quarterphenyls; PFOA, perfluorooctanoate; PFOS, perfluorooctane sulfonate; serum cc, serum concentration.
Four articles studied the link between PCBs and arthritis. Three of them reported arthritis after incidental mass poisoning with PCB (two episodes of contamination of oil in Japan14 15 and contamination of meat/dairy products/eggs in Michigan).16 The first one15 reported ‘Yusho’ patients. Yusho was a food poisoning incident that occurred in Japan in 1968. Exposed patients could have Yusho symptoms (essentially acne-form eruptions and cutaneous/mucosal pigmentation). Thirty-five years after this incident, blood pollutants dosages and examinations were performed. In this study, arthralgia was significantly correlated with polychlorinated dibenzofuran (PCDF) serum concentrations (generated by heat denaturation of PCB), p=0.001 and tended to correlate with PCB and polychlorinated quarterphenyls.
In the second, 2000 people had ingested cooking oil contaminated by PCB and PCDF in 1979 in Taiwan.14 The people were followed in a registry. They had dermatological and neurological symptoms. Illness was referred as ‘Yucheng disease’. Fourteen years after, exposed people born before 1963 were selected and matched with non-exposed control group to participate in an evaluation of morbidity. The risk of arthritis-reported was significantly higher in exposed patients than non-exposed people, in men only: OR 4.1 (95% CI 1.8 to 11.2) (in women OR=1.3 (95% CI 0.8 to 2.3)).
The third study reported the PCB contamination of animals from 1049 farms in Michigan in 1976.16 The data involved farmers and families who had eaten meat/dairy products/eggs contaminated. The control group was farmers from another state (Wisconsin). Declarative questionnaires that included questions on joint pain and joint swelling, physical examination and laboratory tests including blood PCB measurement were performed. The prevalence of musculoskeletal symptoms was higher in PCB-exposed Michigan farmers (40%) than others farmers (30%), χ2=3.8 p=0.05. However, the prevalence of degenerative arthritis, namely OA, as current illness under treatment was 10% in Michigan farmers versus 17% in others farmers, χ2 =4.22 p<0.05. In the last publication, they use cross-sectional data from the National Health and Nutrition Examination Survey (NHANES) cohort, which accurately reflect the US general population. 1721 participants underwent an interview, a physical examination and a blood sample for pollutants (polychlorinated dibenzo-p-dioxins (PCDD), PCDF, dioxin-like PCB, non-dioxin-like PCB and OC pesticides) measurements.17 Among these participants, 414 reported arthritis (116 reported OA). According to concentration of these pollutants, participants were ranked in four quartiles. The adjusted factors were age, ethnicity, poverty income ratio, BMI and smoking. Arthritis was more frequent in patients having higher level of pollutants. The risk to report arthritis was higher in PCDD/PCDF/PCB/OC pesticides detectable versus non detectable. Adjusted OR (aOR) between 1.1 and 1.5 in men (non-statistically significant) and between 1.3 and 2.9 in women (p=0.02 for PCB). In women, for subgroups of PCB, higher aOR was 3.2 (95% CI 1.6 to 6.7), p<0.01. Of note, the higher serum concentration of PCB was especially associated with higher risk of arthritis. This association was statistically significant for 5/9 subtypes of PCB (PCB 74, 118, 170, 180, 187). In women, the risk to report arthritis was higher in OC pesticides detectable versus undetectable, with higher aOR 3.1 (95% CI 1.3 to 7.1), p<0.01, statistically significant for only ¼ subtype of OC pesticides (oxychlordane). When the authors differentiated the subtypes of arthritis, the association persisted for rheumatoid arthritis, but not for OA.
