Article Text

Abstract
Diagnosing peripheral spondyloarthritis (pSpA) remains a significant challenge due to the lack of specific disease biomarkers and the overlap with other SpA subtypes, mainly psoriatic arthritis (PsA), which represents a diagnostic challenge particularly in the absence of skin psoriasis (PsA sine psoriase). This narrative review aimed to compare the epidemiology, genetic susceptibility, pathophysiology, classification criteria, disease phenotype and burden, and therapeutic guidelines between patients diagnosed with pSpA and those with PsA sine psoriase, to determine if the two entities should be considered jointly or distinctly. Globally, pSpA appears to be more inclusive compared with PsA sine psoriase. Areas of similarities include age of onset, number of joints involved and prevalence of axial involvement. However, patients with pSpA have a male gender predominance, a higher prevalence of HLA-B27, enthesitis and involvement of large joints of the lower limbs, whereas patients with PsA sine psoriase have a higher prevalence HLA-Cw6, dactylitis and involvement of hand distal interphalangeal joints. Therefore, the difference between pSpA and PsA sine psoriase goes beyond semantics. The few dissimilarities should drive scientific efforts to reach a better characterisation of pSpA as an individual disease. Accordingly, randomised clinical trials should target patients with well-defined pSpA to identify effective therapies in this population.
- Spondyloarthritis
- Arthritis, Psoriatic
- Spondylitis, Ankylosing
- Epidemiology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THE SUBJECT
Peripheral spondyloarthritis (pSpA) poses a significant diagnostic challenge due to the lack of biomarkers and the overlap with other SpA subtypes, particularly psoriatic arthritis (PsA) sine psoriase.
WHAT THIS STUDY ADDS
pSpA appears to be a more inclusive term compared with PsA sine psoriase when used in clinical studies and is associated with a higher prevalence of male gender, HLA-B27, enthesitis and involvement of large joints of the lower limbs, whereas PsA sine psoriase is associated with a higher prevalence of HLA-Cw6, dactylitis and involvement of hand distal interphalangeal joints.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
The difference between pSpA and PsA sine psoriase goes therefore beyond semantics and the few dissimilarities should drive scientific efforts to reach a better characterisation of pSpA as an individual disease and identify specific effective therapeutic options.
Introduction
Understanding and defining a certain disease are two crucial conditions for estimating its burden on the population and for applying an adequate treatment plan. In times where limited healthcare resources are to be appropriately distributed, a disease must be clearly characterised and conditions representing a higher unmet need must be identified.1 However, defining a particular disease can be challenging, particularly in the absence of a sensitive and specific marker. Peripheral spondyloarthritis (pSpA) is such a condition, where classification criteria were published by the Assessment of SpondyloArthritis international Society (ASAS) in 20112 but where the application of this classification is still unexplored in clinical studies, with only very few exceptions.3 4 In addition to the absence of a biomarker, the diagnosis of pSpA in daily practice is particularly challenged by the clinical overlaps with other diseases of the SpA group,5–7 especially psoriatic arthritis (PsA) mainly defined by the Classification Criteria for Psoriatic Arthritis (CASPAR) criteria8 and axial SpA (axSpA) defined by the ASAS axSpA classification criteria,9 which are considered as much more clearly demarcated SpA subtypes. In fact, the nomenclature of pSpA continues to be more ambiguous in comparison to PsA and axSpA and has been used sometimes interchangeably with some SpA subsets such reactive Arthritis, undifferentiated SpA, and PsA, especially in the absence of associated skin psoriasis, namely the PsA sine psoriase entity.10 This entity poses a particular conceptual definition challenge. Does it refer to a patient with typical PsA who has not developed yet a skin psoriasis, but who will eventually, if followed long enough? Or to a patient who might have a hidden form of psoriasis that was not detected at the time of clinical assessment? Or to a patient who only had a family history of psoriasis? Therefore, it is in the absence of manifest psoriasis that the diagnostic confusion emerges between pSpA and PsA.
