Article Text

Abstract
Objectives Evidence on the current status of gender equity in academic rheumatology in Europe and potential for its improvement is limited. The EULAR convened a task force to obtain empirical evidence on the potential unmet need for support of female rheumatologists, health professionals and non-clinical scientists in academic rheumatology.
Methods This cross-sectional study comprised three web-based surveys conducted in 2020 among: (1) EULAR scientific member society leaders, (2) EULAR and Emerging EULAR Network (EMEUNET) members and (3) EULAR Council members. Statistics were descriptive with significance testing for male/female responses assessed by χ2 test and t-test.
Results Data from EULAR scientific member societies in 13 countries indicated that there were disproportionately fewer women in academic rheumatology than in clinical rheumatology, and they tended to be under-represented in senior academic roles. From 324 responses of EULAR and EMEUNET members (24 countries), we detected no gender differences in leadership aspirations, self-efficacy in career advancement and work–life integration as well as the share of time spent on research, but there were gender differences in working hours and the levels of perceived gender discrimination and sexual harassment. There were gender differences in the ranking of 7 of 26 factors impacting career advancement and of 8 of 24 potential interventions to aid career advancement.
Conclusions There are gender differences in career advancement in academic rheumatology. The study informs a EULAR task force developing a framework of potential interventions to accelerate gender-equitable career advancement in academic rheumatology.
- health services research
- qualitative research
- epidemiology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is already known about this subject?
Gender equity can contribute to social progress, quality of science and academic workforce sustainability.
Yet, in many fields of academic medicine, including rheumatology, women remain under-represented, especially in leadership roles.
What does this study add?
The study provides empirical evidence on gender equity in academic rheumatology based on the surveys of EULAR national societies, EULAR and Emerging EULAR Network members and EULAR Council members.
The study proposes and ranks the perceived utility of 24 potential interventions for career advancement in academic rheumatology by gender.
How might this impact on clinical practice?
The study informs an EULAR task force developing a framework of potential interventions to accelerate gender equitable career advancement of rheumatologists, health professionals and non-clinical scientists in academic rheumatology.
Introduction
‘If the fields of science, medicine and global health are to hope to work toward improving human lives, they must be representative of the societies they serve’—The Lancet poignantly argued in its special issue on advancing women in science, medicine and global health.1 Besides this strong social progress imperative, greater gender equity, that is, the societal and institutional process of being fair to women and men,2 can improve quality of science.3 4 The published literature suggests that female research leaders investigate sex-related and gender-related variables more frequently than male research leaders.5 6 Advancing gender equity in clinical practice, research and training is also necessary for the sustainability of the academic workforce. This requires not only recruiting the new generation into the academic workforce but also advancing and promoting the current generation, who may otherwise leave.
This holds particularly true for many fields of academic medicine, including rheumatology, where women remain under-represented, especially in leadership roles.7–20 In many countries, women enter medical school in similar numbers,10 develop a similar interest in research21 and have similar leadership aspirations as men.22 Yet, women may experience the constraints of traditional gender roles,23 gender bias in academic career structures, tenure and promotion criteria, and research funding,24 as well as sexual harassment.25 26 There are further reports of negative aspects of culture in academic medicine,27 a lack of mentors and role models28 and limited advancement opportunities29 that affect all genders, but more so women.30 ‘Unequal pay for equal work’ disadvantaging women in academic medicine is also reported.31 32
The EULAR is ‘the organisation which represents the people with arthritis/rheumatism, health professionals in rheumatology (HPR) and scientific societies of rheumatology of all the European nations’.33 In 2019, EULAR set up a task force to advance the field of gender equity. As part of that task force, a cross-sectional study was conducted to obtain empirical evidence on the extent of the unmet need for support of female rheumatologists, health professionals and non-clinical scientists in academic rheumatology.
Methods
To formulate a data collection strategy, the task force convenor and steering group prepared a narrative literature review on gender equity in clinical practice, research and training10 11 and conducted a web-based survey of task force members to identify potential factors and interventions affecting gender equity in academic rheumatology. These were discussed at the first face-to-face task force meeting in October 2019, and a data collection strategy was agreed by consensus. The data collection strategy included three web-based surveys administered via SurveyMonkey: (1) a survey of EULAR scientific member society leaders to determine the extent of gender equity in the academic rheumatology workforce by country, (2) a survey of EULAR and Emerging EULAR Network (EMEUNET) members to measure individual perceptions of gender equity and career advancement needs and (3) a survey of EULAR Council (formerly Executive Committee) members to assess the perceived utility of potential interventions to aid career advancement. A further description of the survey populations, questions and procedures is given in online supplemental table S1. The exact wording of the questionnaires is given in online supplementary questionnaires 1–3.