Two articles focused on serum levels of PFOA and PFOS.18 19 These are persistent environmental pollutants that are used in more than 200 industrial processes and consumer applications (such as emulsifiers, protective coatings for textiles and food storage containers). In a cross-sectional study, the authors investigated the association of OA with PFOA and PFOS in a population of 49 432 adults from 6 PFOA-contaminated water districts in mid-Ohio Valley (2005–2006).18 Among them, 3731 had reported OA while diagnosis of RA (rhumatoid arthritis) was an exclusion criterion. Blood PFOA and PFOS levels were assessed. Confounding factors including age, BMI, sex, socioeconomic status, menopausal status, lifestyle factors, comorbidity and others were considered. Reported OA prevalence increased with PFOA serum levels: for highest quartile versus lowest quartile of PFOA serum concentration, aOR for OA was 1.42 (1.26 to 1.59), p=0.00001. This relation was significantly stronger in adults <55 years-old and in non-obese adults. Surprisingly, the concentration of PFOS was associated with less OA (aOR was 0.76 (0.68–0.85), p=0.00001). The second publication comes from the NHANES cohort in 2003–200819. In this general population, PFOA and PFOS were measured in blood serum and OA was evaluated with questionnaire. Potential confounders considered were age, sex, poverty status, ethnicity, daily fat and caloric intake, BMI, fractures, sports, smoking status, parity. The authors found a significant association between higher rates of PFOA and OA in women (fully aOR=1.98 (1.24 to 3.19; p<0.01), not for men (fully aOR=0.82 (0.40 to 1.70). For PFOS, there was a significant association between higher rates of PFOS and OA in the whole studied population (fully aOR=1.77 (1.05 to 2.96) but such an association was no longer statistically significant when men and women were analysed separately.
Concerning lead, three articles studied the relation between this pollutant and OA. In the Korean National Health and Nutrition Examination Survey (2010–2012), which is a cross-sectional study in the general population, higher serum lead levels were associated with a higher prevalence of radiographic knee OA versus lower serum lead levels20: aOR was 1.90 (1.09 to 3.32) for men and 1.81 (1.17 to 2.77) for women after adjustment on age, BMI, house income, education, smoking, alcohol drinking, physical activity, occupation. In the Johnson Country OA Project, including adults living in rural townships, blood lead levels, radiographs of the knees and symptom questionnaire were performed.21 The risk of having knee OA was 20% higher for every 1-unit increase in lead serum level (aOR=1.20 (1.01 to 1.44)), after adjustment for age, sex, race, BMI, smoking and alcohol drinking.21 In the last study, in 90 Egyptian patients with knee OA, there was a significant correlation between blood lead level and the severity of knee OA either clinically and radiologically (p<0.001).22 Interestingly, in a study of Nelson et al from Johnston County OA project, lead serum levels were linked with biomarkers of joint tissue metabolism (urinary cross-linked N telopeptide of type I (uNTX-I),C- telopeptide fragments of type II collagen (uCTX-II), serum cartilage oligomeric matrix protein).23
Bisphenol A (BPA) was detected in the serum of three tested patients with OA (from 17.5 to 23.3 nM) while it is not detected in two patients with immune rheumatism. BPA was also detected in synovial fluid of the tested patient undergoing knee replacement arthroplasty and the concentration was higher than in the serum (54.8 nM vs 23.3 nM).24
Finally, there are limited data about household air pollution. In one study, household air pollution induced by the cooking heat source, electricity or gas/coal, wood or other material was examined. Compared with electricity, gas or other sources of cooking methods increased the risk of arthritis with aOR from 1.73 to 2.00, in a large cohort from the WHO.25 There are no data about outdoor air pollution (such as PM (particulate matter) 2.5 and NO2 exposure) in OA.
Experimental studies
Pollutants concentration in ex vivo OA joint tissues
Six articles reported lead and other chemical elements (calcium, zinc, cadmium, iron, fluor and others) concentration on joint tissue samples harvested during arthroplasty for hip or knee OA (online supplemental table 2 and figure 3). All studies were from Poland or Austria and the samples were small. Together, they represented 202 patients. Gender was known for 153 patients including 110 women (72%). No studies have compared lead concentration between cartilage from patients with OA versus healthy subjects.
Supplemental material

Summary of pollutants data in ex vivo studies.
Brodziak-Dopierala et al reported 53 patients exposed to high environmental concentration of lead due to heavy industry (inhabitants of the Upper Silesian Industrial Area) and who have undergone total hip replacement.26 In this population, the highest concentration of lead was found in cancellous bone from the femoral head, followed by articular cartilage, cortical bone, intertrochanteric cancellous bone and joint capsule. The concentration of lead in the cartilage and bone increased with age in two studies.26 27 In another study, 10 chemical elements, among which lead was included, were quantified in 33 tibial plateau samples obtain during knee joint arthroplasty28: fluor concentration in the inorganic portion of bone, but not other elements, was significant higher in OA knee than in injury knee. Three articles from the same cohort reported higher concentration in men than women for the knee28 and for the hip,29 30 and two others no difference according to sex.26 27 There was higher cartilage concentration of lead in smokers than in non-smokers in two studies.
