Article Text

Abstract
In each era we need to balance between being able to provide care with our “technical skill, scientific knowledge, and human understanding” (Harrison's Principles of Internal Medicine, 1950) to the individual patient and simultaneously ensure that our healthcare serves all. With the increasing demand of healthcare by an aging population and the lack of specialists, accessible healthcare within a reasonable time frame is not always guaranteed. E-health provides solutions for current situations where we do not meet our own aims of good healthcare, such as restrictions in access to care and a reduction in care availability by a reducing workforce. In addition, telemedicine offers opportunities to improve our healthcare beyond what is possible by in person visits. However, e-health is often viewed as an deficient version of healthcare of low quality. We disagree with this view. In this article we will discuss how to position e-health in the current situation of healthcare, given the continuing rapid development of digital technologies and the changing needs of healthcare professionals and patients. We will address the evolution of e-health towards connected and intelligent systems and the stakeholders perspective, aiming to open up the discussion on e-Health.
- autoimmune diseases
- arthritis
- therapeutics
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
With the increasing possibilities offered by digital techniques, the traditional way of practising medicine is changing. Thanks to a growing number of devices and user interfaces, e-medicine completes the moment-dependent medicine in the form of consultations by continuously providing longitudinal information and thus completing the patient journey.1
To date, a substantial part of healthcare providers consider e-health in the form of video consultations, telemonitoring of patient-reported outcomes (PROs), chatbots or automated decision support by artificial intelligence as an deficient version of healthcare of low quality.2 3 There is also concern that machine learning algorithms will take away jobs or lead to unethical care.
We disagree with this view and believe that e-health can improve the current quality of care and meets unmet needs. In this article, we will discuss the current situation of healthcare and how to position e-health, given the continuing rapid development of digital technologies and the changing needs of healthcare professionals and patients.
What is good healthcare?
The role of physicians in healthcare is described in Harrison as follows:
As today’s physicians strive to integrate copious amounts of scientific knowledge into everyday practice, it is critically important that they remember two things: first, that the ultimate goal of medicine is to prevent disease and treat patients; and second, that despite more than 60 years of scientific advances since the first edition of this text, cultivation of the intimate relationship between physician and patient still lies at the heart of successful patient care.
The description focuses on the importance of the interaction between physicians and patients and less on the perhaps more general responsibility of healthcare towards society. The European Alliance of Associations for Rheumatology (EULAR) does take this into account in their statuses 2021:
EULAR aims to reduce the impact of rheumatic and musculoskeletal diseases (RMDs) on the individual and society and to improve the social position and the quality of life of people with rheumatic and musculoskeletal diseases in Europe.
But in clinical practice, time is often too short to establish an interpersonal connection with the patient and to assess social status and quality of life sufficiently. Accessible healthcare within a reasonable time frame is not always guaranteed, due to the increasing demand of healthcare by an ageing population and the lack of specialists. This creates not only frustration, but also loss of valuable information about patients.
In addition, the demands on quality of life in an on-demand society are increasing, making that we see more patients with fewer symptoms.4 Simultaneously, the burden that can be carried by the healthcare working force is decreasing: the average workweek in the EU is getting shorter, there is a decrease in popularity of nursing schools and a reduction in life long careers in healthcare.5–7
These trends are not new; in each era, we need to balance between being able to provide care with our ‘technical skill, scientific knowledge and human understanding’8 to the individual patient and simultaneously ensure that our healthcare serves all.
Solutions for the dilemma
What shall we do with this dilemma of lack of time, increased tasks and an increasing need for information and connection? The answer is simple, we must make a virtue out of necessity and benefit from the dynamics that are already taking place. The dynamic with the most impact on healthcare is digitalisation.
The digital revolution has reached healthcare; more and more people use the internet for medical advice and digital lifestyle products such as smartwatches.9 10 These devices can also be used for disease prevention and monitoring. Thus, there is already an ongoing ‘digital health socialisation’.