Supplemental material
For quantitative analysis, complete survey responses were aggregated and incomplete responses excluded. Do not know/not applicable responses were further excluded from the analysis of individual questions. Analysis included descriptive statistics with comparisons for male/female responses assessed by χ2 test and t-test. The level of statistical significance was set at p <0.001 for data from 5-point scales and at p <0.05 for all other data. Cronbach’s α reliability coefficients were estimated to assess the reliability of scales representing C-Change dimensions of the culture.27 34 Data manipulations and statistical analyses were conducted in Excel and R. Qualitative responses to open-ended questions were coded and analysed thematically using the process of constant comparison. Themes, subthemes and illustrative quotations along with a description of qualitative methods and procedures are given in online supplemental table S2.
Results
Women in academic rheumatology
Table 1 summarises responses from the survey of EULAR scientific member society leaders on the representation of women in academic rheumatology. In total, 12 of 45 EULAR scientific member society leaders completed the survey (response rate=27%) and we received two additional responses from the Group of Women in Rheumatology, Spain, and Female Advancement In Rheumatology (FAIR) Task Force, Austria.
Estimated percentage of women in academic rheumatology by country, data from national society leaders based on various sources, 2020 or the latest available year
Survey responses highlight a lack of gender-disaggregated national statistics on the academic rheumatology workforce in many countries. Much of the reported data is based on the national society membership data and personal estimates by national society leaders, the reliability of which may be limited. Direct comparison of the academic rheumatology workforce by country is also problematic because definitions of medical specialties, academic practices and the status of rheumatology among other medical specialties vary across countries.
