Article Text

Abstract
Objective Successful uptake of biosimilars in rheumatology is limited by lack of real-world evidence regarding effectiveness of biosimilar-to-biosimilar switching. We investigated infliximab biosimilars CT-P13-to-GP1111 switching among patients with rheumatoid arthritis (RA), psoriatic arthritis (PsA) and axial spondyloarthritis (AxSpA).
Methods Observational cohort study from the DANBIO registry. Patients were classified as originator-naïve or originator-experienced. Retention rates of 1-year GP1111 treatment were explored (Kaplan-Meier). We identified baseline factors (at the time of switch) associated with withdrawal of GP1111 (multivariable Cox-regression analyses with HRs including originator treatment history). Changes in subjective and objective measures of disease activity 4 months before and after the switch were assessed in individual patients.
Results Of 1605 patients (685 RA, 314 PsA and 606 AxSpA, median disease duration was 9 years, 37% in Clinical Disease Activity Index/Ankylosing Spondylitis Disease Activity Score remission), 1171 were originator-naïve. Retention rates at 1-year were 83% (95% CI: 81% to 85%) and 92% (95% CI: 90% to 95%) for the originator-naïve and originator-experienced, respectively. GP1111 retention rates were higher in originator-experienced compared to originator-naïve with RA (HR=0.4 (95% CI: 0.2 to 0.7)) and PsA (HR=0.2 (95% CI: 0.1 to 0.8)), but not significantly for AxSpA: HR=0.6 (95% CI: 0.3 to 1.2). Lower disease activity was associated with higher retention. Changes in disease activity preswitch and postswitch were close to zero.
Conclusion This real-world observational study of more than 1600 patients with inflammatory arthritis showed high 1-year retention following a nationwide infliximab biosimilar-to-biosimilar switch. Retention was higher in originator-experienced and in patients with low disease activity, suggesting outcomes to be affected by patient-related rather than drug-related factors.
- biosimilar pharmaceuticals
- infliximab
- arthritis, psoriatic
- arthritis, rheumatoid
- spondylitis, ankylosing
Data availability statement
Data are available upon reasonable request. All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- biosimilar pharmaceuticals
- infliximab
- arthritis, psoriatic
- arthritis, rheumatoid
- spondylitis, ankylosing
WHAT IS ALREADY KNOWN ON THIS TOPIC
The lack of randomised trials and real-world evidence regarding outcomes following switch from one biosimilar to a second of the same originator limits the uptake of biosimilars in routine care rheumatology settings.
WHAT THIS STUDY ADDS
In this observational cohort study, we explored 1 year outcomes among more than 1600 patients with rheumatoid arthritis, psoriatic arthritis and axial spondyloarthritis following a nationwide infliximab biosimilar-to-biosimilar switch (CT-P13 to GP1111).
Treatment retention at 1 year was high in both groups, with lower withdrawal rates among originator-experienced and patients with lower disease activity at the time of switch.
Disease activity in individual patients 4 months before and after switch was stable with no clinically relevant differences.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
A mandatory infliximab biosimilar-to-biosimilar switch was well tolerated by patients. Retention was influenced by patient-related factors.
Biosimilar drugs are highly similar versions of the originator biologic disease-modifying antirheumatic drugs (bDMARDs). Their use is motivated by cost savings.1 Different switch scenarios are emerging with increasing availability of biosimilars, including switching from one biosimilar to a second of the same originator,2 in this paper termed biosimilar-to-biosimilar (B2B)-switching.
For the treatment of rheumatoid arthritis (RA), psoriatic arthritis (PsA) and axial spondyloarthritis (AxSpA) evidence regarding infliximab B2B-switching is limited.1 3 4 Randomised clinical trials (RCTs) have mainly investigated the efficacy and safety of switching from originator infliximab to a corresponding biosimilar.2 5–8 Real-world evidence supporting infliximab B2B-switches stems from a few minor studies in, for example, psoriasis and inflammatory bowel disease (IBD).2 9–12 Concerns regarding B2B-switches relate to effectiveness, safety and immunogenicity.1 13 Previous studies on originator-to-biosimilar switching in real-world patients have indicated an impact of patient-related factors (eg, treatment history and disease activity at the time of switching) on treatment outcomes14–17; however their role remains unclear in B2B-switching. As recommended in the consensus document by Kay et al,18 outcomes of B2B-switching should be assessed in real-world registries.
