Article Text

Abstract
Objective To examine the risk and risk factors of mortality in patients with rheumatoid arthritis (RA) with interstitial lung disease (ILD).
Methods Using the 1997–2013 Taiwanese National Health Insurance Research Database, we identified 32 289 incident patients with RA by using International Classification of Diseases, Ninth Revision codes from 2001 to 2013, and 214 patients developed ILD subsequently. We matched (1:10) RA-ILD with controls for sex, age, time of ILD diagnosis and disease duration. In addition, we conducted propensity score matching (PSM) (1:1) for selected comorbidities to choose RA-ILD patients and controls. Using the Cox proportional hazard model, we estimated the association of mortality with ILD for the two matched populations and assessed factors associated with mortality among 214 RA-ILD patients, shown as adjusted HRs (aHRs) with 95% CIs.
Results In the populations selected before and after PSM, we included 164 and 155 patients with RA-ILD and 1640 and 155 controls, respectively. ILD was associated with mortality in the population before PSM (aHR, 1.73; 95% CI 1.19 to 2.52) and in the PSM population (HR 4.38; 95% CI 2.03 to 9.43). Among 214 patients with RA-ILD, age (aHR 1.04; 95% CI 1.03 to 1.08), chronic obstructive pulmonary disease (COPD) (aHR 2.12; 95% CI 1.25 to 3.58), diabetes mellitus (DM) with end-organ damage and corticosteroid dose (prednisolone equivalent, mg/day) (aHR 1.09; 95% CI 1.07 to 1.11) were associated with mortality in RA-ILD.
Conclusion This population-based cohort study showed that ILD was associated with risk of mortality in patients with RA, and risk factors associated with mortality in patients with RA-ILD included age, COPD, DM with end-organ damage and average daily prednisolone dose.
- arthritis, rheumatoid
- antirheumatic agents
- glucocorticoids
- pulmonary fibrosis
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC?
Rheumatoid arthritis-related interstitial lung disease (RA-ILD) is associated with increase mortality risk. However, there were limited data on the incidence and risk factors for RA-ILD mortality and the sample size for previous studies were pretty small.
WHAT THIS STUDY ADDS?
This study investigated the incidence and risk factors for RA-ILD mortality on both patient-specific and treatment-specific variables by using a population-based database.
We found that ILD was associated with risk of mortality in patients with RA.
The risk factors associated with mortality in patients with RA-ILD included age, chronic obstructive pulmonary disease (COPD), diabetes mellitus (DM) with end-organ damage and average daily prednisolone dose.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY?
More judicious use of steroids among elderly patients with RA-ILD.
Screening for comorbidities of COPD and DM with end-organ damage as part of the routine in treating RA-ILD population.
Research on the effect of RA treatment on RA-ILD mortality is needed.
Introduction
Rheumatoid Arthritis (RA) is a systemic autoimmune disease affecting about 0.46% of the worldwide population.1 The most common extra-articular manifestation of RA is lung involvement, which comprises up to 60% of the RA population.2 3 Basically, any part of the lungs can be affected, that is, pleura, parenchyma, airways and pulmonary vasculatures. Lung parenchyma is the most commonly affected compartment causing interstitial lung disease (ILD). The incidence and prevalence of RA-ILD varied widely due to variable case definitions and sample sizes. A systemic review showed the prevalence of RA-ILD ranged from 1.8% to 67% (median: 24.9%).4 The incidence of RA-ILD in Taiwan’s nationwide population-based cohort study was 0.7%, with an incidence rate ratio (IRR) of 9.05.5 A recent meta-analysis by Qiu et al6 has shown 10 factors associated with increased risk of mortality in RA-ILD: older age, male sex, smoking history, lower diffusing capacity of the lung for carbon monoxide, lower forced vital capacity predicted, higher composite physiological index, usual interstitial pneumonia (UIP) pattern on high-resolution CT, emphysema presence and acute exacerbation of ILD. However, the majority of the studies were single-centre studies. There were very limited studies on the influence of treatment, especially biological therapy, on mortality in RA-ILD.7 8
We conducted a nationwide, population-based cohort study to compare the incidence of death between RA patients with ILD and RA patients without ILD. We also examine the predictors of RA-ILD mortality, concentrating on patient-specific variables and treatment-specific variables, by using the Taiwanese National Health Insurance Research Database (NHIRD).