Notwithstanding these limitations, it appears that in many countries women represent 50% or more of all qualified rheumatologists, but there are disproportionately fewer women in academic rheumatology than in clinical rheumatology. While the majority of early career academic rheumatologists are female, women remain significantly under-represented in senior academic roles.
Respondent profile of the EULAR and EMEUNET membership sample
In total, 649 potential participants accessed the survey of EULAR and EMEUNET members, 324 (completion rate=50%) provided complete responses. Based on the EMEUNET membership, which is open to rheumatologists and researchers who are less than 40 years old (n=2404 at the time of the survey completion) and the number of responses in this age category (210), the estimated survey response rate among EMEUNET members was 9%. The respondents represented 23 of 45 EULAR scientific member society countries (51%), as well as Mexico and the USA (online supplemental figure S1). Given that the EMEUNET membership overlaps with the membership of EULAR scientific member societies and the total membership of EULAR scientific member societies was unknown, we were unable to estimate a survey response rate among the total membership of EULAR scientific member societies.
The majority of the respondents were women (71%) and aged 40 years or below (65%) (online supplemental table S3). The socio-demographic profile of the respondents also highlights substantial proportions of the respondents who identified themselves as an ethnic minority (10%) and as lesbian/gay/bisexual/transgender/queer (7%); one respondent identified themselves as third gender (online supplemental table S3).
The respondents represented varied career paths (online supplemental table S4). By profession, the respondents were predominantly rheumatologists (87%) with a representation of health professionals (6%) and non-clinical scientists (7%). The majority of the respondents regardless of gender had a permanent contract of employment. A slightly higher proportion of male respondents than female respondents (37% vs 31%) reported a leadership role, but this difference was not significant (p=0.20). Female