The uptake of biosimilars is high in Denmark.19 20 Mandatory nationwide switches of, for example, infliximab have been conducted: first from originator to CT-P13 (year 2015), followed by switch to GP1111 (year 2019) in accordance with Danish guidelines.21 Clinical outcomes were prospectively monitored in the nationwide clinical registry, DANBIO,22 providing a unique opportunity for the study of real-world effectiveness following B2B-switching.
In this study, we aimed to investigate the effectiveness of infliximab biosimilar CT-P13-to-GP1111 switching among patients with RA, PsA and AxSpA, including those patients who had previously switched from originator to CT-P13 (originator-experienced) and those who were originator-naïve. Furthermore we aimed to identify factors associated with retention to treatment following the switch.
Methods
Study design
Observational cohort study. More than 95% of adults with inflammatory rheumatic disease treated with bDMARDs in routine care are prospectively followed in DANBIO.22 23 Using civil registration numbers, patient-level information from DANBIO was enriched with previous comorbidities and vital status from The Danish National Patient Registry, and The Danish Civil Registry, respectively (online supplemental table S1).24 25
Supplemental material
Study population
We included patients with a clinical diagnosis of RA, PsA or AxSpA, who performed a B2B-switch from CT-P13 to GP1111 between 1 April 2019 and 1 February 2020 (date of switching=baseline). Patients were divided into two subgroups: originator-naïve and originator-experienced (figure 1).

Study population and definition of the two subgroups according to originator infliximab treatment history. *Switched to CT-P13 in the period 1 May 2015 to 1 March 2016. A time gap of 0–120 days between stop of originator and start of biosimilar was allowed to comply with registration practice.**Based on following International Classification of Diseases (ICD)-10 codes: For RA: M05.9, M06.0, M06.9, M13.0, for PsA: M073.A, M073.B, M46.8 in combination with M07.3 and for AxSpA: M45.9, M46.1, M46.8, M46.9, also M45.9 and M46.8 in combination with M02.9, M07.2, M07.4, M07.5 and/or H20.0. Also minimum one visit in DANBIO after 1 April 2019, and aged ≥18 years at the time of treatment start with a biologic disease-modifying antirheumatic drug (bDMARD). ***Switched to GP1111 in the period 1 April 2019 to 1 February 2020. AxSpA, axial spondyloarthritis; PsA, psoriatic arthritis; RA, rheumatoid arthritis.
Outcomes
The primary outcome was 1-year GP1111 treatment retention in the two subgroups, overall and stratified by indication (RA, PsA and AxSpA). The key secondary outcome was baseline factors associated with GP1111 treatment withdrawal for both groups combined (stratified by indication). Other secondary outcomes included reasons for withdrawal and changes in disease activity 4 months before and after the switch (stratified by indication).
Follow-up
Patients were followed-up for 1 year after baseline. Treatment duration was the number of days each patient maintained treatment with GP1111, until withdrawal (=first missed dose irrespective of reason), death, lost to follow-up or data-cut, whichever came first. Temporary interruptions of less than 3 months’ duration (eg, due to surgery, infections) were disregarded. Reasons for withdrawal were identified according to predefined categories in DANBIO.
Approvals
Danish registry studies neither require patient consent nor ethical approval. The study was approved by the Danish Data Protection Agency (RH-2015–209, 04145). Data from DANBIO was obtained through the Danish Rheumatologic Quality Registry (RKKP DANBIO-2021-07-09).
Statistical analysis
All statistical analyses were conducted using R (V.3.6.1).26 P values<0.05 were considered statistically significant.
Clinical characteristics are presented as medians (ranges) or numbers (percentages), as appropriate. GP1111 treatment retention was explored with Kaplan-Meier curves.