Methods
Study design
This was a nationwide, population-based, matched cohort study.
Data source
Claims data from 1997 to 2013 were retrieved from the Taiwanese NHIRD. Since 1995, the National Health Insurance (NHI) was initiated in Taiwan. It is a compulsory insurance programme covering 99% of the Taiwanese population. The National Health Research Institute manages the NHIRD and releases claims data for research purposes and The Bureau of NHI routinely audits and monitors claims data to avoid the inclusion of fraudulent data.
The NHIRD contains registration files and comprehensive claims data for all ambulatory and inpatient services, including information regarding demographics, residence, prescription medications, diagnoses, medical expenditure, surgeries, procedures and examinations. All patients with major illnesses are registered in the catastrophic illness registry if the categorisation is agreed on regardless of disease severity after a thorough review of original charts by two independent specialists. There after, a catastrophic illness certificate will be issued to these patients whom the medical services expenses will be exempted.
Patients identifications from the entire Taiwan population
Patients with RA who were registered in the catastrophic illness registry (International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) codes 714.0, 714.30–714.33) were retrieved. All patients newly diagnosed with RA from 2001 to 2013 were included. Exclusion criteria were a diagnosis of ILD (ICD-9-CM codes 515, 516.3, 516.8, 516.9, 517) before the time of RA diagnosis or overlapping diagnosis of systemic autoimmune rheumatic diseases, including systemic lupus erythematosus (ICD-9-CM code 710.0), Sjogren’s syndrome (ICD-9-CM code 710.2), dermatomyositis (ICD-9-CM code 710.3), polymyositis (ICD-9-DM code 710.4) and systemic sclerosis (ICD-9-CM code 710.1). The index date for patients with RA was defined as the RA catastrophic illness certificate application date.
Definition of ILD
Patients with RA identified above will be further divided into ILD and non-ILD groups. In order to improve the validity of ILD diagnosis, we defined ILD as follows: (1) at least one outpatient or inpatient visit using ICD-9-CM code 515, 516.3, 516.8, 516.9 or 517 and (2) a radiological or pathological diagnosis using the appropriate NHI code (online supplemental table A) within 6 months before or after the first date of diagnosis. If the radiographic or pathological ILD diagnosis was made after the first outpatient or inpatient visit, we required at least another outpatient or inpatient visit with ILD diagnosis. Exclusion criteria were those without insured amount and those without urbanisation categorisation. The index date was the first date of ambulatory or inpatient visit with an ILD diagnosis.
Supplemental material
Age, sex, year of ILD diagnosis and disease duration-matched RA population
We matched (1:10) RA-ILD patients with RA patients without a diagnosis of ILD during the follow-up period for age, sex, year of ILD diagnosis date and disease duration.
Propensity score-matched RA population
In addition, using the 1:10 matched RA population mentioned above, we conducted propensity score matching (PSM) for the comorbidities used to calculate the Charlson Comorbidity Index at a ratio of 1:1 to select another RA population to examine the influence of ILD on mortality in patients with RA.
Outcome
The primary outcome was mortality for both groups of patients during the study periods. Data were censored on 31 December 2013 or on the withdrawal date from the NHI for any reason, whichever came first.
