Article Text

Abstract
SARS-CoV-2 has been recognised as a potential trigger of inflammatory arthritis in individuals with inflammatory rheumatic diseases as well as in previously unaffected individuals. However, new-onset arthritis after COVID-19 is a heterogeneous phenomenon that complicates differential diagnosis. For example, acute arthritis with features of viral arthritis has been reported after COVID-19, as has crystal-induced arthritis. Arthritides mimicking reactive arthritis (ReA) have also been described, but these patients often do not fulfil the typical features of ReA: several reports describe cases of patients older than 45 years at the onset of arthritis, and the characteristic genetic feature of ReA, HLA-B27, is rarely found. Because viral infections are much less likely to cause ReA than bacterial infections, and respiratory infections are rarely the cause of ReA, it is currently unknown whether SARS-CoV-2 can cause true ReA. Here, we report the case of a 30-year-old patient who presented with acute pain, swelling and redness in the left metatarsophalangeal (MTP) joint and ankle 7 days after resolution of a SARS-CoV-2 infection. Diagnostics revealed arthritis of the MTP2, synovitis of the upper ankle with significant joint effusion and peritendinitis of the flexor tendons. Based on the clinical manifestations and diagnostic test results, ReA appeared to be the most likely cause. A screening for typical ReA-associated infections was negative. The patient was treated with NSAIDs and intra-articular and systemic glucocorticoids. At a follow-up visit after discontinuation of glucocorticoids, the patient was symptom-free. Overall, we observed a ReA with typical clinical, genetic and patient characteristics after SARS-CoV-2 infection, and we conclude that a direct association with COVID-19 is highly plausible.
- arthritis, reactive
- COVID-19
- arthritis
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPICS
ARS-CoV-2 can cause inflammatory arthritis in individuals who have inflammatory rheumatic disease, but also in individuals who do not have the disease previously.
New-onset arthritis following COVID-19 is a heterogeneous phenomenon.
WHAT THIS STUDY ADDS
SARS-CoV-2 is likely capable of causing reactive arthritis.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Physicians should consider reactive arthritis as a possible differential diagnosis.
Introduction
COVID-19 is caused by infection with SARS-CoV-2. COVID-19 is associated with a range of symptoms including fever, loss of sense of smell and taste, gastrointestinal symptoms, thromboembolic complications, cardiomyopathy, pneumonia, and renal failure.1 Early on, musculoskeletal symptoms such as arthralgia and myalgia were reported in association with SARS-CoV-2 infection.1 2 Recently, SARS-CoV-2 has also been recognised as a precipitating cause of inflammatory arthritis in individuals known to have an inflammatory rheumatic disease, as well as in previously unaffected individuals. However, new-onset arthritis after COVID-19 is a heterogeneous phenomenon that complicates differential diagnosis. For example, acute arthritis with features of viral arthritis3 4 and crystal-induced arthritis5 have been reported after COVID-19. Arthritides mimicking reactive arthritis (ReA)6–11 have also been described, but the affected patients often do not conform to the typical ReA patient pattern: several reports describe cases of patients older than 45 years at onset, and the characteristic genetic feature of ReA, HLA-B27, has rarely been found. In addition, viral infections are much less likely to trigger ReA than bacterial infections, and respiratory tract infections are also much less likely to cause ReA than gastrointestinal and genitourinary mucosal infections. Therefore, it is currently unknown whether SARS-CoV-2 can cause true ReA. Here, we present a typical case of ReA following a rather mild course of COVID-19.
Case report
In May 2021, an otherwise healthy 30-year-old female patient presented with acute pain, swelling and redness in the second left metatarsophalangeal (MTP) joint and left ankle. Sixteen days before the onset of these symptoms, she tested positive for SARS-CoV-2 by PCR testing. She had subfebrile temperatures, cold symptoms, and loss of olfactory and gustatory function. The patient was self-isolated, and hospitalisation was not required. The patient also reported swollen, irritated and red eyes with no history of eye infections. COVID-19 symptoms resolved after ten days, and a nasopharyngeal swab tested negative for SARS-CoV-2, indicating that the infection had resolved and the virus had been cleared.
Physical examination revealed swelling, redness and pain in the left ankle and forefoot. The patient had no history of psoriasis or inflammatory bowel disease (IBD). Other than the pain in the right foot, there were no other complaints. The patient had no history of trauma to the foot or strenuous exercise. She had no history of joint, back or muscle pain. Deep vein thrombosis was ruled out by duplex sonography. No osseous lesions were found in radiographic imaging (figure 1).
