Article Text

Objective
To analyse the performance of the rheumatoid arthritis impact of disease (RAID) score in patients with ankylosing spondylitis, polymyalgia rheumatica, systemic lupus erythematosus, primary Sjögren’s syndrome, idiopathic inflammatory myositis and systemic sclerosis, as compared with rheumatoid arthritis (RA).
Methods
A total of 12 398 patients from the German National Database were included. For each diagnosis, we calculated age-adjusted/sex-adjusted partial correlation coefficients between RAID and patient global (PtGl) health, PtGl disease activity, physician global (PhGl) disease activity, Well-Being Index (WHO-5) and EuroQoL-5 Dimensions (EQ-5D). As a measure of agreement, the mean differences between the RAID and other outcomes were compared with the respective differences for RA. The effect of each diagnosis on the difference between RAID and the other scores was assessed with linear regression, with RA as the reference.
Results
Across all diagnoses, RAID correlated strongly with PtGl health (0.71–0.83), moderately to strongly with PtGl disease activity (0.59–0.79), WHO-5 (0.65–0.81) and EQ-5D (0.68–0.73) and weakly with PhGl disease activity (0.23–0.38). Mean differences were calculated for RAID and PtGl disease activity (0 to −0.6), PtGl health (−0.4 to −0.9), WHO-5 (−0.7 to −1.3), EQ-5D (1.1 to 1.7) and PhGl disease activity (1.4 to 2.2). Discrepancies between other scores and RAID were comparable to RA. Linear regression revealed no clinically relevant effect of any of the diagnoses on the difference between RAID and the other outcomes.
Conclusion
The RAID score performs comparably across all diagnoses investigated. This supports the use of RAID for measuring the impact also of other rheumatic diseases.
- patient reported outcome measures
- outcome assessment, health care
- arthritis, rheumatoid
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is already known about this subject?
The Rheumatoid Arthritis Impact of Disease (RAID) score is a valid tool to measure the impact of rheumatoid arthritis (RA) in different domains (pain, function, fatigue, sleep disturbance, emotional well-being, physical well-being and coping) that are highly relevant for patients with RA.
With the Psoriatic Arthritis Impact of Disease questionnaire, an adapted instrument has been developed for patients with psoriatic arthritis.
What does this study add?
The use of the RAID in other inflammatory rheumatic diseases (ankylosing spondylitis, polymyalgia rheumatica, systemic lupus erythematosus, primary Sjögren’s syndrome, idiopathic inflammatory myositis and systemic sclerosis) provides meaningful results, comparable to those in RA.
The unweighted RAID score has comparable properties to the weighted score, which improves its feasibility in the clinical routine.
How might this impact on clinical practice or further developments?
The RAID could be used as a generic instrument across inflammatory rheumatic diseases to measure the impact of the disease on patient quality of life.
Introduction
The Rheumatoid Arthritis Impact of Disease (RAID) score is a patient-reported outcome measure (PROM) for evaluating the impact of rheumatoid arthritis (RA) on patient quality of life; it also indicates disease activity from the patient’s perspective.1–3 An important proportion of patients with RA with complete control of the inflammatory process still perceive significant impact of the disease, which is missed by objective clinical evaluation through physical examination and biomarkers. Ferreira et al4 5 proposed two different targets in the management of RA: disease process remission and disease impact control. To assess this impact, an international collaboration between people with RA, rheumatologists and healthcare professionals under the aegis of the European League Against Rheumatism developed the RAID. It takes the form of a simple questionnaire and is considered to give an informative expression of the general status of the patient in domains of major importance to people with RA. Although the concept of life quality and impact of disease are closely related, the comparably new term ‘impact’ refers to the inclusion of the patient’s perspective on the disease. The perceived impact of disease can be understood as major determinant of quality of life.6 Besides measuring severity of an outcome, the RAID adds the importance of the outcome to the patients and the concept of coping rarely mentioned before.7 8 The RAID domains go beyond the questions of quality of life instruments such as the EuroQoL-5 Dimensions questionnaire (EQ-5D) by also capturing fatigue, sleep disturbances and physical well-being in addition to pain, functional capacity and emotional well-being.1 9 Individual Numeric Rating Scales (NRS) are used to measure each of the domains, with 0 being the best or lowest activity score and 10 the worst or highest activity score. The values are weighted by patient assessments of relative importance and combined in a single score. While the score represents the patients’ conditions, the different domains indicate why the patients are unsatisfied. As Duarte et al9 have shown, the separate use of the individual