Article Text

Abstract
Aims In May 2020, a nationwide, web-based system for remote entry of patient-reported outcomes (PROs) in inflammatory rheumatic diseases was launched and implemented in routine care (DANBIO-from-home). After 1.5 years of use, we explored clinical characteristics of patients who did versus did not use the system, and the time to first entry of PROs.
Methods All patients followed in DANBIO were informed about DANBIO-from-home by electronic invitations or when attending their clinic. Characteristics of patients who did/did not use DANBIO-from-home in the period after implementation were explored by multivariable logistic regression analyses including demographic and clinical variables (gender, age group, diagnosis, disease duration, use of biological disease-modifying agent (bDMARD), Health Assessment Questionnaire (HAQ), Patient Acceptable Symptom Scale (PASS)). Time from launch to first entry was presented as cumulative incidence curves by age group (<40/40–60/61–80/>80 years).
Results Of 33 776 patients, 68% entered PROs using DANBIO-from-home at least once. Median (IQR) time to first entry was 27 (11–152) days. Factors associated with data entry in multivariate analyses (OR (95% CI)) were: female gender (1.19 (1.12 to 1.27)), bDMARD treatment (1.41 (1.33 to 1.50)), age 40–60 years (1.79 (1.63 to 1.97)), 61–80 years (1.87 (1.70 to 2.07), or age >80 years (0.57 (0.50 to 0.65)) (reference: age <40 years), lower HAQ (0.68 (0.65 to 0.71)) and PASS ‘no’ (1.09 (1.02 to 1.17). Diagnosis was not associated. Time to first entry of PROs was longest in patients <40 years of age (119 (24–184) days) and shortest in the 61–80 years age group (25 (8–139) days).
Conclusion A nationwide online platform for PRO in rheumatology achieved widespread use. Higher age, male gender, conventional treatment and disability were associated with no use.
- Patient Reported Outcome Measures
- Epidemiology
- Health services research
Data availability statement
All data relevant to the study are included in the article or uploaded as supplemental information. Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Patient-reported outcomes (PROs) are widely used to monitor inflammatory rheumatic diseases (IRDs).
We lack knowledge regarding the implementation of online systems for monitoring of PROs in IRD routine care including the time to first entry and characteristics of the patients who use or do not use the system.
WHAT THIS STUDY ADDS
A web-based system for remote entry of PROs was launched during the COVID-19 pandemic, and after 1.5 years, nearly 70% of 33 776 patients had used the system.
Use was high in all patient groups, and median time to first entry was 27 days.
Women and patients treated with a biological disease-modifying antirheumatic drug used the system most, and use was lowest in the young and elderly.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
From-home systems for capturing PROs can be successfully implemented in routine care to support monitoring of patients.
Background
The benefits of using patient-reported outcomes (PROs) for monitoring of health status in chronic diseases, including inflammatory rheumatic diseases (IRDs), are well established.1–6 In the debate on how to optimally manage patients with chronic diseases in routine care,7 8 digital solutions for online monitoring of diseases constitute a more recent solution.9–14 Recent 2022 EULAR points to consider for remote care in rheumatology highlighted that knowledge about drivers and barriers to telehealth is essential to facilitate remote care approaches in clinical practice.15 Importantly, not all patients have access, skills or interest in using remote digital solutions.16 Although previous studies (mainly explorative or outside rheumatology) have demonstrated feasibility of electronic systems for online data entry of PROs,17–24 no studies have to our knowledge explored use following large-scale routine care implementation of a nationwide online system in IRD.
In Denmark, patients with IRD treated in routine care are monitored prospectively in the nationwide DANBIO registry.25 For nearly 20 years, PROs have been entered by touch screens in the waiting areas of the rheumatology clinics.25 26 The validity of remote entry of PROs had been assessed and compared with touch screen reporting.27 Motivated by the SARS-CoV-19 pandemic, an online website for secure entry of PROs was launched and implemented for use in clinical practice in the spring of 2020 (DANBIO-from-home).28
With this study, we aimed to explore the use in routine care of DANBIO-from-home for entry of PROs during the first 1.5 years after launch, with focus on (a) the characteristics of patients who did versus who did not use the system, and (b) the impact of patient characteristics on time to first entry of PROs. We hypothesised that clinical factors such as age could affect the use and delay time to first entry.