Digital applications are increasingly used for disease management and therapy of chronic diseases (digital therapeutics, DTX).11 For medication management apps have functions such as treatment reminder or drug interaction detectors. In terms of intervention they mostly focus on lifestyle intervention, cognitive–behavioural therapy and physical therapy. Successful clinical trials have been reported for different diseases, such as psychiatric disorders and osteoarthritis.12–14 DTX also serve for patient education and monitoring. Therefore, DTX should be a first line intervention, rather than an add on for drug therapy.
Finally, digital solutions are tackling the administrative burden for instance by chatbots, automated appointments, voice recognition, recorded conversations or integration of PROs in the electronic medical records (EMRs). Simple tasks like drug renewals can be done by email with automated connection to the prescription system and pharmacies. This time efficiency can benefit the interaction with patients.
Better access to healthcare
Remote care offers solutions for people living in remote underpopulated areas. But also in densely populated European areas it can improve care accessibility. The way we have shaped rheumatology healthcare is fixed around care at one location, during office hours. This is practical from the healthcare professionals’ perspective, but not necessarily from the patients’ perspective, at least, not for all patients. Elderly patients who have difficulties travelling and patients with high demanding jobs or families face difficulties fitting their medical needs within the boundaries of how we provide our care.15 After all, a visit to an outpatient clinic with travelling, parking, waiting time and blood work up, will easily take up half a day. In case elderly are not able to visit, we tend to change disease modifying antirheumatic drugs to lower doses and transfer care to the primary care physician. We might get frustrated with people not showing up at appointments or waiting to seek care, incorrectly concluding that their low health status is due to their irresponsible behaviour. Remote care could meet the needs of patients whose needs we currently do not meet, by providing digital access through our clinics using video consultations and teleconsultations or by improving our support to primary care physicians.
Tailored patient consultations
For the above examples, remote care might still be seen as a suboptimal alternative to the best care, namely in person care. It is true that remotely, clinical or ultrasound exams cannot be performed in the same way. Naturally, e-health cannot replace the empathy from face-to-face conversation, but it still can be preferred by some patients. In addition, we know certain physical information can be better obtained at home, such as blood pressure measurement.16 17 This might also be true for markers of rheumatic diseases. The balance lies in what patients and healthcare professionals need from the consultation in order to prevent or treat diseases appropriately (and not in what we might want to know from a research perspective).18 19 This can be illustrated in three case vignettes :
Scenario 1: Asymptomatic patient, 43 years with rheumatoid arthritis under biologic treatment. In a video consultation symptoms, tolerability of the treatment, drug discontinuation or tapering, vaccination or the cardiovascular risk profile can be discussed. Monthly reported PROs are stable and data from wearables show no signs of reduced mobility.
Scenario 2: A 54-year-old patient with rheumatoid arthritis and secondary fibromyalgia on third line therapy with persisting pain and sensation of joint stiffness and swelling. PROs are catastrophic and wearables show low mobility. Ultrasound of the peripheral joints and a blood examination is needed. The psychological status and factors for fibromyalgia can best be assessed in a face to face consultation.
Scenario 3: A 79-year-old patient with chronic lumbar back pain due to severe spinal stenosis, osteoarthritis, cardiovascular disease and a history of gout as well as unexplained weight loss. Remote PROs are not available. The GPS tracker shows low level, but decreasing mobility. Data from a smartwatch indicate stable vital signs. An interdisciplinary videodiscussion between family doctor, rheumatologist and surgeon clarifies operability, necessary diagnostics, hospitalisation and social environment. The patient is seen by the general practitioner who also knows the family of the patient.
Thus, ‘Cultivating the intimate relationship between physician and patient’8 does not necessarily mean we have to see each patient personally. We suggest discussing with each patient the possibility of videoconsultations with advantages and limitations. In both forms of consultation, as much data as possible and realistic (PROs, wearables, work capacity, blood results, reports from other specialists) should be available to make the best decisions.
Digital solutions such as automatic scheduling and video conferencing can improve interdisciplinarity and the possibility to easily obtain second opinions. Of course, the video consultation as well as the remote monitoring must also be remunerated accordingly in order to fairly reflect the medical service both remotely and in person.