NRS is valid, reliable and sensitive to change (RAID.7). It allows for the personalised assessment of the impact of RA in different domains and supports the selection and the monitoring of the most appropriate interventions to mitigate the impact beyond disease process remission. Among different PROMS, the RAID shows the best performance when compared with the patients opinion of their symptomatic status (PASS).10 While the Psoriatic Arthritis Impact of Disease constitutes an adapted instrument for psoriatic arthritis (PsA),11 there are no comparable instruments for other inflammatory rheumatic diseases. Since the individual RAID questions are largely generic and should also apply to other diseases, it could be an informative instrument beyond RA. This study used data from a large epidemiological database to analyse the performance of the RAID score in ankylosing spondylitis (AS), polymyalgia rheumatica (PMR), systemic lupus erythematosus (SLE), primary Sjögren’s syndrom (pSS), idiopathic inflammatory myositis (IIM) and systemic sclerosis (SSc), and to compare the performance to that in RA. For this objective, we measured the distribution of the RAID score and its deviation from other measurement tools such as the patient global health or disease activity, the WHO Well-Being Index (WHO-5) or the EQ-5D questionnaire in the other inflammatory rheumatic diagnoses and compared it to the distribution of the RAID and its deviation from the other instruments in RA.
Patients and methods
Participants and study design
The German Rheumatology Research Centres’ (DRFZ) national database (NDB) of the German collaborative arthritis centres is an ongoing prospective long-term monitoring study.12 It contains annually updated clinical data and patient-reported outcomes for unselected outpatients with inflammatory rheumatic diseases. The NDB has been specifically conceptualised to provide data on healthcare for all patients with rheumatic diseases. In addition, it contains more specific instruments for the most frequently reported diseases, which include RA, AS and SLE.
In this study, cross-sectional data from the years 2015–2019 were used. All patients with a complete RAID questionnaire were included. The patients complete all questionnaires during their visit to the rheumatological clinic or practice, either on paper or on a tablet. Patients who were seen more than once during this period were included with the last available visit. This was selected to obtain data as up to date as possible.
Measures/instruments
The NDB comprises physician-derived information, such as key clinical states including the 28-joint count Disease Activity Score-Erythrocyte Sedimentation Rate (DAS28-ESR), and the global assessment (PhGl) of disease activity (NRS from 0 to 10, with 10 as highest possible activity).13
Patients recorded the individual items of the RAID (pain, functional capacity, fatigue, physical and emotional well-being, sleep disturbances and coping) on NRSs.1 9 The individual NRSs used in the RAID are based on an RA-specific wording. In order to use the score for other rheumatic diseases we omitted the specific diagnostic reference in the question wording. In order to avoid the influence of the RA-specific weighting, we also calculated an alternative unweighted RAID score as a mean of the seven individual NRS.
Furthermore, the patients assessed the patient global (PtGl) health status (NRS 0 (best)−10 (worst), the PtGl disease activity (NRS 0 (no activity)–10 (highest))13 and the 5-item WHO Well-Being Index (WHO-5).14 An overall score from 0 to 100 is determined with higher scores indicating a better well-being. Health-related quality of life was assessed by the generic three-level version of the EQ-5D questionnaire,15 which includes five dimensions: mobility, self-care, usual activities, pain/discomfort and anxiety/depression. The combination of the five dimensions leads to an index score between −0.205 and 0.999 with higher scores indicating a better perceived quality of life.15 The EQ-5D and WHO-5 were rescaled to match the scale of the RAID (range 0–10). Patients with AS also completed the Bath Ankylosing Spondylitis Disease Activity Index (BASDAI).16
Statistical analyses
Patient characteristics and outcomes were described using means and SD for continuous variables and percentages for binary variables. A violin plot was prepared to understand the distribution of the RAID composite score at each diagnosis. The violin plot depicts distributions of numeric data using density curves. The width of each density curve corresponds with the approximate frequency of data points in each region. A floor effect was considered to be present if the RAID score was 0–1 in more than 15% of the patients.17 18
In a next step, we calculated the partial correlation coefficients between the RAID score and each of the five other instruments to control for the confounding effect of the different age and sex distributions of the diagnoses (0.3–0.5 weak, 0.5–0.7 moderate, >0.7 strong correlation). We also calculated the partial correlation coefficient between the RAID and the DAS28 in patients with RA and between the RAID and the BASDAI in patients with AS.