Baseline factors associated with retention were explored with univariable and multivariable Cox regression analyses. These were conducted for both subgroups combined (ie, all patients who switched from CT-P13 to GP1111) with previous originator treatment history included as a covariate. Analyses were performed as crude, age-adjusted and gender-adjusted, fully adjusted and further stratified by indication. For fully adjusted analyses, the following a priori defined variables were included based on literature review14 19 20: age, gender, originator treatment history (yes/no), concomitant methotrexate (yes/no), C-reactive protein (CRP), patient global score on a Visual Analogue Scale (VAS) and number of comorbidities ≥1 (yes/no).
Disease activity in individual patients was assessed 4 months before baseline, at baseline and 4 months after baseline and changes preswitch and postswitch were calculated and compared using a paired t-test. If a patient had no registration of disease activity, data was registered as missing. It was not considered meaningful to impute missing data on disease activity due to the fluctuating course of rheumatic diseases.
Results
In total, 1605 patients performed an infliximab B2B-switch and were included; 1171 originator-naïve and 434 originator-experienced (table 1, online supplemental tables S2 and S3). At baseline, median disease duration was 9 years and 29–42% were in Clinical Disease Activity Index (CDAI) or Ankylosing Spondylitis Disease Activity Score remission.
Characteristics of originator-naïve and originator-experienced switchers at the time of GP1111 switch, stratified by indication
Originator-naïve patients were younger, had shorter disease duration and fewer comorbidities than those who were originator-experienced. Furthermore, baseline subjective and objective disease markers (eg, CRP, CDAI, patient global VAS) were higher, and fewer were in remission. Patients in both subgroups had median three visits during follow-up (table 1).
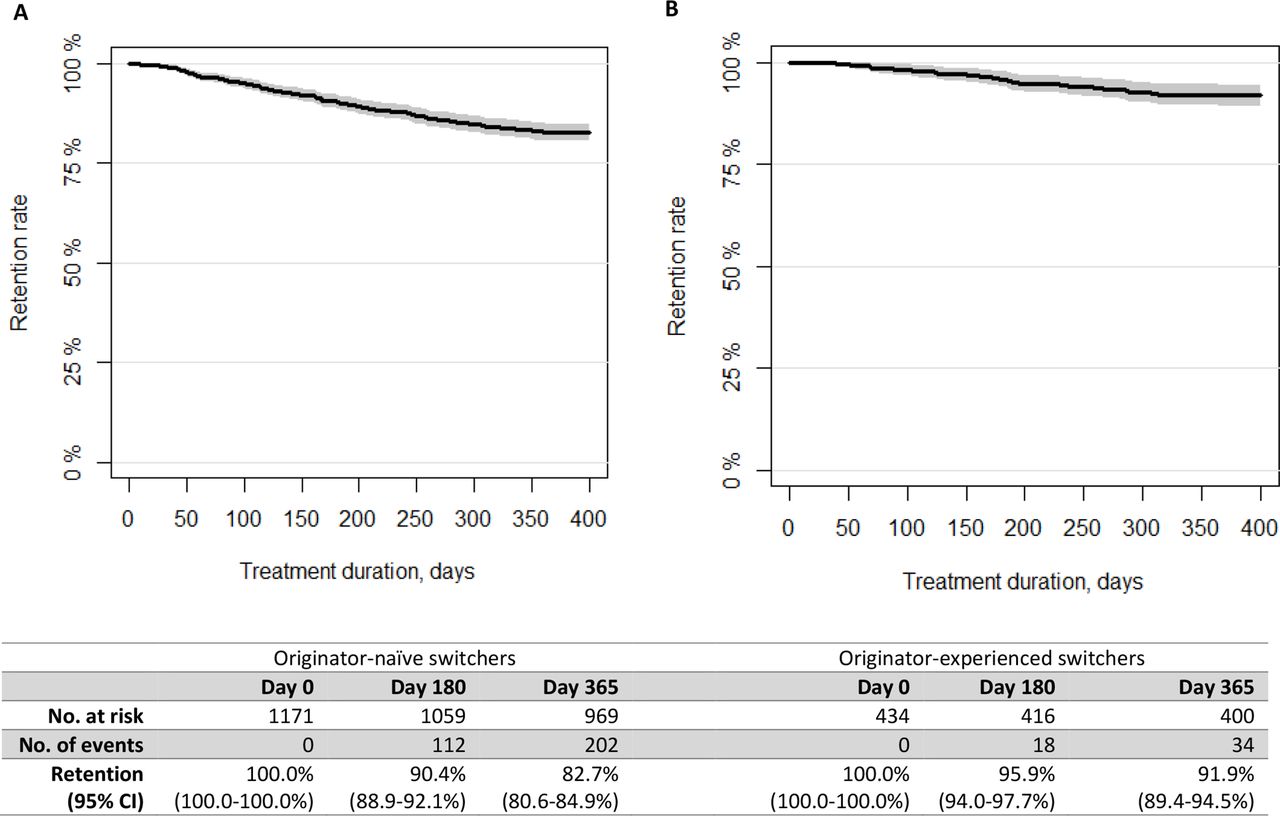