Two studies with X-ray fluorescence examination performed on cadavers without OA (14 samples) found an accumulation of lead in the cartilage tidemark, the zone between the non-calcified and the calcified articular cartilage.31 32
In vitro effects of pollutants on human chondrocyte
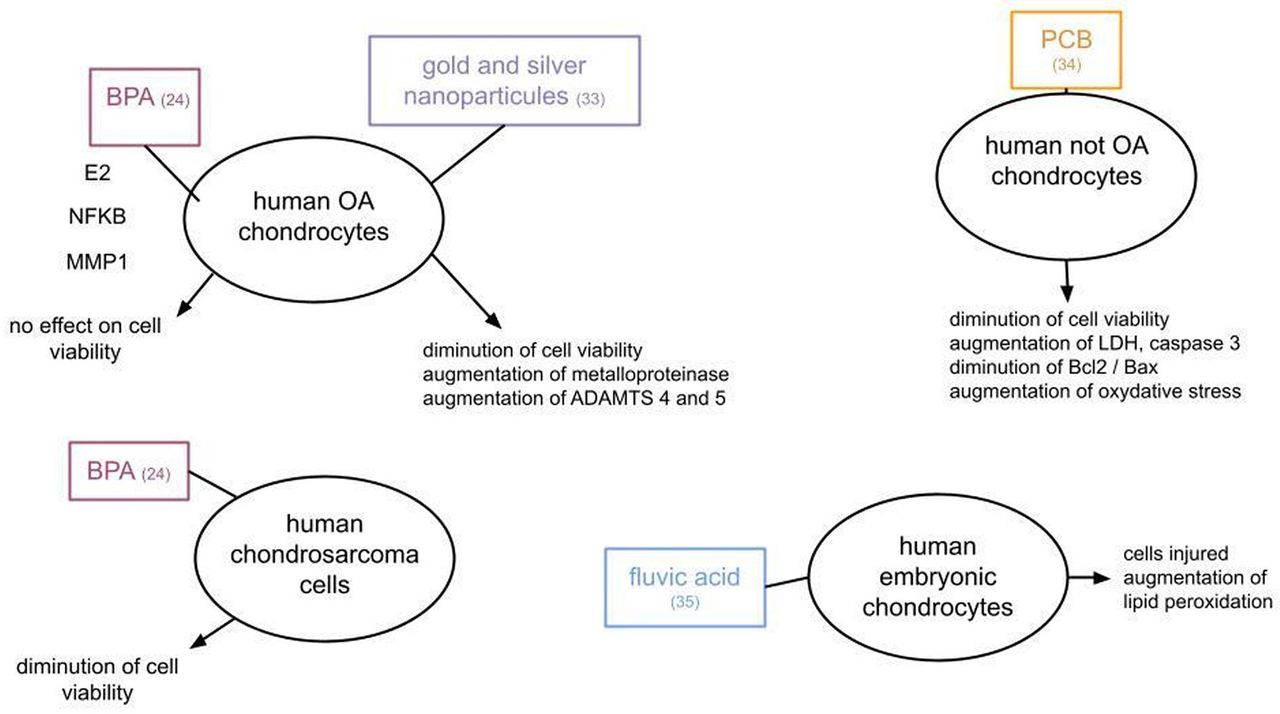
Four studies assessed the in vitro effect of pollutants on human chondrocytes (online supplemental table 3 and figure 4).
Supplemental material
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Summary of pollutants data in in vivo studies. ADAMTS, A Disintegrin And Metalloproteinase with Thrombospondin motifs; Bax, Bcl2 associated X protein; Bcl2, B-cell lymphoma 2; BPA, bisphenol A; E2, estradiol; LDH, lactate dehydrogenase; MMP1, mettaloproteinase 1; NFKB, nuclear factor kappa B; OA, osteoarthritis; PCB, polychlorinated biphenyl.