respondents reported working less than full time significantly more frequently than male respondents (21% vs 10%, p=0.02). In total, 46% of the respondents reported having an academic role and a further 29% of the respondents were considering pursuing an academic career. However, 33% of the respondents were considering minimising or leaving their academic role (online supplemental table S4).
Academic workload
There were no significant gender differences in the share of time spent by academic rheumatologists on clinical care, research, teaching, administration and other activities in a typical week (figure 1).
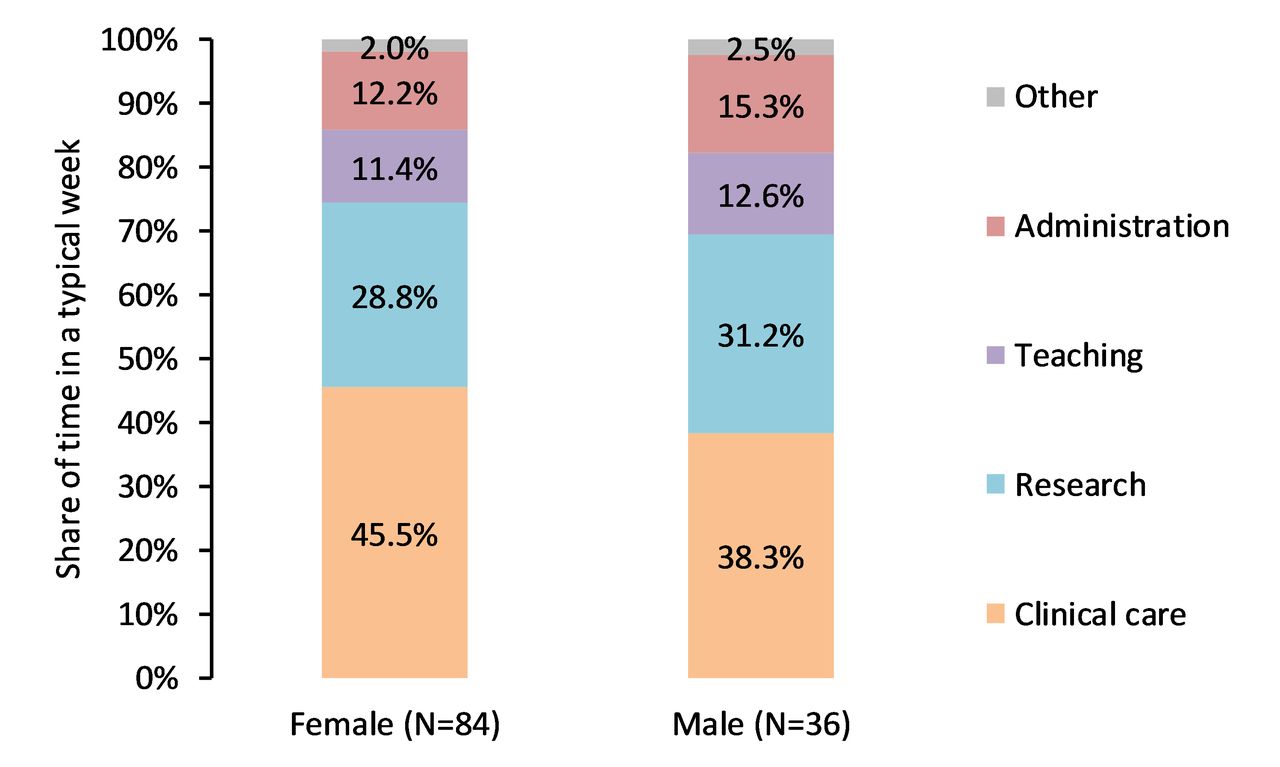
Share of time spent by academic rheumatologists on different activities in a typical week by gender, EULAR and EMEUNET members, 120 responses. The respondents were asked to distribute 100 points representing their working hours during a typical week across different activities. EMEUNET, Emerging EULAR Network.
A comparison of typical self-reported working hours in a week by role shows that respondents in academic roles (women and men combined) work longer hours than respondents in non-academic roles (p=0.02) (figure 2). A cross-country comparison of France, Italy and UK, which had the largest number of respondents in both academic and non-academic roles, showed that in each of these countries respondents in academic roles worked longer hours and that cross-country differences were not statistically significant (p=0.95). While there were no statistically significant gender differences in typical working hours in non-academic rheumatology (p=0.65), male respondents in academic roles appear to work on average 4.5 hours/week longer than their female counterparts (p=0.03).
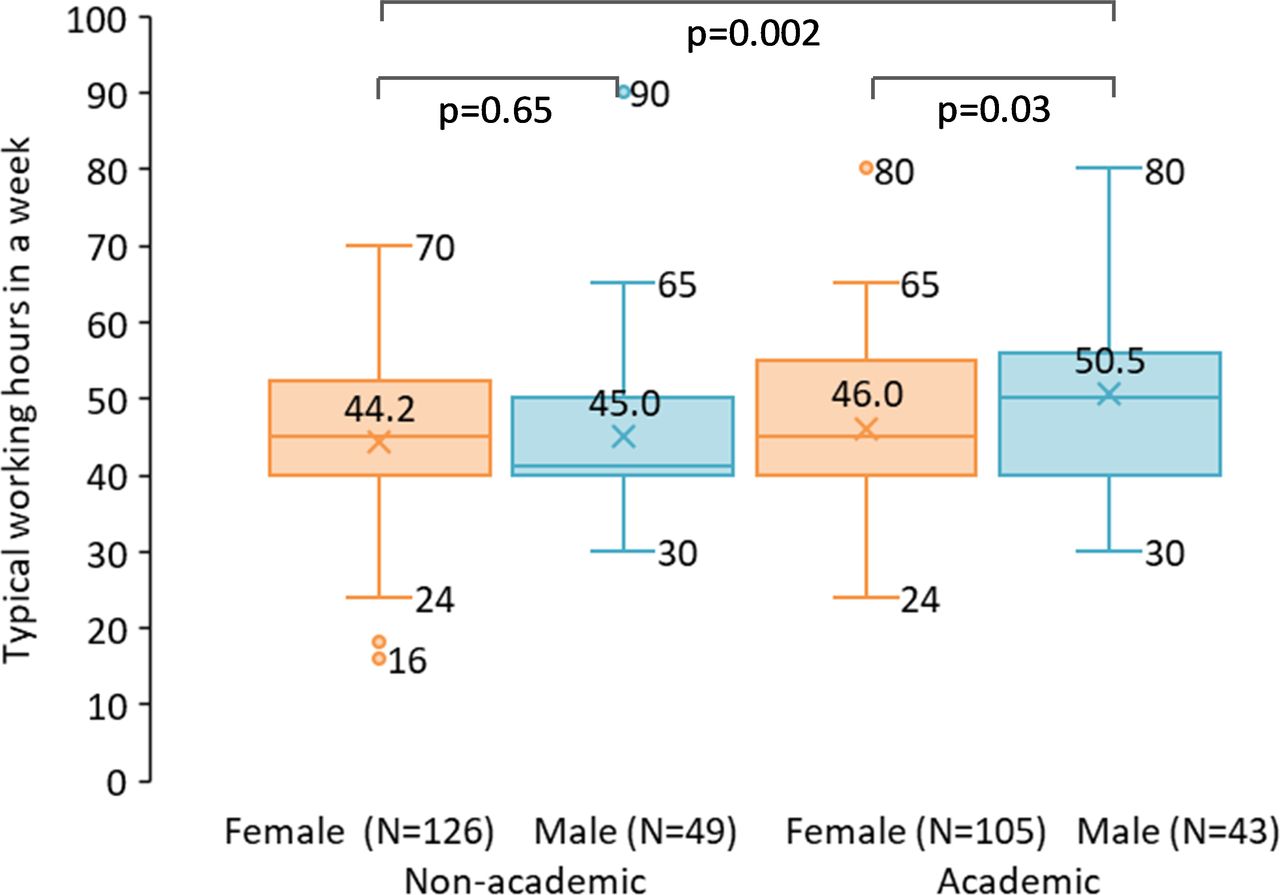
Typical self-reported working hours in a week by role and gender, EULAR and EMEUNET members, 323 responses. The box and whisker chart shows distribution of data into quartiles: the top of the boxes indicates the upper quartile, the bottom of the boxes indicates the lower quartile, the lines extending vertically indicate variability outside the upper and lower quartiles, the dots outside those lines indicate outliers, the Xs inside the boxes indicate the mean values and the horizontal lines inside the boxes indicate the median values. EMEUNET, Emerging EULAR Network.