At 1 year, 83% (95% CI: 81% to 85%) of the originator-naïve and 92% (95% CI: 90% to 95%) of the originator-experienced switchers maintained GP1111 treatment (figure 2). Stratified by indication, the retention rate was 80–87% for originator-naïve (highest in AxSpA) and 90–96% for originator-experienced switchers (lowest in RA) (online supplemental figure S1).

{kind=link}
{kind=link}
Kaplan-Meier plots of crude treatment retention rates in GP1111-treated patients ((A) originator-naïve and (B) originator-experienced switchers)*.*The grey shaded area on the figures represents the 95% CI.
Main reasons for withdrawal were lack of effect (originator naïve 60% and experienced 29%) and adverse events (16% and 23%) (table 2).
Reasons for GP1111 withdrawal during 1-year follow-up
Risk of GP1111 withdrawal was lower in originator-experienced compared with naïve patients, mainly in patients with RA (HR=0.36, 95% CI: 0.19 to 0.68) and PsA (HR=0.23, 95% CI: 0.07 to 0.75), respectively. For all indications, higher baseline disease activity was associated with higher withdrawal (table 3).
Baseline variables associated with GP1111 treatment withdrawal, performed in all switch patients (n=1605) and stratified by diagnosis
For both originator-naïve and originator-experienced switchers, changes in disease activity preswitch and postswitch in individual patients were close to zero for all measures with no statistically significant differences (table 4).
Disease activity and functional status 4 months prior to GP1111 switch, at the time of switch and 4 months after switch, stratified by indication and by originator treatment history
Discussion
In this nationwide cohort study among more than 1600 B2B-switch patients, we found high GP1111 treatment retention rates, with 8 of 10 originator-naïve switchers and 9 of 10 originator-experienced switchers maintaining treatment after 1 year. Similar rates have been reported in RCTs and observational studies for infliximab originator and biosimilar CT-P13.5 6 14 27 Furthermore, we demonstrated stable disease activity before and after switching.