Pascarelli et al cultured human OA chondrocytes, from patients with hip OA, with gold or silver nanoparticles. These nanoparticles induced a dose-dependent cytotoxic effect (from 80 to 250 µM) and a dose-dependent secretion of metalloproteinases.33 As well, PCB (from 1 to 10 µM) decreased cell viability of cultured immortalised human juvenile costal chondrocyte. Are noted increase of necrosis and aptosis markers and oxidative stress index.34
BPA may antagonise the protective effects of estrogens (E2) on cultured OA chondrocytes stimulated by interleukin 1β (obtained during arthroplasty).24
Peng et al focused on Kashin-Beck disease, a chronically endemic OA disease in China.35 The authors noticed a high concentration of fluvic acid or other free radicals in drinking water. As a result, they performed several experimental models including cell cultures of human embryonic chondrocytes with these free radicals. Fluvic acid was reportedly pathogenic since it injured chondrocytes and increased lipid peroxidation, conversely to what decreases such a peroxidation.
Discussion
In addition to the traditional risk factors, external environmental factors could also influence the development and progression of OA. Our SLR raises the following assumptions (1) high exposition to PCB, OC pesticides and PFOA/PFOS is potentially associated with an increased risk of OA, (2) there might be an association between serum lead levels and radiographic knee OA, (3) lead concentration is high in cartilage harvested during arthroplasty for OA (without knowing concentration in healthy cartilage) and (4) some heavy metals, BPA and fluvic acid could promote human chondrocyte death or dysfunction in vitro. Altogether these results suggest a possible link between OA and pollutants.
Various types of pollutants were studied for a potential role in OA such as PCB and other POPs, OC pesticides, PFOA, PFOS, lead and other chemical elements. Such a list is based on studies availability and the wide and common exposure in general population. However, at least three factors need to be considered here. First, the ever-increasing number of chemical pollutants currently used, second, their relative half-lives and third, the effects of mixtures of chemicals. Mixtures of chemicals have been studied for other disease (eg, effect of contaminants in human amniotic fluid on thyroid hormone signalling and brain development), but we have not found such studies in OA.
BPA is produced worldwide and used extensively in epoxy resins lining food and beverage containers and polycarbonate plastics in many consumer products. Many studies demonstrated estrogenic activation, decreasing sperm production, alteration in the onset of sexual maturity and obesogenic effects.36–38 It is now banned in most countries, at least for baby product and food containers, but still present in human fluid.
PCBs are widely distributed in the environment, since they have been used in the industry on a large scale during the last century. These pollutants, due to their high chemical stability and lipophilicity, tend to accumulate mainly in lipid rich-tissues. High exposition to PCB in a context of water/food poisoning is normally related to dermatological, ophthalmological and mucosal signs.39
PFOA and PFOS are part of perfuoroalkyl acids family (PFAA), exclusively man-made chemicals. PFAA are use in >200 industrial processes and consumer applications (protective coatings for textiles, wood, leather, food storage containers, Teflon coating, personal care products).40 They have persistent chemical properties and they resist to environmental degradation. U.S. Environmental Protection Agency requested the removal of these chemicals but they are still used in some areas. PFOA and PFOS have been linked to thyroid disease,41 42 ulcerative colitis,43–45 elevated levels of liver enzymes, elevations in serum uric acid levels, adverse lipid profiles, insulin resistance in humans42 46 47 and cancer.48–50
Lead, cadmium and mercury induce damages of the kidney, liver, brain and bone.51 52 Fluoride accumulation in bone is known to be harmful. Conversely, iron, zinc, selenium and manganese are essential for the physiology of living organisms but may be toxic at high levels of exposure. These heavy metals naturally exist in the environment but some are/have been largely employed in industrial products. Lead has been widely employed in paint, fuel, piping and so on and its toxic effect on body, especially on the central nervous system, is no longer debated. It has been banned in some countries such as the USA and Europe, but this is not the case everywhere in the world and there is a bioaccumulation of this pollutant. Likewise, most adults have already accumulated a substantial body burden of lead.
Epidemiological clinical studies focused mainly on PCB, PFOA/PFOS and lead. These studies suggest a possible link between these pollutants and OA, but results are discordant for some studies. In ex vivo studies, we reported that some pollutants such as lead accumulate in the joint tissues and then may have deleterious effects such as those found on chondrocytes. Last articles reported effect of pollutants on human chondrocytes in vitro: some nanoparticles or PCB or BPA had a repercussion on chondrocyte viability.