Gender discrimination and sexual harassment
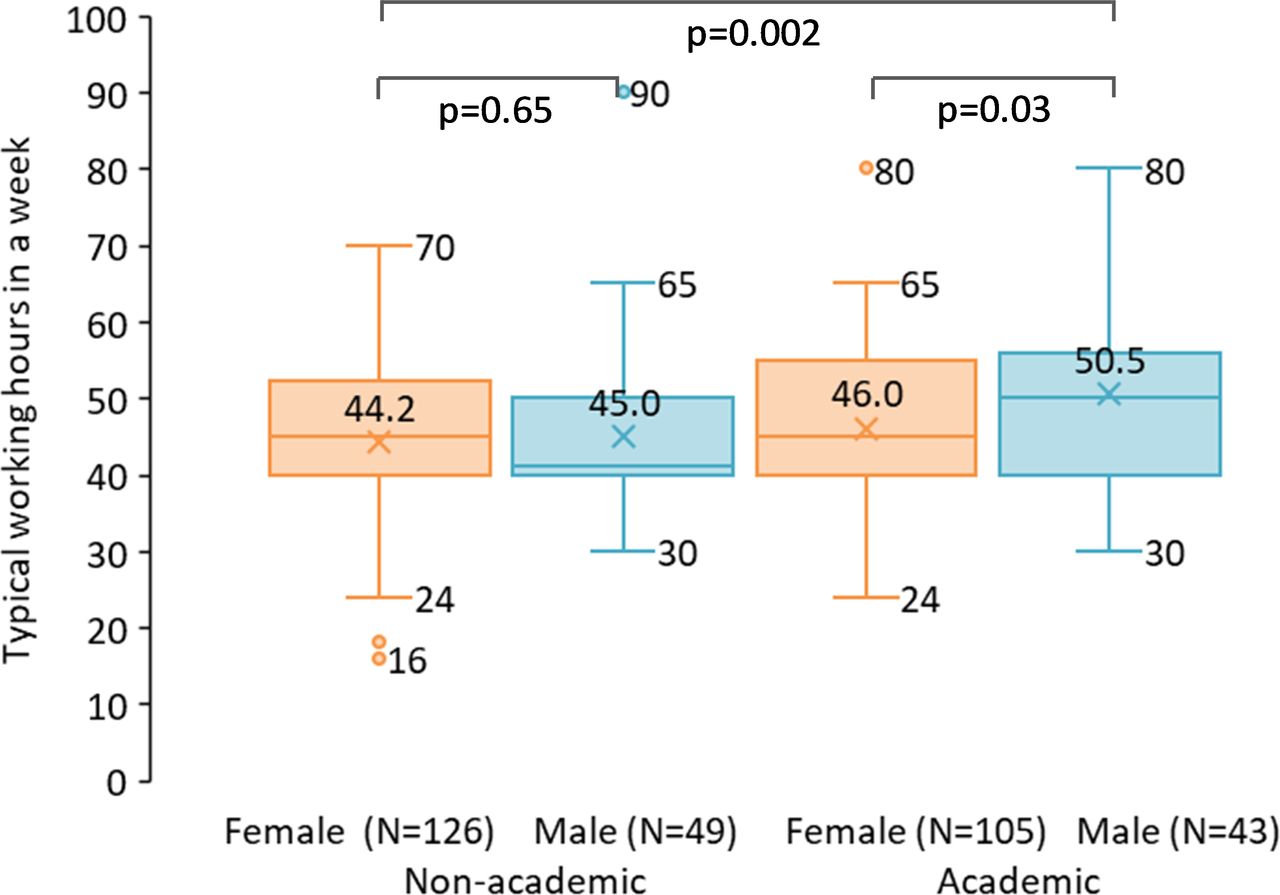
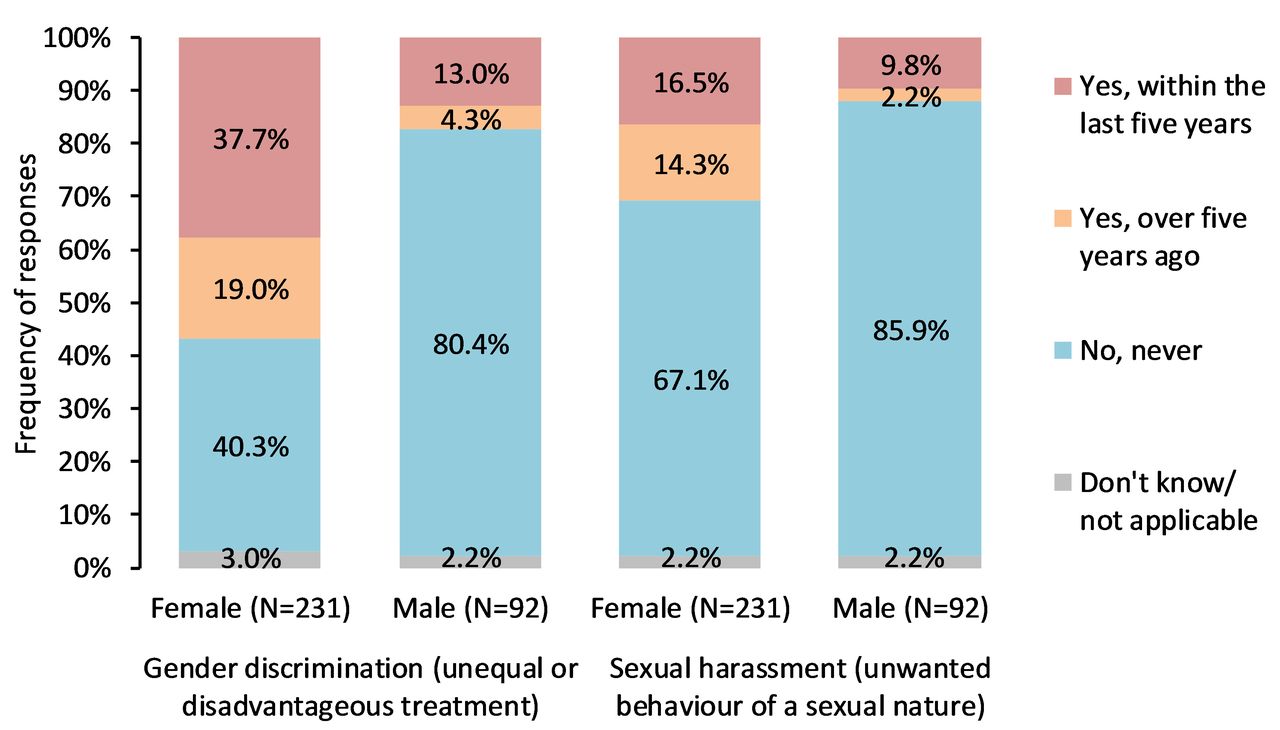
Women significantly more frequently than men reported having experienced gender discrimination, that is, unequal or disadvantageous treatment, in their professional careers both in the last 5 years (38% vs 13%, p<0.05) and over 5 years ago (19% vs 4%, p<0.05) (figure 3). While women significantly more frequently than men reported having experienced sexual harassment, that is, unwanted behaviour of a sexual nature, in their professional careers over 5 years ago (14% vs 2%, p<0.05), there was no gender difference in the last 5 years (17% vs 10%, p=0.3). One respondent, who identified themselves as third gender, reported experiences of both gender discrimination and sexual harassment.

Frequencies of responses to the question ‘Please tell us if you have personally experienced in your professional career any gender discrimination or sexual harassment’ by gender, EULAR and EMEUNET members, 323 responses. EMEUNET, Emerging EULAR Network.
Institutional culture
Table 2 summarises estimated characteristics of dimensions of the institutional culture in rheumatology, measured using validated psychometric scales from the C-Change Faculty Survey.27 A higher mean score reflects perceptions of a more positive culture. Importantly, the survey results indicate no statistically significant gender differences in leadership aspirations, self-efficacy in career advancement and work–life integration. Yet, female respondents perceived significantly lower levels of gender equity in their institutions than male respondents. In the context of this exploratory survey, Cronbach’s α reliability coefficients indicate sufficient levels of reliability for all dimensions of the institutional culture, with higher reliability for gender equity and self-efficacy in career advancement, and lower reliability for leadership aspirations.