Furthermore, for each of the diagnoses the mean differences between the RAID score and the other outcomes were compared with the respective differences for RA. The differences were calculated by subtracting the values for the different outcomes from the RAID and plotted in a violin plot for each diagnosis. Finally, linear regression was used to assess the age-adjusted and sex-adjusted effect of each diagnosis on the difference between the RAID score and the five other scores with RA as the referent diagnosis. Results of the regression analyses are presented as regression coefficient and 95% CI. We defined the effect of a diagnosis as clinically relevant if the mean change of difference was at least one unit, that is, if the CI of the regression coefficient exceeds −1 and 1 (figure 4).
Available data for the other instruments besides RAID are reported in table 1. The proportion of missing values for the comparator variables was 5% or lower for all diagnoses, except for the WHO-5, which was not collected until 2018. The absolute of the standardised mean difference between scores from patients with valid and missing scores was below 0.2 in most cases (online supplemental table 1), with the exception of some variables and diagnoses with a very low number of missing values. Based on this, we decided not to impute any missing values.
Supplemental material
Patient characteristics and patient-reported and physician-reported outcomes in patients with inflammatory rheumatic disease
Results
From 2015 to 2019, a total of 16 625 patients with RA, AS, PMR, SLE, pSS, IIM and SSc were documented in the NDB. The RAID score was available for 12 398 patients. The proportion of missing RAID scores ranged between 22% in PMR and 33% in SSc. Patients without RAID scores did not differ regarding sex (72 vs 71% female), age (62 vs 61 years) or disease duration (13 years).
Patient characteristics
Table 1 shows characteristics of patients with the different diagnoses. The proportion of female patients ranged from 42% in AS to 89% in SLE and SSc. SLE had the lowest mean age at 47 years, while patients with PMR were the oldest at an average of 73 years. Patients with PMR were also those with the shortest mean disease duration (5 years). The other diagnoses ranged from 11 to 18 years with AS having the longest disease duration.
RAID distribution
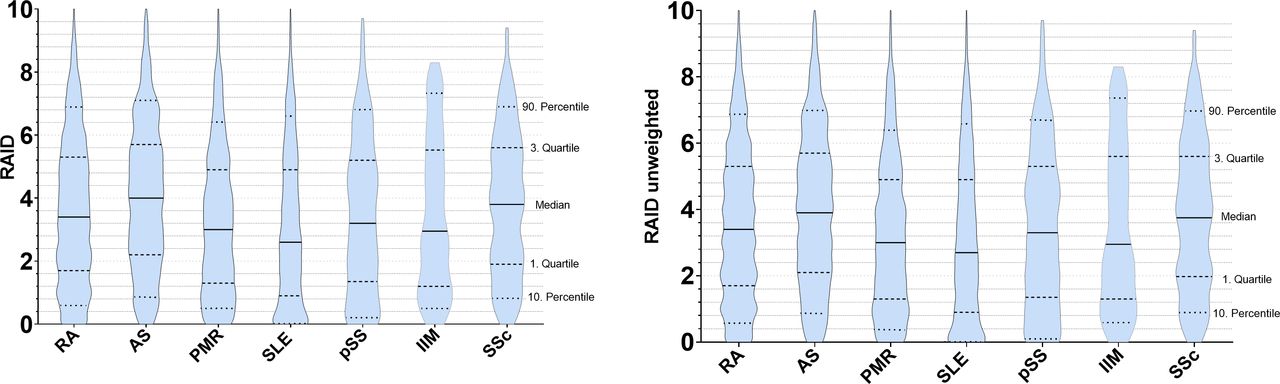
The median (weighted) RAID score in RA (3.4) was lower (better) than in AS (4.0) and SSc (3.8) and higher (worse) than in PMR (3.0), SLE (2.6), pSS (3.2) or IIM (2.9), with SLE having the lowest median. With the exception of SLE and IIM, the mean RAID score was higher in women than in men (data not shown). Figure 1 shows the distribution of the weighted and unweighted RAID composite score at each diagnosis. Overall, the weighted and unweighted scores were very similar and only differed in the second decimal place when comparing mean values. Both were not normally distributed, positively skewed for all diagnoses. Similarly, relevant floor effects were observed in all diagnoses, although these were most pronounced in SLE and IIM. A total of 16% (AS) to 30% (SLE) (RA: 22%) had a score between 0 and 1, and 25% (AS) to 32% (PMR) (RA: 29%) between 1 and 2, whereas only 4% (SLE) to 9% (IIM) (RA: 6%) had scores between 8 and 9, and 0% (IIM) to 3% (AS) (RA: 2%) 9 and 10, respectively.