A debate about lumping these SpA subtypes altogether or splitting them has been going on for several years, and the pros and cons of each approach are still broadly discussed.11–13 Nevertheless, going beyond the semantic debate, the stakes for a proper definition are now much higher because of the recent dramatic increase in the choice of approved, yet expensive, drugs for PsA14 and the absolute necessity to identify the patients, particularly those with the poorly defined pSpA, who can benefit from these new therapies. In particular, the question remains whether the two poorly defined SpA subtypes, that is, pSpA and PsA sine psoriase, should be grouped together—and consequently treated in the same way—or should they be regarded as two separate diseases. With new guidelines developed recently for PsA,15 including more than 10 classes of potential pharmacological treatments, defining the diseases is more imperative than ever.
We aimed to compare the epidemiology, genetic susceptibility, pathophysiology, classification criteria, disease phenotype and burden, and therapeutic guidelines between patients diagnosed with pSpA and those with PsA sine psoriase. To this end, we performed a narrative review with a focus on international SpA cohorts, to determine if the two entities should be considered jointly or distinctly.
Epidemiology
Prevalence and geographical distribution
The SpA as a group has a prevalence of 0.2%–1.7%,16 with lowest percentages from South-East Asia and highest from the Northern Arctic communities. Methodological differences also partially account for the wide range of estimates across different studies. However, few epidemiological studies used the ASAS classification criteria to define SpA subgroups.
Peripheral spondyloarthritis
Crude prevalence and incidence rates of pSpA are lacking.10 Nevertheless, the prevalence relative to the whole group of SpA has been evaluated in several studies and ranges between 22.8% and 28.5% of all SpA. For instance, in the proportion of pSpA was 22.8% in the Spanish Esperanza SpA cohort,17 which included 377 patients with SpA, 26.8% in the Dutch SpA cohort18 included 314 patients with SpA, and 28.5% in the first 122 SpA patients of the Be-Giant early SpA cohort.19 Similarly, in the large GAZEL cohort comprising 20 625 employees in the French national gas and electrical company,20 the prevalence of SpA as screened by a validated questionnaire was 0.43%; of which 25% fulfilled the ASAS pSpA criteria.
Finally, two global ASAS-endorsed international studies evaluated patients with SpA worldwide in the recent past years. First, in the Comorbidities in SpA (COMOSPA) study, including 3985 patients with SpA from 22 countries,21 56.4% had peripheral articular involvement, and 14% fulfilled the ASAS pSpA classification criteria. Importantly, patients who fulfilled both ASAS axial and pSpA classification criteria were exclusively classified in the axial group.22 In addition, psoriasis and the absence of HLA-B27 were associated with the development of peripheral symptoms. Second, the most recent peripheral manifestations in SpA (PerSpA) study included 4465 patients with SpA from 24 countries,5 9.7% were considered as having pSpA as the main diagnosis made by the rheumatologist. The definition of pSpA as ‘main diagnosis’ probably accounts for the lowest prevalence compared with the other cohorts. Including patients with overlapping features would probably increase this prevalence, as 78% of the 4465 patients had ever suffered from at least one peripheral musculoskeletal manifestation. Peripheral disease was reported in 57%, enthesitis in 44% and dactylitis in 15%. When considering different region of the world, the highest prevalence of peripheral joint disease (80%) was found in Latin America.
In brief, taking data from cohorts where overlap was allowed, the prevalence of pSpA ranged between 22.8% and 28.5% of all SpA patients. However, when considering the disease as a main entity from the COMOSPA (based on classification criteria) and the PerSpA (based on the rheumatologist diagnosis) international studies, the prevalence of pSpA was lower, ranging from 9.7% to 14% of all SpA.
PsA sine psoriase
Prevalence data for PsA sine psoriase can be derived from PsA cohorts, as very few studies addressed the PsA sine psoriase entity alone. The prevalence of this entity depends on the studied population and mainly on the length of the follow-up.