Methods
DANBIO-from-home was launched on 15 May 2020 and allowed patients to enter PROs remotely by computer, tablet or smartphone after secure log-on to the website (https://danbio.dk).28 The launch took place 2 months into the SARS-CoV-19 pandemic. The information technology (IT) solution ensured that PROs entered by the online system were fully integrated with data already available in DANBIO. Patients were informed about DANBIO-from-home when they attended their rheumatology clinic, but also by invitations sent through e-Boks. e-Boks is a public Danish infrastructure for electronic communication available to 80%–90% of Danish citizens. Use of e-Boks is mandatory to all Danish citizens, and exemption can only be given to citizens with poor digital skills, lack of access to computer, language limitations, poor physical/cognitive health or similar.29 In the current study, e-Boks invitations were sent to patients ≥18 years old, with >1 registered DANBIO contact (visit in hospital or rheumatology specialists in primary care) after 11 May 2019, alive and with ongoing contact to a rheumatology clinic.
Patients could enter their PROs by DANBIO-from-home at any time point. However, they were encouraged to access before planned rheumatology consultations (by phone, video or physical). Furthermore, PROs were entered as part of the voluntary survey ‘You and your rheumatic disease during times with coronavirus’, which was conducted on three occasions in fixed time intervals and independently of routine care appointments: May 2020, November 2020 and June 2021.28 30 ,31 In relation to each of the three surveys, patients were informed in e-Boks about DANBIO-from-home (twice per survey: invitation and friendly reminder to non-respondents, patients who declined to participate in the survey received no additional information). Thus, survey participation occurred largely independently of routine care appointments.
During the pandemic, the options for providing patient information in physical format (pamphlets, etc) were limited, and patient education and information only occurred through the website (https://danbio.dk), in the e-Boks electronic letters or in relation to routine care consultations. The PROs entered by DANBIO-from-home were identical to those previously entered by touch screens in the waiting areas of the rheumatology clinics.5 25 27 Data entry by touch screens was still possible during the study period.
For each patient, disease-specific PROs were collected according to the diagnosis recorded in DANBIO: rheumatoid arthritis (RA), psoriatic arthritis (PsA), axial spondyloarthritis (axSpA). All patients reported patient global score on a Visual Analogue Scale (VAS) (0–100 mm), fatigue (VAS), pain (VAS), Health Assessment Questionnaire (HAQ), Patient Acceptable Symptom Scale (PASS, yes or no) and external anchor question (for details, see footnote in table 1). For patients with axSpA and PsA, Bath-Ankylosing-Spondylitis items were also collected (details not shown).27
Patient characteristics* stratified by those who did and did not use DANBIO-from-home at least once during the study period (1.5 years after launching of system)
In the current study, patients in DANBIO were divided into two groups according to whether or not they entered PROs at least once using DANBIO-from-home during the study period (1.5 years, from 15 May 2020 until 1 December 2021) (in the following denoted ‘users’ vs ‘non-users’). Users were defined as patients who answered at least one of the voluntary surveys as well as patients who provided DANBIO-from-home entries during routine care appointments. Non-users were defined as patients without e-Boks, and patients who did not to use DANBIO-from-home despite e-Boks invitations. For all patients, we captured clinical and demographic characteristics in DANBIO according to the latest visit before March 2020 (baseline) to estimate disease status prior to the COVID-19 pandemic, that is, gender, age, diagnosis, disease duration, current use of biological disease-modifying antirheumatic drugs (bDMARDs) and PROs.
Characteristics of users versus non-users were reported with percentages or medians (IQRs) as appropriate. Characteristics associated with users were explored by univariable and multivariable logistic regression analyses adjusted by gender, age group (<40, 40–60, 61–80, >81 years), diagnosis (RA, PsA, AxSpA), disease duration, use of biologics, HAQ and PASS.