Violin plots displaying the distribution of the original weighted and the alternative unweighted rheumatoid arthritis impact of disease (RAID) composite score for different diagnoses. The violin plot depicts distributions of numeric data using density curves. The width of each density curve corresponds with the approximate frequency of data points in each region. The lower and upper dashed lines represent the first and third quartiles with the middle 50% of the data in between. The line in the middle shows the median. AS, ankylosing spondylitis; IIM, idiopathic inflammatory myositis; PMR, polymyalgia rheumatica; pSS, primary Sjögren’s syndrome; RA, rheumatoid arthritis; SLE, systemic lupus erythematosus; SSC, systemic sclerosis.
Partial correlation between RAID and other scores
For each of the diagnoses, the RAID correlated most strongly with the PtGl health status (r=0.71–0.83). As in RA, a strong correlation was also found between the RAID and PtGl disease activity in AS, SLE, pSS and SSc (r=0.71–0.79), while in patients with PMR and IIM had a moderate correlation (r=0.59). Similar to RA, the RAID also showed a strong correlation with the WHO-5 score in AS, IIM and SSc and a moderate correlation in SLE, PMR and pSS. Across all diagnoses, the RAID correlated moderately to strongly with the EQ-5D and weakly with the PhGl disease activity. In patients with RA, DAS28-ESR values correlated moderately with the RAID score (0.51, n=6250) and in AS patients, BASDAI values correlated strongly with the RAID score (0.85, n=1298) . In summary, after adjusting for age and sex, the RAID correlated with the analysed scores comparably to RA, strongest for AS and weakest for PMR (figure 2).

Age-adjusted and sex-adjusted partial correlation coefficients between the raid score and other patient-reported and physician-reported outcomes. 0.3–0.5 weak, 0.5–0.7 moderate, >0.7 strong correlation. EQ-5D, EuroQoL-5 Dimensions; IIM, idiopathic inflammatory myositis; PhGl, physician global; PMR, polymyalgia rheumatica; pSS, primary Sjögren’s syndrome; PtGl, patient global; RA, rheumatoid arthritis; SLE, systemic lupus erythematosus; SSC, systemic sclerosis; WHO-5, WHO Well-Being Index.
Differences between the RAID and other outcomes
Figure 3 shows the differences between the RAID composite score and the other patient-reported or physician-reported outcomes. Small mean differences were found between the RAID and either PtGl disease activity (0 to −0.6; RA: −0.1), PtGl health status (−0.4 to −0.9; RA: −0.5) or WHO-5 (−0.7 to −1.3).