Now the question is how to implement such tailored care in our hospital systems. Should it be completely personalised or could we tailor more on a group level? This could be done by clustering or according to current disease activity and /or predicted DAS28-C reactive protein. More tricky is tailoring taking into account real world data such as PRO. As an example, patients with persisting high PROs (in the absence of fibromyalgia) and ideally confirmation of disease activity by a specific digital biomarker would put the patient on a ‘High Flare Probability List’. In case of an open slot in the consultation (eg, a cancellation), one of those patients will automatically receive a short-term appointment. The implementation will depend on the logistic possibilities and management tasks of individual care systems. But also here it is imaginable that the future will bring new opportunities to allow such flexibility.
Connected care
Collecting longitudinal data can improve our understanding of patient journeys. This information is far more valuable if it is shared between stakeholders. ‘Connected care’ can be seen as the evolution of digital health with interoperable user interfaces (apps, wearable, smartwatches, etc) and EMRs via application programming interfaces.20 ‘Connected health’ is a conceptual model for a patient-centred health management where devices, services or interventions are easily accessible for healthcare professionals and patients (figure 1). Similar to online banking, interoperable apps will likely become the point of connected care. Examples in real life and research setting exist though complete integration into the healthcare systems remain challenging and the apps often focus on one medical specialty.21–25
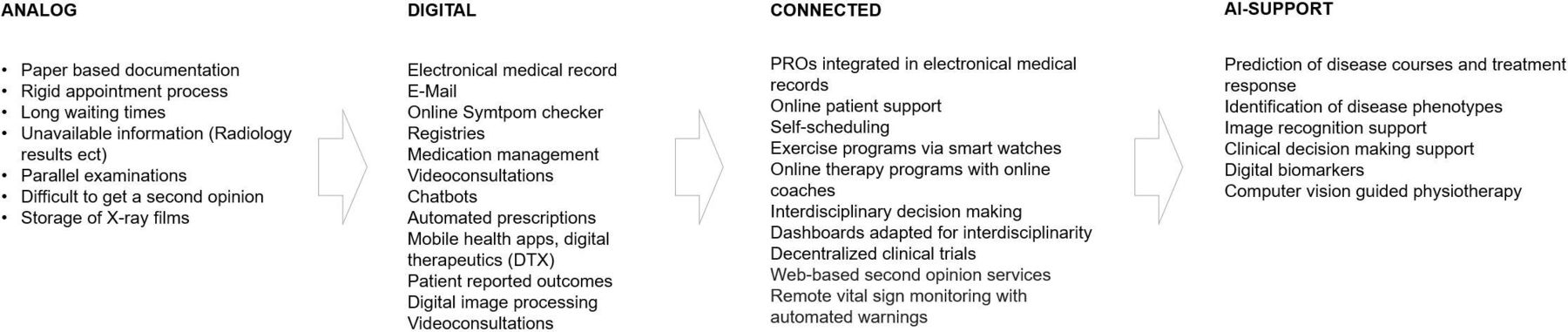
The evolution of e-health towards connected and intelligent systems. PROs, patient-reported outcomes.
Today the communication between healthcare specialists and back to the patient still works via conventional information channels, mostly email or phone. Involved healthcare professionals including doctors, physiotherapists or psychologists literally are not on the same page. Even in hospitals, where physicians of different specialties use the same EMRs, they are not really connected. Current dashboards in EMRs usually do not illustrate disease specific activity of concomitant diseases such as psoriasis, psoriasis arthritis and colitis in a parallel way. We believe that dashboards adapted for interdisciplinary work are necessary which integrate relevant information to understand the patient journey holistically and facilitate interdisciplinary communication between healthcare providers and with patients themselves.