Definitions and estimated statistical characteristics of C-Change scales representing dimensions of the culture, EULAR and EMEUNET members, 324 responses*
Factors impacting career advancement
Figure 4 summarises means and gender differences for factors impacting career advancement. The responses indicate that 7 of 26 societal, professional, institutional and personal factors have a disproportionate impact on women’s and men’s career advancement.

Means and statistically significant gender differences (p<0.001) for responses to the question ‘Please indicate what impact, if any, the following factors have on your career advancement’ on a 5-point scale from ‘strongly negative’ (−2) to ‘strongly positive’ (2), EULAR and EMEUNET members, 323 responses. The colour gradient represents the range of values: red marks the minimum, yellow the middle and green the maximum values. EMEUNET, Emerging EULAR Network.
In stark contrast with male respondents, female respondents perceived a negative impact of societal factors on their career advancement. There were significant gender differences in the perception of the impact of societal gender norms and expectations as well as maternity/paternity leave. While female respondents perceived a negative impact of gendered norms and behaviours in rheumatology as well as gender balance in professional associations, male respondents perceived a positive impact. Both female and male respondents perceived a positive impact of the visibility of suitable role models in rheumatology. However, a significant gender difference in the magnitude of perceptions implies a lower visibility of suitable role models for female respondents.
The most salient institutional factors regardless of gender concerned the positive impact of support from supervisors/colleagues and mentors/sponsors as well as the negative impact of long working hours. Of note, women reported a neutral and men a small positive impact of part-time working opportunities on their career advancement. The most salient personal factors concerned the negative impact of caring responsibilities and the positive impact of support from family/friends, partner’s role, as well as career planning and leadership skills.
Interventions to aid career advancement
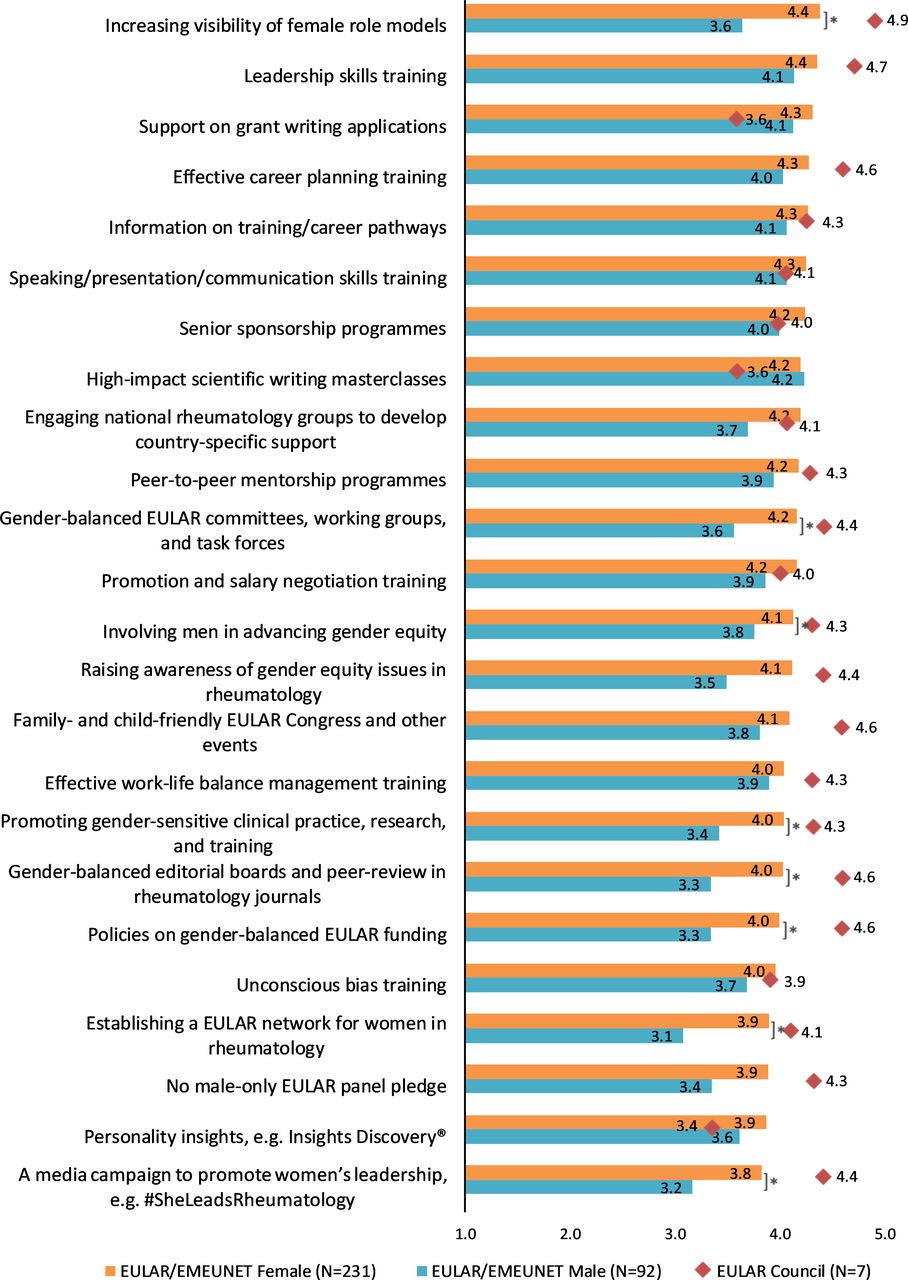
Figure 5 summarises means and gender differences (p<0.001) for the perceived utility of potential interventions to aid career advancement. While 8 of 24 potential interventions showed a significantly higher ranking by female respondents, the majority of these potential interventions did not differ in their perceived utility by gender. The highest-ranked interventions for career advancement regardless of gender included: leadership skills training, support on grant writing applications, effective career planning training, information on training/career pathways, speaking/presentation/communication skills training, senior sponsorship programmes and high-impact scientific writing master classes.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Means and statistically significant gender differences (p<0.001) for responses to the question ‘Please indicate how strongly you agree or disagree that the following interventions would be helpful for your career advancement’ on a 5-point scale from ‘strongly disagree’ (=1) to ‘strongly agree’ (=5) by EULAR and EMEUNET members, 323 responses. *Statistically significant gender differences (p<0.001). ♦Means for responses to the question: ‘Please indicate how strongly you agree or disagree that the following interventions would be helpful for EULAR members’ by EULAR Council members, 7 responses. EMEUNET, Emerging EULAR Network.