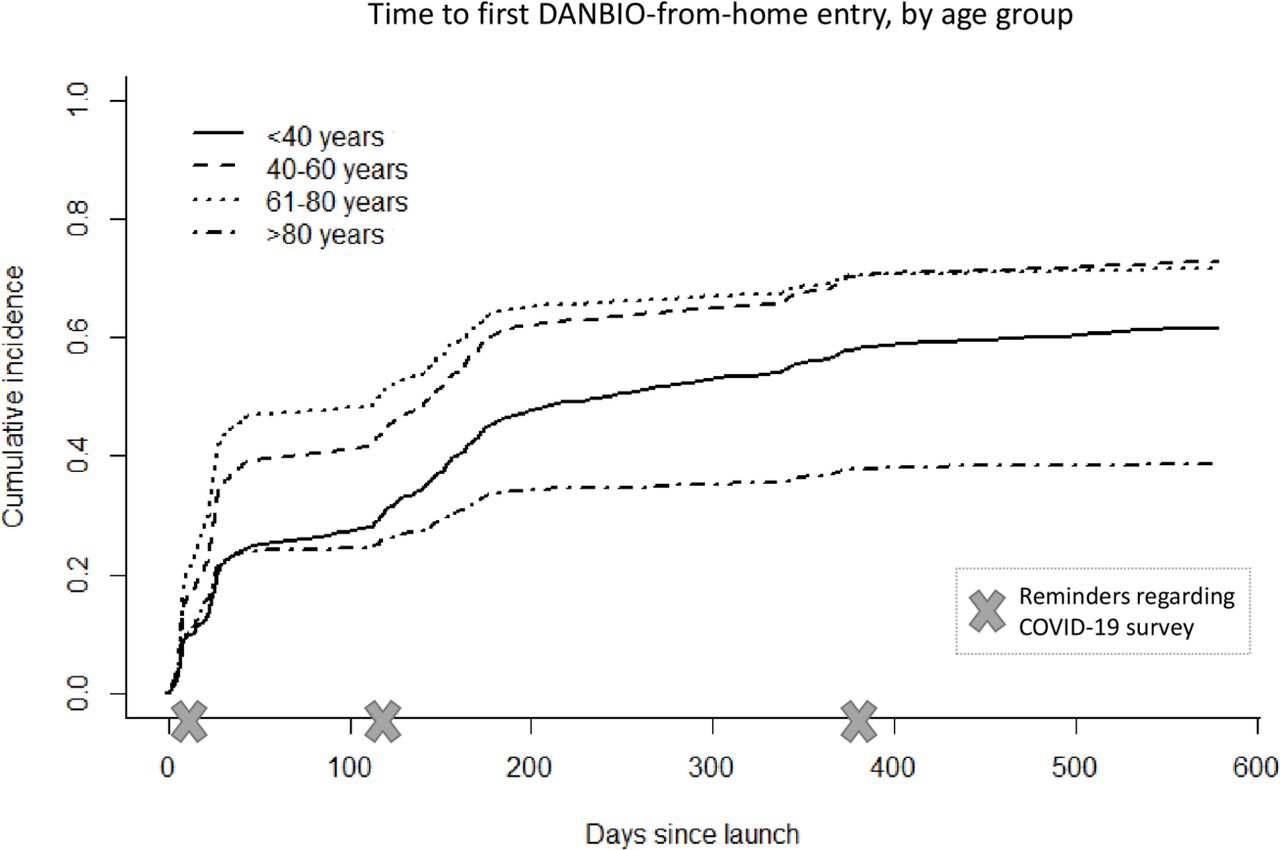
Time to first entry of PROs (number of days from 15 May 2020 until first entry) was presented as cumulative incidence curves stratified by age group.
Patient and public involvement
Patient representatives were actively involved in the phrasing of e-Boks invitations and in the design of the user interface of the DANBIO-from-home solution. Furthermore, two patient representatives, who also participate in the DANBIO steering committee, are affiliated to the patient organisation Gigtforeningen (the Danish Rheumatism Organization) and are coauthors of this manuscript.
Results
Of the 33 776 patients with IRD who were invited to use DANBIO-from-home, 68% (n=22 990) entered PROs using the online system at least once during the 1.5-year study period (users). In users, 16 772 (73%) provided entries twice or more during the study period (figure 1).

Number of entries per patient by the DANBIO-from-home solution during the study period. The figure includes non-users (number of entries=0).
In the 10 786 patients (32%) who did not use DANBIO-from-home, 51% had entered PROs by touch screens in the waiting areas. Similarly, among the 22 990 patients who had used DANBIO-from-home, 46% had also used the touch screens at least once during the study period.
Compared with non-users, users were slightly younger (62 vs 65 years old), but all age groups were well represented. Treatment with bDMARD was more frequent among users (37% vs 29%), and HAQ slightly lower (0.5 vs 0.625) (table 1).
In logistic regression analyses, factors associated with use of DANBIO-from-home in both univariable and multivariable analyses were: age group 40–60 or 61–80 years and not age >80 years (with age <40 years as the reference), treatment with a bDMARD and lower HAQ. Furthermore, in multivariable analyses, female gender and PASS ‘no’ were associated with use. Diagnosis and disease duration had no impact (table 2).