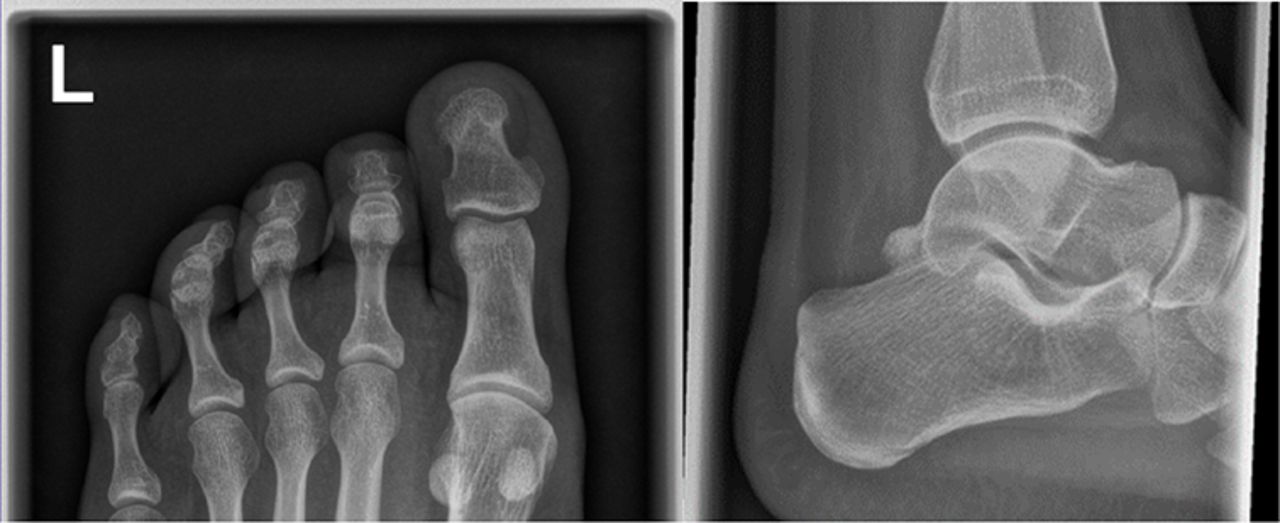
Radiograph of the patient’s left foot showing no bony lesions.
Laboratory examination revealed elevated humoral inflammatory parameters (C-reactive protein (CRP): 1,6 mg/dL, erythrocyte sedimentation rate (ESR): 79 mm/hour). Rheumatoid factor and antibodies to cyclic citrullinated peptides were not detectable. The ANA-titre was negative. The patient was HLA-B27 positive. Serological screening for acute respiratory and gastrointestinal tract infections (including IgG and IgM antibodies to Chlamydia pneumoniae, Chlamydia trachomatis, Mycoplasma pneumoniae, Yersinia enterocolitica and Campylobacter jejuni) was negative; IgM and IgG antibodies to Borrelia spp were also not detected.
An ultrasound examination of the left foot was performed, which revealed synovitis of the upper ankle and synovitis of MTP 2 with significant joint effusion and increased power doppler signal (figure 2), as well as peritendinitis of the posterior tibialis muscle and digitorum longus muscle, flexor hallucis muscle, and peronei longus and brevis muscles.

{kind=link}
{kind=link}
Ultrasound images of the left MTP 2 joint as well as the left ankle showing joint effusion and increased power doppler signal. MTP, metatarsophalangeal.
After a diagnostic joint aspiration, the synovial fluid analysis revealed a cell count of 0.3×103 leucocytes per µL and no crystals.
The patient was initially treated with non-steroidal anti-inflammatory drugs (NSAIDs), and because symptoms did not improve, she received 30 mg/die of prednisolone. Treatment resulted in a partial response, but symptoms in the MTP2 joint persisted. Diagnostic and therapeutic arthrocentesis of the left MTP 2 joint was performed. Although no joint fluid was obtained, an injection of 12 mg triamcinolone actetonide resulted in significant clinical improvement. At a follow-up visit after discontinuation of corticosteroids, the patient was completely symptom-free. On analysis of blood tests, CRP and ESR were within the normal range.