Support by artificial intelligence
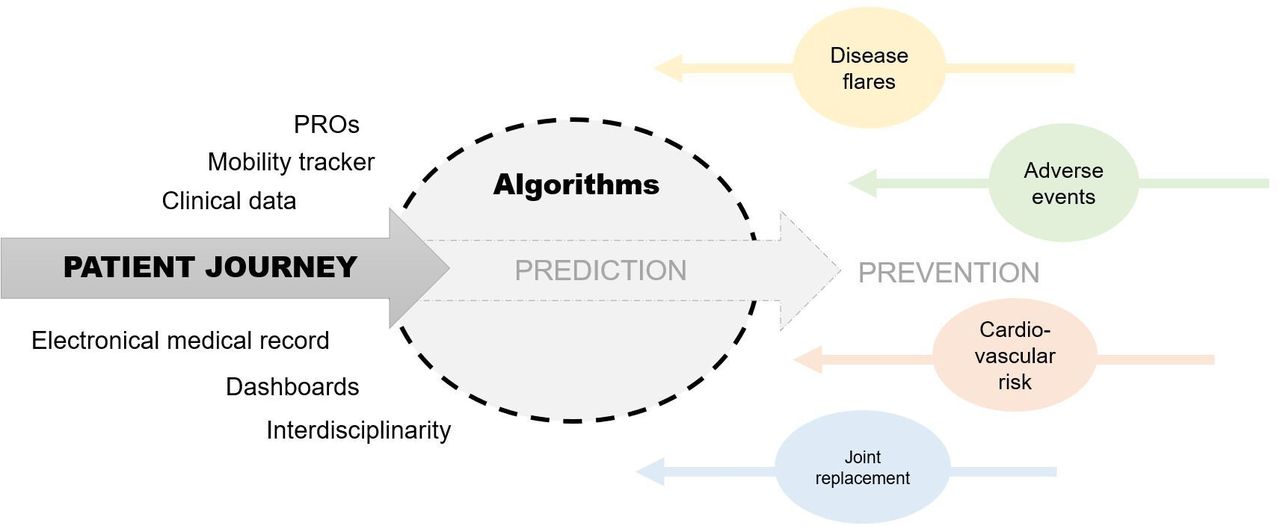
Using remote care, healthcare professionals will be capable of recognising trends by longitudinal data on symptoms or disease activity. The data flood generated by EMRs, apps, etc cannot possibly be acted on by the doctor alone. For optimal exploitation of data machine learning algorithms are necessary.26 Algorithms likely will play a more active role in, for example, clinical decision making, disease phenotyping, treatment and complications prevention(figure 2). Clearly, a shared decision-making process between patient, doctor and machine is necessary and most ideal.27 In regions without adequate patient care, algorithms might help to ensure at least a low level quality of care. In our opinion, machine learning algorithms will remain a ‘mass production tools’ to solve frequent and relatively simple problems and require human assessment of the results. Conversely, machine learning algorithms also can include incoming data via digital biomarkers in semiclosed loop systems in order to create a certain action (eg, apply a methotrexate dose via an implanted device), such as successfully applied in diabetes care.28 29 Importantly, if machine learning models are allowed to make decisions, this has to be under strict rules and high knowledge of the biologic and regulatory environment. The development of such legislations and the ethical standards need to evolve together with the digital evolution and align with the quality of the models at that time. This will require active involvement of all stakeholders and thus an interaction of healthcare professionals and patient organisation with healthcare authorities.

{kind=link}
{kind=link}
E-Health data as a basis for algorithms to predict disease courses and to reduce complications. PROs, patient-reported outcomes.
Stakeholders perspective
Several studies assess the perspective of the main stakeholders (patients with rheumatic diseases and healthcare providers) on existing or theoretical eHealth solutions. The majority of patients view e-Health solutions as (possibly) beneficial to their health provided these solutions are ‘needs-tailored’ and ‘codeveloped by healthcare professionals’.3 30–32 Patients support the notion that e-Health could increase reliability of symptom tracking and information sharing to obtain reliable information about their disease.32 33 Also clinicians support the idea that more detailed disease activity information through e-Health could improve their care.32 In a focus groups study, both patients and healthcare providers (rheumatologists and nurses) verbalised the expectation that e-Health could reduce the number of necessary visits and improve the focus of care to patients’ needs.33 Mentioned limitations were motivational aspects, target group aspects, legal and organisational requirements and the burden of chronic app-use leading to negative illness behaviour. In line with our opinion, a fishbowl study with 476 stakeholders concluded that stakeholders find it important that the ‘final diagnosis and therapeutic decisions should be exclusively made by rheumatologists’.3 Among stakeholders, there are different views on which group of patients would benefit most from digital solutions; those with low disease activity and long-standing disease (as this is a safe group?) or new patients with active disease that need more care than the standard visits?