Clinical factors associated with use (yes vs no) of DANBIO-from-home; results of univariable and multivariable logistic regression analyses with ORs
Overall, the time to first entry was (median (IQR)) 27 (11–152) days and was longest in patients <40 years old (119 (24–184) days) and shortest in the 61–80 years age group (25 (8–139) days).
Time to first entry was longest in patients >80 years followed by the <40 years old. For all age groups, the use increased after invitations to participate in the COVID-19 surveys (figure 2).
{kind=link}
{kind=link}
Cumulated incidence curves showing time to first entry by the DANBIO-from-home solution, stratified by age group. Time scale is time from launch of solution (15 May 2020) until first entry.
Discussion
In this study, we explored the use of a nationwide web-based system for secure remote entry of PROs, which was launched for use in >30 000 patients with IRD. Our focus was on the overall use, and on clinical characteristics of the users compared with the non-users and the time to first entry. We found that the launch was successful since the system had been used by nearly 70% of eligible patients corresponding to 22 900 individuals during the first 1.5 years.
Our results are in contrast to experiences with web-based surveys in general, which have been reported to have overall lower response rates than, for example, paper based.32 Other Danish surveys that have approached patients by use of the e-Boks system have reported response rates in the range of 36%–54%.33–35 The high uptake should be seen in the light of several motivating factors: most patients were accustomed to the DANBIO infrastructure including the concept of contributing PROs as part of routine care.5 25 Thus, 77% of patients with established RA had at least one registration of PROs in 2019.36 DANBIO-from-home was launched during the COVID-19 pandemic, and the widespread cancellation of physical contacts or reallocation towards remote care is likely to have kick-started its use. Furthermore, it was launched as part of a survey regarding pandemic behaviour and anxiety, and up to six reminders were sent to the patients through the nationwide e-Boks system.28 30 From a previous validation and feasibility study, we knew that patients preferred DANBIO-from-home over those obtained in the waiting room, and that the PRO results were interchangeable.27
For several years, it has been debated how to monitor patients with chronic conditions including IRD.15 Concepts such as ‘open consultations’ and ‘on-demand access’ have previously been suggested to optimise and tailor timing of consultations in accordance with the patient’s needs—instead of routinely scheduling consults with regular intervals.8 Digital health solutions including video consultations, email correspondence and telephone consultations are examples of contact forms often used as an alternative to physical consultations, depending on preferences and the infrastructure available.7–9 37 There is no doubt that the pandemic further motivated these discussions.38 39
It was not the aim of the current study to explore use of consultation forms in detail. It is, however, important to emphasise that DANBIO-from-home is a voluntary add-on to the currently used entry of PRO via touch screens in the waiting areas. Thus, patients lacking digital skills, having physical limitations or similar barriers may continue using the existing in-clinic data entry where assistance from healthcare personnel is available.26 The touch screens were available during the study period and were used by almost half of the DANBIO-from-home users. DANBIO-from-home could serve as a valuable supplement to any consultation form—whether remote or physical. For remote-access consultations, PROs reported online could qualify shared decision-making, whereas in preparation for physical consultations, remote data entry is convenient and enables patients to report PROs in privacy.27 This demonstrates the advantages of providing patients with user-oriented flexible monitoring with ‘hybrid systems’ allowing them to pick the modality that suits them best at any time.37
The main scope of this study was to explore use versus non-use of DANBIO-from-home. We did not investigate the characteristics of patients with multiple data entries. Patients with stable rheumatic disease are routinely monitored in DANBIO annually.25 Thus, patients with multiple entries would be expected to be either participants in the COVID-19 survey (with three rounds of questionnaires), or patients with, for example, high disease activity or recent modifications of medication; that is, patient groups who might not be representative of the DANBIO cohort in general.
Although the system was used widely across different segments of patients, we found that patient-related factors, mainly age, gender and PASS, had a substantial impact on the use of DANBIO-from-home. Less widespread use in the elderly might indicate lack of IT skills or equipment. Low response rates in the elderly have previously been reported in digital surveys’16 33 but results are conflicting with other studies in which age was reported to be unrelated to digital preference.20 The more modest uptake in the younger age groups may reflect lack of time or interest, but improved after friendly reminders. The high entry rate in patients receiving bDMARDs is well explained by those patients having overall more severe and established disease, reinforced by the focus on immunosuppressive agents and infection risk during the pandemic.40 Patients who were not in an acceptable symptom state (ie, replied ‘no’ to the PASS question) used DANBIO-from-home more often. One may speculate that they were motivated because of poor disease control or flares. Socioeconomic factors and being outside the workforce have previously been reported to be associated with non-participation in surveys.33 Unfortunately, we had no data to explore this further.