Figure 5 also provides means for the perceived utility of potential interventions for career advancement from the survey of EULAR Council members. In total, 7 of 30 EULAR Council members completed the survey (response rate=23%). The majority of the respondents were male (71%) and over 55 years of age (71%). Compared with the responses from EULAR and EMEUNET members, responses from EULAR Council members indicate a higher perceived utility for the majority of the proposed interventions. The highest-ranked interventions concerned increasing the visibility of female role models, leadership skills training, effective career planning training, family-friendly and child-friendly EULAR Congress and other events, policies on gender-balanced EULAR funding and gender-balanced editorial boards and peer-review in rheumatology journals.
Discussion
Despite evidence that gender equity can contribute to social progress, quality of science and academic workforce sustainability, women remain under-represented in academic medicine: this is particularly so in leadership roles. This cross-sectional study has gathered and analysed empirical evidence on the extent of the unmet need for support of female rheumatologists, health professionals and non-clinical scientists in academic rheumatology with a view to informing a framework to address this through EULAR. The study included three web-based surveys of (1) EULAR scientific member society leaders, (2) EULAR and EMEUNET members and (3) EULAR Council members. Although we could not determine to what extent the survey results are representative of the study populations, the survey results provide several important findings for discussion.
First, in many countries, there are disproportionately fewer women in academic rheumatology than in clinical rheumatology, and women in academic rheumatology tend to be under-represented in senior academic roles. However, similar to the previous reports by the European Musculoskeletal Conditions Surveillance and Information Network35 and by the EULAR task force on the conduction of workforce requirement studies in rheumatology,36 our study highlights challenges in obtaining and monitoring standardised workforce data in Europe. Specifically, much of our data is based on the national society membership and personal estimates by national society leaders as currently there is a lack of gender-disaggregated national statistics on the academic rheumatology workforce in many countries.
Second, we found that in a typical week both women and men in academic roles work longer hours than respondents in non-academic roles, but there are no significant gender differences in the share of time spent on clinical care, research, teaching, administration and other activities. While there are no statistically significant gender differences in typical self-reported working hours in non-academic rheumatology, male respondents in academic roles appear to work on average 4.5 hours/week longer than their female counterparts. These findings have important implications for the sustainability of the academic rheumatology workforce as previous research showed that role strain is positively associated with intent to leave academic medicine for both genders and perceived work–family conflict is negatively associated with leadership-seeking for women.21 37 38
Third, respondents of all genders reported having experienced instances of perceived gender discrimination and sexual harassment in their professional careers, but women did so more frequently than men. A survey conducted in early 2021 with support from the German Society of Rheumatology reported similar findings among German rheumatology physicians and residents.39 These findings are consistent with previous research from other fields of academic medicine demonstrating that women had more difficulties in being taken seriously than men,40 women were more likely to be excluded from the dominant institutional culture,41 and that sexism was one of the most common disadvantages to an academic career.42 Previous research also demonstrated that gender equity interventions could cause resentment among men about perceived positive discrimination of women.43 Previous research also linked gender discrimination and sexual harassment.25 26 A recent multi-institutional longitudinal study in US medical schools argued that women seeking career advancement were more vulnerable to sexual harassment due to greater exposure to potential abuses of authority, but showed resilience and succeeded nonetheless.44 Monitoring and addressing sexual harassment is required to ensure that those who seek career advancement do not risk exposure to sexual harassment rather than become expect to develop resilience to it.