Potential confounders
Potential confounders for this study included age, sex, disease duration, urbanisation level of residence, income, comorbidities and medications for RA treatment. The urbanisation level of a residence was categorised according to population density (people/km2); the proportion of agricultural workers, participants with an educational level above college and elderly (aged >65 years); and the number of physicians/105 individuals.9 The payroll-related insured amount was used as a proxy of income and was transformed into a categorical variable with two levels. The comorbidities used to calculate the Charlson Comorbidity Index were considered potential confounders.10 The presence of comorbidity was defined as having at least one hospitalisation or at least three ambulatory visits with a corresponding ICD-9-CM code within 1 year before the index date. The ICD-9-CM codes of comorbidities are shown in online supplemental table A. RA-related medications included corticosteroids, non-steroidal anti-inflammatory drugs (NSAIDs), cyclophosphamide, other immunosuppressants (ciclosporin, azathioprine, mycophenolate and mycophenolic acid), conventional synthetic disease-modifying anti-inflammatory drugs (DMARDs) (methotrexate, sulfasalazine, leflunomide and hydroxychloroquine) and biological DMARDs (tumour necrosis factor inhibitor (TNFi), tocilizumab, abatacept and rituximab). Use of RA-related medications at baseline was identified within 1 year before the index date and was adjusted as categorical variables, which may serve as a proxy of baseline RA disease activity. We also adjusted time-averaged dose of RA-related medications during the follow-up period (ie, NSAID, cumulative defined daily dose (cDDD)/day; corticosteroid, prednisolone equivalent dose, mg/day; methotrexate, per 2.5 mg/week, sulfasalazine, cumulative dose/500 mg/day; leflunomide, cDDD/day; cyclophosphamide, cumulative dose/500 mg/month, other immunosuppressant, cDDD/day; TNFi, cDDD/day; tocilizumab, cDDD/day; abatacept, cDDD/day; rituximab, cumulative dose/500 mg/6 months).
Statistical analysis
Continuous variables are presented as mean±SD while categorical data are presented as the percentage of subjects. The χ2 test was utilised to evaluate differences between categorical variables whereas the Student’s t-test was used for continuous variables. The mortality of RA-ILD or RA-non ILD was taken as the number of subjects’ death events in percentage. The IRRs and their corresponding 95% CIs were evaluated. Finally, the association of mortality with ILD was assessed using the multivariable Cox regression analysis shown as adjusted HR (aHR) with 95% CIs adjusting for potential confounders. In the PSM population, we conducted a conditional Cox regression analysis to estimate the influence of ILD on the risk of mortality. To examine the impact of covariates on mortality among 214 patients with RA-ILD, we conducted a multivariable Cox regression analysis adjusting for the covariate with a p<0.05 in the univariable Cox regression analysis.