In addition to assessing the stakeholders viewpoints, it is interesting to quantify the stakeholders experiences, which is a research field on its own.34
In the end, studies summarise a group level preference and expectations which is limited by stakeholders’ previous experiences, imagination and the available tools at that time. With the evolving e-health opportunities we will need to continuously assess the stakeholders’ perspective. But probably most importantly, doctors should discuss with patients the possibilities of e-health including telemonitoring, DIGAs or connected care with all stakeholders ideally at first visits and together decide what is most preferable.
Discussion
Our current healthcare does not meet the standards for accessible care, maximising the use of scientific knowledge and human understanding. Thus, we are not optimally improving ‘the social position and the quality of life of people’. E-health provides solutions to fill these lacunae: it provides flexibility in the way we can provide care whereby we can meet patients desires, it can capture aspects of patients performances which can be missed at in-person assessments and it optimises interactions with and between patients and between specialists.
Is e-health the holy grail? No. It is not a substitute for our current care, we still need to find the right balance between empathic in-person medicine and the systematic integration of data. But e-health can complement and improve care. E-health is a quickly moving field with inevitable suboptimal performance of novel tools. Luckily, the digitalisation in our society is moving fast which will make e-health solutions increasingly workable. Simultaneously, the scientific community is developing standards on how to build implementable machine learning algorithms.35 36 An active discussion supported by scientific studies can help to define how to integrate e-health into healthcare. EULAR conference 2022 set a good example with multiple sessions discussing e-health.
In the discussion on the most optimal use of e-Health in clinic, much can be learnt from other scientific fields such as social sciences. While assessing the current literature and experiences, it is important to distinguish e-health studies that make use of digital solutions for data collection purposes or to serve healthcare. Many of the data-collection-focused studies show low participants adherence comparable to paper diaries and long questionnaire studies.18 Our viewpoint focuses on solutions targeted at improving care. But also there, it remains important that the users are aware and ideally continuously experience the benefits of the e-health solutions in order to optimise adherence (ie, of course not much different from drug usage).
Inevitably, there will be other limitations to e-health that are currently uncertain. Both patients and healthcare providers are concerned about the risk of ‘negative illness behaviour’ fed by too frequent interactions with the healthcare system, target group aspects, and legal and organisational requirement.18 To completely assess these risks, it is advisable to not solely study e-Health from the disease activity perspective but also perform social studies to their impact.
A (current) limitation of e-health is that it requires a certain digital literacy from patients and rheumatologists.37 Digital literacy is quickly increasing, even to the extent that in the (near) future patients might find it easier to find the right care online, then to know how to arrange an appropriate doctor’s visit. This trend is already observed in the USA, where an increasing number of people aged <35 years are not registered at any primary care office.38 39 Particularly this group is keen to sign up for digital healthcare as offered by Amazon.40 This brings us to our final argument: while there is still much to improve in the field of e-health, tech companies are entering ‘our’ playing field; they are providing complete healthcare services online.40 If at some point their care becomes more accessible or meets patients’ (short-term) needs better than our care, it might significantly change the healthcare scene.
For the future, in addition to the discussion how we value e-health solutions, the implementation of these solutions will pose new challenges. Some are already apparent, such as reimbursement questions, outpatient clinic management and data protection. This is topped by heterogeneity between countries in legal, financial and cultural aspects. In our view these challenges will likely be surmountable, but require more detailed discussion in a separate paper.
Conclusion
E-health provides solutions for current situations where we do not meet our own aims of good healthcare, such as restrictions in access to care and a reduction in care availability by a reducing workforce. In addition, telemedicine offers opportunities to improve our healthcare beyond what is possible by in person visits. Are we ready to participate in the digital transition and willing to make our healthcare future proof?41
Ethics statements
Patient consent for publication
References
Footnotes
Contributors Both authors work on content and writing collaboratively.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Commissioned; externally peer reviewed.