Biosimilar use and switch procedures vary across countries.28–31 In some countries biosimilars are hardly used—potentially with huge impact on drug expenditures and access to treatment.32 In Denmark, biosimilars are implemented at the time of marketing based on national tenders. The bDMARDs are provided free of charge to all patients via a tax-based system, and mandated switch procedures are implemented according to national guidelines.14 19 20
The European Medical Agency’s approval of the biosimilar GP1111 was based on a phase III trial in previously infliximab-naïve patients with RA randomised to either GP111 or originator infliximab.8 33 The extrapolation of this approval to also cover PsA, AxSpA, IBD and psoriasis could be challenged by factors differing across indications (age, genetics, drug dose, comorbidities, co-medications) potentially affecting immunogenicity, pharmacokinetics and/or dynamics.2 34 Furthermore, the highly selected patients included in RCTs are not representative of patients in routine care, who are older and have more comorbidities or other complicating characteristics.35
Current evidence regarding B2B-switching is very limited. To date, no RCT or observational study has investigated infliximab B2B-switches in patients with inflammatory rheumatic disease. In a small IBD cohort (n=176) 1 year treatment retention rates for originator-experienced and originator-naïve were similar (85% vs 87%).12 Unchanged retention and disease activity following infliximab B2B-switching have also been reported in other small observational studies among patients with IBD (n between 87 and 271) and psoriasis (n=96).36–39 Well-conducted observational studies based on prospective data collection in well established registries in countries performing nationwide systematic switches can provide important evidence and may challenge the need for systematic clinical studies.18 40
Our study provides important knowledge regarding real-life effectiveness for different switch scenarios among patients with inflammatory arthritis. The originator-experienced patients had been treated with infliximab for many years and had lower disease activity. Both previous originator treatment history and lower disease activity at the time of switch, especially subjective markers (eg, patient global VAS), were associated with higher retention. This suggests treatment outcomes to be more affected by patient-related than drug-related factors and indicates the presence of a ‘nocebo-effect’, that is, negative expectations towards the drug.17 33 Similar findings have been reported for originator to biosimilar infliximab switching.2 14 The proportion of patients who discontinued treatment due to adverse events was similar to those previously reported in other real-world studies of biosimilar infliximab.14 29–31 Details regarding type of adverse event could not be explored due to lacking data in DANBIO.
The Danish nationwide strategy of frequent mandatory biosimilar switches combined with routine-care prospective follow-up in DANBIO contributed a large cohort with high data completeness. Limitations include the reporting of associations and not definitive causal relationships due to the observational study design. Despite adjustment for several baseline variables, residual confounding cannot be excluded.
In conclusion, infliximab B2B-switching, both in originator-naïve and originator-experienced patients with inflammatory arthritis, was effective and safe. Retention to GP1111 was higher in originator-experienced switchers and patients in remission at the time of the switch, suggesting outcomes to be more affected by patient-related than drug-related factors.
Data availability statement
Data are available upon reasonable request. All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants but was not approved by Danish registry studies neither require patient consent nor ethical approval. The study was approved by the Danish Data Protection Agency (RH-2015-209, 04145). Data from DANBIO was obtained through the Danish Rheumatologic Quality Registry (DRQ) (RKKP DANBIO-2021-07-09).Danish registry studies neither require patient consent nor ethical approval. The study was approved by the Danish Data Protection Agency (RH-2015-209, 04145). Data from DANBIO was obtained through the Danish Rheumatologic Quality Registry (DRQ) (RKKP DANBIO-2021-07-09).
Acknowledgments
We are grateful to all patients and Danish departments of rheumatology for reporting to the DANBIO registry. The authors acknowledge Sandoz for supporting the work. Preliminary findings have been presented orally at the EULAR congress.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
MLH and BG are joint last authors.
MLH and BG contributed equally.
Contributors Study conception and design: HN, BG and MLH. Acquisition of data: HN, BG, MLH, FM and NSK. Statistical analysis: HN, BG and MLH. All authors contributed to the interpretation of the data. HN, BG and MLH wrote the manuscript. All authors critically revised the manuscript. All authors revised and approved the final manuscript to be published. HN is the guarantor.
Funding Funding support was provided by Sandoz (Hexal AG) without influence on the data collection, statistical analyses, manuscript preparation or decision to submit.
Competing interests HN: Research grant from AbbVie and Sandoz. AGL: AbbVie, Eli Lilly Denmark A/S, Janssen-Cilag A/S, MSD, Novartis, Pfizer, UCB teaching or consultancy fees. OH: AbbVie, Pfizer, Novartis. MLH: AbbVie, Biogen, BMS, Celtrion, Eli Lilly Denmark A/S, Janssen Biologics B.V, Lundbeck Fonden, MSD, Pfizer, Roche, Samsung Bioepis, Sandoz. Furthermore, chair of the steering committee of the Danish Rheumatology Quality Registry (DANBIO), which receives public funding from the hospital owners and funding from pharmaceutical companies. Co-chair EuroSpA, which generates real-world evidence of treatment of psoriatic arthritis and axial spondyloarthritis based on secondary data and is partly funded by Novartis. BG: BMS, Pfizer, Sandoz (research grants).
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.