Results
Baseline characteristics
In total, we identified 214 patients with RA-ILD and 30 882 RA-non ILD patients after excluding the criteria mentioned above. Figure 1 shows the flow chart of subject identification. After matching the age of RA, age of ILD diagnosis, gender and disease duration, we were able to identify 164 and 155 patients with RA-ILD patients in the age, sex, year of ILD diagnosis date and disease duration-matched population and the PSM population, respectively. The mean±SD disease duration from RA diagnosis to ILD detection was 3.5±2.8 years. The demographic and clinical characteristics of the study subjects, including the level of urbanisation, patient income, comorbidities and medications, are shown in table 1.

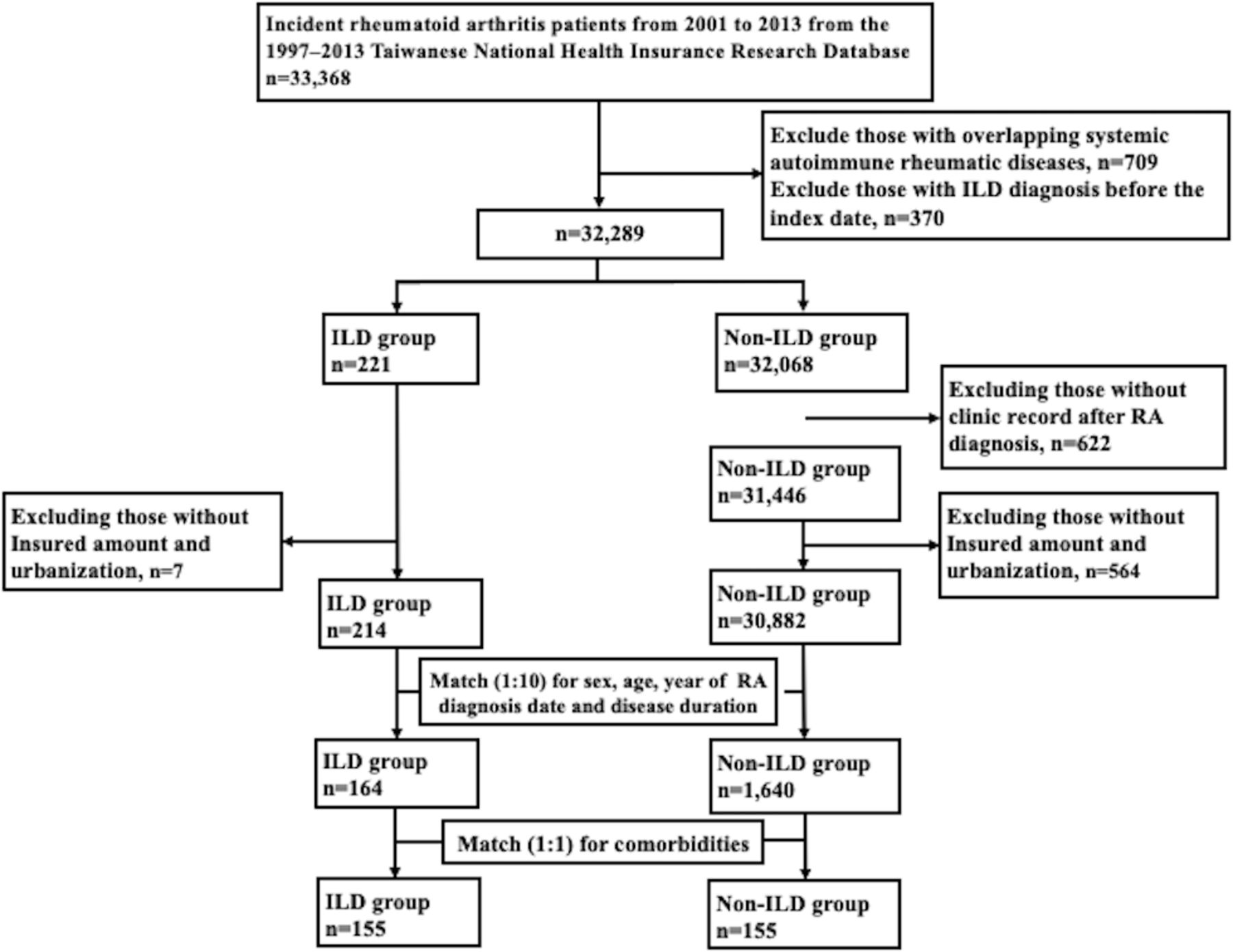{kind=link}
Study subject identification flow chart. ILD, interstitial lung disease; RA, rheumatoid arthritis.
Incidence rates of death in study subjects
Incidence of mortality in RA patients with ILD and RA patients without ILD
As seen in table 1, the mortality rate was significantly higher in the RA-ILD group compared with the non-ILD group, with the IRR of 2.66 in the pre-PSM population and 2.55 in the PSM papulation. Among the population before PSM, we found that ILD was significantly associated with the risk of mortality in patients with RA in the univariable model (crude HR 2.69; 95% CI 1.97 to 3.68) and in the multivariable model (aHR 1.73; 95% CI 1.19 to 2.52) using the Cox regression analyses. In the PSM population, ILD was significantly associated with the risk of mortality in patients with RA using the conditional Cox regression model.
Factors associated with mortality in patients with RA-ILD
Online supplemental table 2 indicates the demographics and clinical characteristics of RA-ILD patients, whereas online supplemental table 3 summarises the Cox proportional regression analysis of factors associated with mortality. For patient demographic factors, predictors of mortality included age at ILD diagnosis. With regard to comorbidities, dementia and diabetes mellitus (DM) with end-organ damage were significantly associated with higher mortality across all models. Regarding RA-related medications, only a time-averaged dose of corticosteroid during the follow-up period was significantly associated with mortality in patients with RA-ILD.