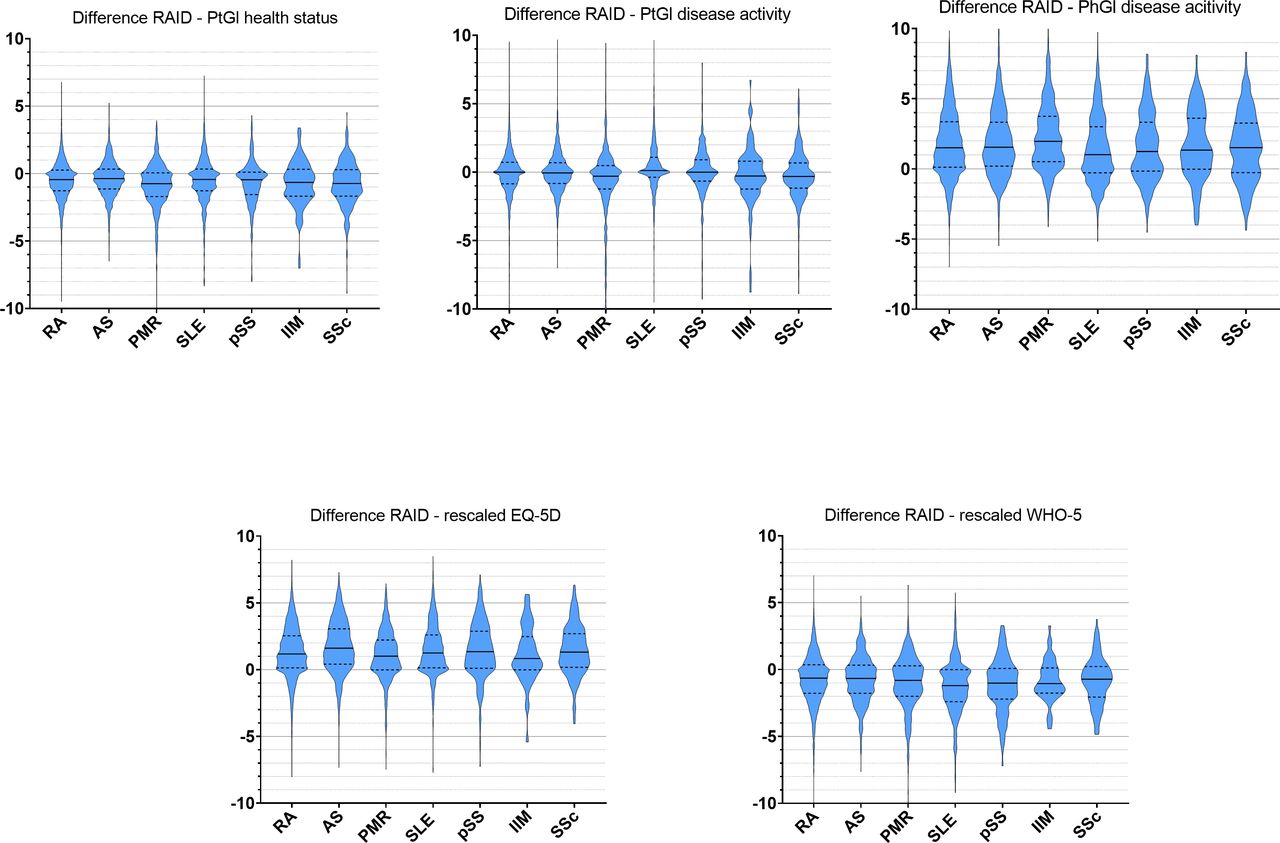
Differences between raid und five outcomes (PtGl health, PtGl disease activity, PhGl disease activity, WHO-5, EQ-5D). The difference was calculated as raid minus the respective outcome. The lower and upper dashed lines represent the first and third quartiles with the middle 50% of the data in between. The line in the middle is the median. AS, ankylosing spondylitis; EQ5-D, EuroQoL-5 Dimensions; IIM, idiopathic inflammatory myositis; PhGl, physician global; PMR, polymyalgia rheumatica; pSS, primary Sjögren’s syndrome; PtGl, patient global; RA, rheumatoid arthritis; SLE, systemic lupus erythematosus; SSC, systemic sclerosis; WHO-5, WHO Well-Being Index.