Major strengths of this work include a considerable and representative nationwide sample, and the involvement of patient partners in the study design and as authors of this manuscript. Our study has limitations to consider. Thus, it is a weakness that despite widespread use of DANBIO-from-home, 10%–15% of patients lacked skills to access e-Boks and therefore could not use the system. We expect that this proportion will decrease over time. Furthermore, digital skills, ethnicity, educational status and comorbidities could potentially have impacted use of DANBIO-from-home, but we did not have access to these data for the current study. Missingness of some baseline variables was also a limitation.
The current implementation of DANBIO-from-home is a voluntary add-on to digital systems already in extensive use (e-Boks, DANBIO). Nevertheless, further investigation of barriers and facilitators is needed. Future studies should include the exploration of additional clinical factors associated with non-use, and the impact of age, especially why the younger patients were more reluctant users than the middle-aged.
In conclusion, a large-scale, web-based system for remote entry of PROs in patients with IRD was successfully launched and used by nearly 70% of patients during the first 1.5 years. Secure online entry of PROs increased the flexibility in the monitoring of patients and appeared to be a viable supplement to the existing entry in the waiting room, which should be kept as an alternative to some segments of patients.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplemental information. Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
Ethical approval was not required according to Danish legislation for research projects using online surveys (Komitélovens §14, stk. 2, www.nvk.dk, Journal Number 21074953). The project was approved by the regional data protection agency (P-2020-543, 14 May 2020). Data from DANBIO were obtained through the Danish Rheumatologic Quality Registry (DRQ) (RKKP DANBIO-2021-04-06). Patients gave online consent to participate.
Acknowledgments
Patients and Danish departments contributing to the DANBIO registry. Lundbeck foundation for funding.
References
Footnotes
Presented at Preliminary results have previously been presented (poster tour) at EULAR, Copenhagen, 2022.
Contributors Study conception and design—BG, DVJ and MLH. Acquisition of data—BG, DVJ, MLH and NSK. Statistical analysis—BG and NSK. All authors contributed to the interpretation of the data. BG and MLH wrote the manuscript. All authors critically revised the manuscript. All authors revised and approved the final manuscript to be published. BG is the guarantor for this manuscript.
Funding Partly funded by an unrestricted grant from the Lundbeck Foundation (grant number: R349-2020-629).
Competing interests BG—research grants: AbbVie, BMS, Pfizer and Sandoz. BG chairs the steering committee of the Danish Rheumatology Registry (DANBIO), which receives public funding from the hospital owners and funding from pharmaceutical companies. OH—research grants: AbbVie, Novartis and Pfizer. LT—speaker fees: from Roche, Novartis, Pfizer, UCB, Janssen and Eli Lilly. MO—research grants: AbbVie, BMS, Celgene, Merck, Novartis; consultancy and/or speaker fees: AbbVie, BMS, Boehringer-Ingelheim, Celgene, Eli Lilly, Galapagos, Gilead, Hospira, Janssen, Merck, Novartis, Novo, Orion, Pfizer, Regeneron, Roche, Sandoz, Sanofi and UCB. MPJ—speaker fees: AbbVie and Pfizer. RDO—research grants: AbbVie; consultancy and/or speaker fees: AbbVie, BMS, Boehringer-Ingelheim, Eli Lilly, Janssen, Merck, Novartis, Pfizer, Roche, Sanofi and UCB. AGL—research grant: Novartis; consultancy and/or speaker fees: AbbVie, Eli Lilly, Janssen, MSD, Novartis, Pfizer and UCB. MLH—AbbVie, Biogen, BMS, Celtrion, Eli Lilly Denmark, Janssen Biologics, Lundbeck Fonden, MSD, Pfizer, Roche, Samsung Biopis and Sandoz. MLH co-chairs EuroSpA, which generates real-world evidence of treatment of psoriatic arthritis and axial spondyloarthritis based on secondary data and is partly funded by Novartis. The remaining authors have nothing to declare.
Patient and public involvement statement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods’ section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.