Discussion
This nationwide, population-based study showed that ILD significantly increased the risk of mortality in patients with RA, with aHR of 1.73 in the age, sex, disease duration-matched population and 4.38 in the PSM population. The mean±SD age at ILD diagnosis was 64.2±14.2 years. These results were consistent with most of the systematic reviews as well as meta-analyses on RA-ILD mortality risk factors.6 11–13 The explanation for the high mortality rate in RA-ILD populations is multifactorial. The majority of patients with RA-ILD comprise of UIP pattern, which itself is a poor prognostic factor.14–16 The most common radiological features in UIP are subpleural and basilar predominant reticular abnormalities, honeycombing and traction bronchiectasis with rarely ground-glass opacification. Of note, UIP is also a feature of idiopathic pulmonary fibrosis (IPF).17 A recent article found a similar genetic susceptibility between IPF and RA-ILD.18 Exacerbation of ILD and recurrent lungs infection also increases the risk of mortality in RA-ILD.6
Our study found a significant association between mortality and older age, which is consistent with meta-analysis data.6 Other patient-specific variables which significantly increase RA-ILD mortality are comorbidities of chronic obstructive pulmonary disease (COPD) and DM with end-organ damage. There is growing evidence that the autoimmune pathway is playing a significant role in emphysema, especially in the RA population.19 20 COPD increased mortality in patients with RA had been shown in a recent Danish population-based study.21 A few studies also showed a poorer prognosis in RA-ILD with the presence of emphysema.22 23 Smoking is a known risk factor for COPD and it represents a confounder for the association between COPD and RA-ILD mortality. The prevalence of DM is increased in patients with RA, and there is a strong linkage between RA insulin resistance and systemic inflammation induced by proinflammatory cytokines.24 25 There is an association between DM and ILD/IPF with an unknown mechanism.26 Our study has shown that DM with end-organ damage increased RA-ILD mortality. Further study is needed to explore the pathophysiology linkage between DM and RA-ILD.
There are only very limited studies on RA treatment as predictor for RA-ILD mortality. There were also a controversy with regards to the effect of conventional DMARDs and biological DMARDs on RA-ILD onset, progression and mortality.7 27–29 Our report showed average daily prednisolone dose increased RA-ILD mortality. One of the reasons of this association might be due to risk of infections with increase prednisolone usage.30 Indirectly, it also reflected on increased RA or ILD activity which directly affecting the mortality in RA-ILD group.
There are few limitations in this study. First, lack of smoking data which represents an unmeasured confounder for RA-ILD mortality. However, we have assessed the association of RA-ILD mortality with smoking-related comorbidities, which may partially reflect the impact of smoking. Second, the diagnosis of RA and ILD may be questionable from claim data. We had overcome this by identifying patients with RA and ILD from the catastrophic illness registry whereby the diagnosis of RA had been confirmed by at least two rheumatologists after careful review of original medical records. Third, asymptomatic RA-ILD might went undetected due to the lack of standardised screening methods. Finally, the study results might not be able to be generalised to non-Taiwanese populations.
In conclusion, this is one of the few population-based cohort studies to analyse the predictors of RA-ILD mortality. Our data confirm that older age of ILD diagnosis is a strong predictor of mortality in patients with RA-ILD. We found associations of mortality with COPD and DM end-organ damage among patients with RA-ILD. In terms of treatment-specific variable, average daily prednisolone dose carried a worst prognosis. Further studies are required to study the pathophysiology link between DM and RA-ILD as well as the effect of RA treatments on RA-ILD progression and mortality.
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information.
Ethics statements
Patient consent for publication
Ethics approval
This study was approved by the Institutional Review Board (IRB) of Taichung Veterans General Hospital (IRB number: CE17100B). The requirement for informed consent was waived because detailed personal information was completely anonymised before data analysis.
Acknowledgments
The study is based on data from the NHIRD provided by the National Health Insurance Administration and the Ministry of Health and Welfare and managed by the National Health Research Institutes. The interpretation and conclusions do not represent those of the National Health Insurance Administration, the Ministry of Health and Welfare or the National Health Research Institutes. The authors would like to thank the Biostatistics Task Force of Taichung Veterans General Hospital, Taichung, Taiwan, ROC for statistical support. This study has been presented as an abstract at the EULAR 2022 Congress. Chen HH, Chen DYPOS0578. Risk and risk factors of mortality in rheumatoid arthritis patients with interstitial lung disease: a nationwide, population-based cohort study. Annals of the Rheumatic Diseases 2022;81:555.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors C-HL analysed the data and generated figures. K-HN analysed the data and wrote the manuscript. D-YC, C-HL and W-CC performed bioinformatics analysis and wrote the manuscript. H-HC designed the study, conducted data analysis and wrote the manuscript. H-HC is responsible for the overall content as the guaranto. The guarantor accepts full responsibility for the work and/or the conduct of the study, had access to the data, and controlled the decision to publish. All authors read and approved the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.