The EQ-5D (1.1 to 1.7; RA: 1.3) deviated slightly more from the RAID, while the biggest differences were found between the RAID and the PhGl disease activity (1.4 to 2.2; RA: 1.8). However, the discrepancies between the five outcomes and the RAID turned out to be similar across all diagnoses and were comparable to RA. All values are reported in online supplemental table 2.
Linear regression models
Figure 4 shows the results of linear regression models assessing the age-adjusted and sex-adjusted effect of each of the diagnoses on the difference between the RAID score and the five other scores with RA as reference diagnosis. The regression models revealed no clinically relevant effect of any of the diagnoses on the differences between the RAID and the other outcomes.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Linear regression models. The dependent outcome variable is the difference between the RAID score and the five respective outcomes determined as: RAID minus PtGl health status (A), RAID minus PtGl disease activity (B), RAID minus PhGl disease activity (C), RAID minus EQ-5D (D), RAID minus WHO5 (E). Independent variables were sex, gender and diagnosis with RA as reference category. An effect of a diagnosis was defined as clinically relevant if the outcome deviated from the RAID more than one unit than it did for patients with RA (grey area). AS, ankylosing spondylitis; EQ5-D, EuroQoL-5 Dimensions; IIM, idiopathic inflammatory myositis; PhGl, physician global; PMR, polymyalgia rheumatica; pSS, primary Sjögren’s syndrome; PtGl, patient global; RA, rheumatoid arthritis; SLE, systemic lupus erythematosus; SSC, systemic sclerosis; WHO-5, WHO Well-Being Index.
Discussion
This study is the first to analyse the application of the RAID composite score in patients with six inflammatory rheumatic diseases and compared performance to that in RA. Our findings support the use of the RAID for measuring the impact of disease on quality of life not only in RA, but also in AS, SLE, PMR, pSS, IIM and SSc. Our data also show that the unweighted RAID score has comparable properties to the weighted score.
The observed mean and median RAID scores in AS, SLE, PMR, pSS, IIM and SSc differed from those in RA. The lower RAID scores in SLE could be explained by the younger age of the patients. The higher RAID scores in AS may be related to the high number of AS patients in the NDB with long-standing illness and a considerable functional impairment. This is also supported by the high correlation with the BASDAI. However, poorer PROs are also found in other studies when compared with RA.19 20
Across all diagnoses, the RAID distribution is characterised by a positive skewedness and a more or less pronounced floor effect. This effect was also found in other studies18 21 but not in the original RAID validation study.1 A floor effect could be a limitation of the RAID, but applies equally to RA and the diagnoses investigated in this study and often occurs in health status measures.18 We examined an alternative unweighted RAID score and found that the distribution was very similar to the original one which is in line with the analyses the authors of the RAID performed in the peer-review process.7
Across all diagnoses, we found moderate to strong correlations between RAID and patient- or physician-reported measures. As expected and similar to RA, RAID correlated only weakly with physician-reported disease activity. The strongest correlation was with PtGl health status which was also found for RA.1 3 18 21 The RAID score also correlated strongly with PtGl disease activity in patients with AS, SLE and pSS, which supports Heiberg’s perception18 of the RAID as a global measure and its increasing use as an indicator for disease activity in RA.2 PMR and IIM stand out with a moderate correlation, which for PMR could be related to the lack of stiffness in the RAID domains. Similarly, muscle symptoms are cardinal features in IIM and included in the core set,22 but are not part of the RAID which may limit its use as an activity score.
As expected and found in other studies, quality of life, measured with the EQ-5D, and the related concept of well-being, measured with the WHO-5, were found to be moderately to strongly inversely correlated with impact of disease.6 18 The correlation of the RAID and WHO-5 in patients with RA was stronger than in SLE, PMR and pSS. However, the differences in the coefficient were very small. Underlining these results, regression analyses found no clinically relevant effect of any of the diagnoses on the agreement between RAID and all the investigated outcomes. It is important to note here that this analysis does not imply that the scores all measure the same. A different distribution of the individual scores is to be expected. With the calculation of the mean differences and the regression analysis we assessed whether the expected deviations for the examined rheumatic diseases are clearly different to RA. This would indicate that the RAID is not eligible to measure the impact of the diseases. However, the differences compared with RA are very small, so that we can assume that the RAID for the selected diseases depicts the outcomes to a comparable extent as for RA.