Fourth, using previously validated psychometric scales, we obtained valid and reliable measures of institutional culture in rheumatology. While female respondents reported lower levels of gender equity in their institutions than male respondents, we found no gender differences in the respondents’ perceptions of their leadership aspirations, self-efficacy in career advancement and work–life integration. They are novel in the context of rheumatology but similar to the previous research into institutional culture in US medical schools.22 These findings suggest that women and men equally aspire to become leaders in rheumatology, but institutional culture makes it harder for women than men to realise their leadership aspirations. There is a greater need to improve institutional culture with regard to gender equity for women, but women and men are likely to benefit equally from interventions aimed at supporting leadership aspirations, career advancement skills and work–life integration.
Fifth, we found that 7 of 26 societal, professional, institutional and personal factors have disproportionate impact on women’s and men’s career advancement, but professional associations have a limited potential for intervention to address some of the most salient factors. Yet, there might be a potential for EULAR to raise awareness about the negative impact of societal factors on women’s career advancement. In contrast, there is a clear potential for EULAR to influence many of the salient professional factors, such as gendered norms and behaviours in rheumatology, gender balance in professional associations and the visibility of suitable role models in rheumatology, both on their own and with support from national professional societies and associations. Similar to the EMEUNET postdoctoral mentoring programme,45 EULAR could potentially offer mentoring and sponsorship programmes to complement institutional ones. There is a clear potential to influence some of the factors related to personal skills and capabilities by offering training on promotion and salary negotiation skills, career planning skills, self-confidence and leadership skills.
Finally, we found gender differences in the perceived utility of interventions focusing on women as expected beneficiaries and no statistically significant gender differences in the perceived utility of interventions with both women and men as expected beneficiaries. Skills-based training interventions were ranked highly by both men and women, whereas increasing the visibility of female role models was the highest-ranked intervention by female respondents and by EULAR Council members.
Our study has several noteworthy limitations. One, we could not determine whether the survey results are statistically representative of the study populations. We obtained data on the academic rheumatology workforce from 13 EULAR member countries, which may not be representative of all 45 EULAR member countries. Reliability of personal estimates by national society leaders and national society membership data may be limited. Due to variations in national practices, direct comparison of the academic rheumatology workforce by country and career stage is problematic. Future research is likely to yield more comprehensive and reliable results when gender-disaggregated national statistics and national society data on the academic rheumatology workforce across all EULAR countries becomes available. Another, we could not control for selection bias in the EULAR and EMEUNET members sample because we could not obtain data on the membership of EULAR national societies and EMEUNET disaggregated by gender and key socio-demographic and career characteristics. An estimated 9% response rate among EMEUNET members suggests potential for significant non-response bias due to the survey procedures and topic. Namely, the survey was distributed by the EULAR Office and EMEUNET as part of their multiple communications and news updates via email, websites and social media for 10 weeks. Using other procedures, such as personalised mailouts and reminders, financial incentives, postal and telephone strategies and a shorter questionnaire could have increased the response rate.46 Due to the lack of data on non-respondents, we cannot ascertain whether selection bias is a concern for the sample. We do not rule out that those who had higher aspirations for an academic career or those who experienced gender inequalities were more likely to reply. An estimated 9% response rate may also indicate that the majority of potential respondents did not perceive gender equity as a problem for their career advancement. Generalisability of the results to specific national contexts may be further limited due to variation in national practices. Future research is likely to yield more statistically representative results by sampling survey participants based on national society membership and taking into account specific national contexts. Yet another, a 23% response rate for the EULAR Council members survey does not rule out a possibility of non-response bias. A higher response rate in future research is likely to yield more statistically representative results. Overall, future research could usefully test our findings in representative samples taking into account specific national contexts.
In conclusion, this study provides important empirical evidence on gender differences in career advancement in academic rheumatology and explores potential interventions to aid gender-equitable career advancement in academic rheumatology across Europe. However, the findings may not be fully generalisable to the entire study populations and specific national contexts. This study has informed an EULAR task force developing a framework to accelerate gender-equitable career advancement of rheumatologists, health professionals and non-clinical scientists in academic rheumatology through EULAR.
Ethics statements
Patient consent for publication
Ethics approval
This study was considered by the University of Oxford's Clinical Trials and Research Governance team and exempted from full ethics review. The outcome was communicated via email without a reference number or ID. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We thank Patrizia Jud from the EULAR Office and the EMEUNET, Concha Delgado Beltrán from the Group of Women in Rheumatology, Spain, and Christina Duftner from the Female Advancement In Rheumatology Task Force, Austria, for their help with data collection. Preliminary results from this study were presented at the 2020 EULAR Congress.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @lauraandreoli80, @CarolineOspelt, @ElenaNikiUK, @drlauracoates
Contributors All authors have contributed to this work and approved the final version. LCC acts as guarantor.
Funding This study was funded by the EULAR (project number: EPI 024). LCC is supported by the National Institute for Health Research (NIHR) Oxford Biomedical Research Centre. PVO is supported by the NIHR Oxford Biomedical Research Centre and the European Union’s Horizon 2020 research and innovation programme (grant agreement number: 872396). HS and A-MK are supported by the NIHR Leeds Biomedical Research Centre. The views expressed are those of the authors and not necessarily those of the UK National Health Service, the NIHR or the UK Department of Health and Social Care.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.