Pollutants could have either a direct toxic effect or through obesity and/or endocrine disruption on thyroid signalling or through other nuclear receptors and their signalling pathways targeted by endocrine disrupting chemicals.53 These include PPARs (peroxisome proliferator activated receptors), ARs (androgen receptors), ERs (estrogen receptors), RXRs (retinoid X receptors), PXRs (pregnane X receptors) and TRs (thyroid hormone receptors), as well as AhR (the aryl hydrocarbon receptor that acts as a receptor for dioxin and PCBs).
The effects of pollutants on the disruption of endogenous hormones have been known for decade, with key examples being the sexual hormones or thyroxin.8 13 54 Some pollutants increase pro-inflammatory cytokines, increase oxidative stress, and have a direct cytotoxic effect. Some are stored in adipose tissue and can cause metabolic disturbances, including over-secretion of leptin55 or insulin resistance.56 Lead appears to be toxic to the joint according to publications of arthropathies in animal studies and related to intra-articular bullets in humans.57 58
Some studies (not presented in this SLR) reported association between occupational activity and OA: this association can be explained by the work-related physical activity (like kneeling), but these studies covered works leading to potential exposure to pollutants (miners, farmers, cleaners, women in the clothing industry) so there is also a potential role of pollutants in the development of OA in these patients.59–61
However, several comments can be made that could weaken our conclusions. First, despite we have several publications on pollutants in OA, epidemiological studies were cross-sectional studies from cohorts: increased report of joint symptoms in people that were exposed to an accidental high exposure to pollutants, or an increased pollutant blood concentration in patients reporting OA from population-based cohorts. The association present in some studies here does not mean it is necessarily a causal association given the design of the studies. Most of the studies are about poisoning accident with high level of pollutants exposure. Considering the frequency and the chronicity of OA, studies on chronic low exposures in everyday life would be better valuable. Second, the definition of cases, namely patients with OA, is an issue in some studies. In studies on PCB, the studied disease was ‘arthritis’ without precision of ‘OA’ (among a large list of symptoms by organ system). However, considering the frequency of OA and the frequency of inflammatory rheumatic diseases such as rheumatoid arthritis or ankylosing spondylitis (~10 vs 1% of the population in general, respectively), we may expect that OA was the main diagnosis among arthritis cases. Moreover, some caution should be made about the accuracy of OA diagnosis in the studies about PCB and PFOA/PFOS since it was a self-reported diagnosis by the patient. However, some authors reported 81% agreement between self-reported of ‘definite’ OA and clinical confirmation.62 Third, according to ex vivo studies, pollutants (chemical elements) were found in OA joint samples but without comparison with healthy joints. However, the normal comparator is a recurrent issue in OA research since it is unrealistic and unethic to get normal joints. Of note, the majority of publications on this topic are from Poland so the results are not generalisable since exposure to pollutant might change between countries. Forth, these ex vivo studies were only on chemical elements, including heavy metals, but there were no studies on synthetic pollutants and traditional risk factors of OA were not mentioned. Finally, in vitro studies are scarce since there was only one study with gold or silver, one study with PCB and one study with BPA. Also noted that unfortunately our review is not registered in PROSPERO.
Our review has also strengths. The selection of the keywords was large enough to avoid missing studies. Moreover, since pollutants are an emerging field of research in chronic diseases, we tried to be as exhaustive as possible to find the articles on the subject and by including all types of study: observational study, experimental data on human explants and data from cell culture. The results of all these studies are summarised in three comprehensive figures (figures 2–4).
Prevalence of OA seems to increase since around 50 years and environmental factors may be involved in this phenomenon. Our SLR gives a signal concerning the involvement of environmental pollutants in OA. However, there is a critical need for novel clinical and basic research studies in order to clearly delineate the role of each pollutant in OA using cohorts, biological studies and ideally big-data analysis to gather exhaustive data concerning the way of life of individuals and subsequent potential exposure.
Supplemental material
Ethics statements
Patient consent for publication
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @CamilleDeprouw
Contributors All the authors participated in this work.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.