Limitations and strengths
Within the framework of a large epidemiological database, we were able to calculate the RAID score for a high number of patients with RA, AS, SLE, PMR, pSS, IIM and SSc. However, due to the character of the NDB as a long-term monitoring database illustrating the routine rheumatological care in Germany, we had a proportion of missing RAID values of up to 33%. As it is not compulsory in the NDB for the patient to fill in the RAID, this percentage corresponds to the procedure of the participating rheumatologists and does not necessarily argue against the feasibility of the RAID in routine care. Some analyses however, for example on WHO-5 in IIM, should be interpreted with caution due to small case numbers.
One of the strengths of the RAID is the participation of patient research partners in the development of the instrument. It reflects the domains that are most important to patients with RA and considers the weighting of each domain according to the patient’s assessment. Therefore, an important step in the development process is lost if the RAID is simply used for other, not validated diseases. This leads to important outcomes like stiffness in PMR, muscle symptoms in IIM or dryness in pSS not being adequately represented. For this purpose, numerous disease-specific standardised and validated quality of life measures or even core sets in the area of life impacts are available, for example, for IIM22 or the Impact Tracker for SLE.23
However, there is no consensus on how to measure the impact of disease using a single composite score with little respondent burden like the RAID. The more complex scores are rarely used in daily clinical practice. The usefulness of the RAID as an impact indicator beyond RA is supported by its individual domains, which have long been part of clinical rheumatology and have proven valuable, such as the measurement of pain and function.24 25
Others like fatigue are already part of established core sets of outcomes.22 26 27 If not yet included in core sets, they have been defined as important28–31 or they are part of a research agenda.32 Patients indicated that the domains work, relationships with others (such as family and friends) and spare time/hobbies were missed in the RAID and could be added to obtain a more ‘complete’ picture of the impact of the disease.33
Conclusions
Our results suggest that the RAID performs comparably well across all investigated diagnoses in comparison to RA. Our data also showed the unweighted RAID score to have comparable properties to the weighted score, which would improve its feasibility in the clinical routine. Given the growing popularity of PROs and the fact that rheumatologists increasingly need to collect them, it is necessary to determine measures which are feasible, reliable and sensitive in the clinical setting. The RAID meets these requirements and can be used to measure the impact of disease for AS, PMR, SLE, pSS, IIM and SSc as well, if no diagnosis-specific alternative is available.
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Ethics committee of the Charité University Medicine Berlin ID EA1/196/06. Participants gave informed consent to participate in the study before taking part.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @callhoffj
Contributors JC is responsible for the overall content as guarantor. KT and JC had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. Study concept and design: KT, KA, JC, AZ. Acquisition, analysis or interpretation of data: KT, KA, AZ, MA, SS, KK, UvH, JC. Drafting of the manuscript: KT, KA, JC. Critical revision of the manuscript and approval of the manuscript: KT, KA, AZ, MA, KK, UvH, SS, JC.
Funding The National Database of the German Collaborative Arthritis centers is supported by the Association of Regional Cooperative Rheumatology Centres, the German Society for Rheumatology and joint contributions to the Rheumatological Training Academy and the German Rheumatism Research Centre by the following members of the Working Group of Corporate Members of the German Society for Rheumatology: AbbVie, AstraZeneca, BMS, GALAPAGOS, GSK, Lilly, Medac, MSD, Pfizer, Sanofi-Aventis and UCB.
Competing interests KT, KA, AZ, MA, KK and UvH: None declared, SS: Speakers bureau: BMS, Gilead, GSK, Janssen, Lilly, Novartis, Pfizer, Sanofi, UCB, Consultant of: Abbvie, Gilead, GSK, UCB, Novartis. JC: Paid instructor for Rheumatologische Fortbildungsakademie GmbH, Grant/research support from Abbvie, AstraZeneca, BMS, GALAPAGOS, GSK, Lilly, Medac, MSD, Pfizer, Sanofi, UCB.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.