Discussion
The patient presented 7 days after resolution of SARS-CoV-2 infection with typical, although mild, symptoms of COVID-19 with severe swelling and pain in the left ankle joint and forefoot. Based on the overall picture, ReA appears to be the most likely cause of the patient’s symptoms. The most common differential diagnoses for oligoarthritis are ReA, spondyloarthritis, psoriatic arthritis, sarcoidosis, Lyme arthritis, gouty arthritis and arthritis associated with IBD, as well as soft connective tissue disease or vasculitis. No symptoms suggestive of pathologies other than ReA—such as lymphadenopathy, back pain, skin lesions, a history of tick bites or Borrelia antibodies, IBD, psoriasis or symptoms consistent with soft connective tissue disease or vasculitis—were found on history, clinical presentation and comprehensive diagnostic examination.
ReA is a sterile joint inflammation complicating an extra-articular infection. There are no universally accepted diagnostic criteria, and the diagnosis is based mainly on clinical aspects such as oligoarthritis of the lower limbs that develops within 1–6 weeks of the previous infection, especially in young, HLA-B27-positive individuals. The suspected diagnosis of ReA was supported by the typical case constellation: the patient was young, HLA-B27-positive, had asymmetric oligoarthritis involving the lower extremity, the synovial fluid was sterile and symptoms began several days after resolution of infection. Complete response to NSAIDs and glucocorticoids was also consistent with typical features for ReA. The HLA-B27 allele is the genetic hallmark of SpA, including ReA; the phenotype is found in 50%–80% of cases with ReA,12 however, in many of the reports describing arthritis following infection with SARS-CoV2 published to date, patients were HLA-B27 negative or were not tested for HLA-B27. The mechanism by which HLA-B27 contributes to ReA is not yet fully understood. However, HLA-B27 correlates with more severe and prolonged arthritis and sacroiliitis and a higher incidence of extra-articular manifestations. Screening our patient for underlying respiratory and gastrointestinal coinfections, common in ReA, was negative, leading us to assume an association with SARS-CoV-2 infection.
However, there is no formal evidence of a causal relationship with COVID-19, as the arthritis in our patient may have been caused by a subclinical infection that was not detected during the comprehensive diagnostic workup. A limitation in this case is that although a comprehensive diagnostic workup was initiated, urinalysis was not performed for genitourinary tract infections, which are commonly associated with ReA. In at least 25% of patients with ReA, the previous infection is asymptomatic.13 It is also possible that the pathogen of a possible subclinical coinfection could no longer be detected at the time of serological diagnosis.
On the other hand, viral arthritides have been described after COVID-19.3 4 Viral arthritis is frequently described in association with acute infection with parvoviruses, hepatitis B, hepatitis C, HIV and alphaviruses.14 In our patient, viral arthritis cannot be completely excluded. Nevertheless, the features of viral arthritis are typically different from the manifestation of ReA, as viral arthritis presents as acute polyarthritis in combination with other symptoms such as fever, rash or lymphadenopathy, mimicking rheumatoid arthritis, and is usually self-limiting.14 All of these features were not present in our patient. Therefore, testing for SARS-CoV-2 in the aspirated synovial fluid was not performed because a positive finding was considered highly unlikely.
The pathogenesis of ReA is only partially understood, and many proposed mechanisms are still under debate.15 16 In well-studied pathogens such as C. trachomatis, it is known that the vital organism is transported to the joint in infected monocytes/macrophages and settles in the synovial tissue, leading to infection of the synovium.17 Other pathogens do not reach the joint in a vital and intact state, but in parts—including so-called ‘arthritogenic peptides’.15 18 A local inflammatory reaction is then triggered in the synovium. Common hypotheses suggest that the inflammation is caused either by direct cross-reactivity of HLA-B27 with these arthritogenic antigens or, at least in part, by molecular mimicry.15 18 Although molecular mimicry has been shown to trigger autoimmunity and has been discussed in acute SARS-CoV-2 infection as well as in the postinfectious immunological phenomena reported to date,19 20 molecular mimicry between SARS-CoV-2 and HLA-B27 has not yet been demonstrated or described.
The causal relationship between SARS-CoV-2 infection and new-onset arthritis has not been proven, and further studies are needed to understand the immunopathogenic mechanisms. However, as more cases are reported and clinical manifestations are heterogeneous, physicians should be sensitive to this phenomenon. Overall, we believe it is likely that SARS-CoV-2 infection can cause ReA.
Ethics statements
Patient consent for publication
References
Footnotes
Contributors All authors contributed drafting of this manuscript.
Funding This work was supported by the Verbundantrag 'COVIM' (project AP8, 01KX2021) by the Federal Ministry of Education and Research of Germany; and by the FöFoLe program of the medical faculty of the LMU Munich.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.