Psoriasis occurs in 2 to 4% of adults,23 and around 20%–30% of psoriasis patients develop PsA.24 25 A prospective cohort included 464 patients with psoriasis without any inflammatory arthritis at presentation; 51 of those developed PsA during an 8-year follow-up, indicating an annual incidence of 2.7%.26
Two reviews of 84 and 28 studies, respectively,16 27 found a prevalence of PsA ranging from 0.01% (95% CI 0.00% to 0.17%) in the Middle East to 0.19% (95% CI 0.16% to 0.32%) in Europe for the first review, and from 0.02% to 0.67% (also a higher prevalence for Asian countries) with a median of 0.13% for the second one. The different estimates between studies were explained by the different set of criteria used, the geographic area and the time the data was collected (lower prevalence for studies conducted before 1999). Studies using only the CASPAR classification criteria estimated the prevalence of PsA around a median of 0.12%. Furthermore, the incidence ranged from 3 to 41.3 cases every 1 00 000 patients-years (PY) with a median of 8.3 every 100 000 PY.
Although psoriasis usually antedates arthritis, it may also appear much later in the disease course in about 20% of the cases.28 29 In a UK study including 6087 patients from two PsA cohorts (UK Clinical Practice Research Datalink and Bath cohort), a minority of patients, 7.1% and 14.8% respectively, received their PsA diagnosis before the psoriasis occurrence, with a median time between diagnoses of 7 and 8 years.30 Scarpa et al31 32 reported that arthritis preceded the skin lesion by more than 10 years in 1.6% of PsA patients, but that gap may go up to 21 years according to some clinical case reports.31 32 Importantly, sometimes the psoriasis is just ‘hidden’ and not readily identified in areas such as the scalp, nails, flexural areas and natal cleft.33 Interestingly, these are the phenotypes of psoriasis most likely associated with the development of PsA.34 In a retrospective study of 162 patients with PsA,35 PsA sine psoriase has been reported in 1.8%.
Data from the COMOSPA study36 showed that 22.4% (894/3,984 patients with SpA) fulfilled the CASPAR criteria. Of those 894 patients, 26.4% also fulfilled the pSpA ASAS criteria, and 39.6% also fulfilled the axSpA ASAS criteria. In patients fulfilling the CASPAR criteria, 76.4% had psoriasis. Thus, it can be deduced that 24.6% of patients with PsA, according to the CASPAR criteria (5.5% of the whole COMOSPA cohort), had PsA sine psoriase.
Similarly, in the PerSpA study,5 23.1% (1033/4,465) were considered to have PsA as the main diagnosis by the rheumatologist. In these patients, with a mean symptom duration of 16.8 years, psoriasis was present in 86.5% of the cases. Thus, it can be deduced that 13.5% had PsA sine psoriase, that is, 3.1% of the whole PerSpA cohort.
In summary, using the data from COMOSPA and PerSpA, the prevalence of PsA sine psoriase ranged from 3.1% to 5.5% of all SpA (lower than that of pSpA), indicating that pSpA might be a more inclusive entity.
Age at onset
Very few studies evaluated the demographic characteristics in patients with pSpA and PsA sine psoriase (table 1). The mean age of patients ranged from 32.8 to 42.2 years in pSpA (data derived from the Spanish Esperanza, Belgian Be-Giant, Dutch cohort and international PerSpA studies)17–19 and from 30 to 44 years in three cohorts of patients with PsA sine psoriase including 20, 57 and 100 patients, respectively,37–39 suggesting a more or less similar range of age at onset for both entities.
Epidemiological characteristics and disease phenotype of peripheral spondyloarthritis (SpA) and psoriatic arthritis (PsA) sine psoriase
Genetic susceptibility
The aetiology of the SpA disease group, as in all chronic inflammatory diseases, is still unknown, with an interplay between genetic and environmental factors creating a complex mechanism that cannot always be elucidated.
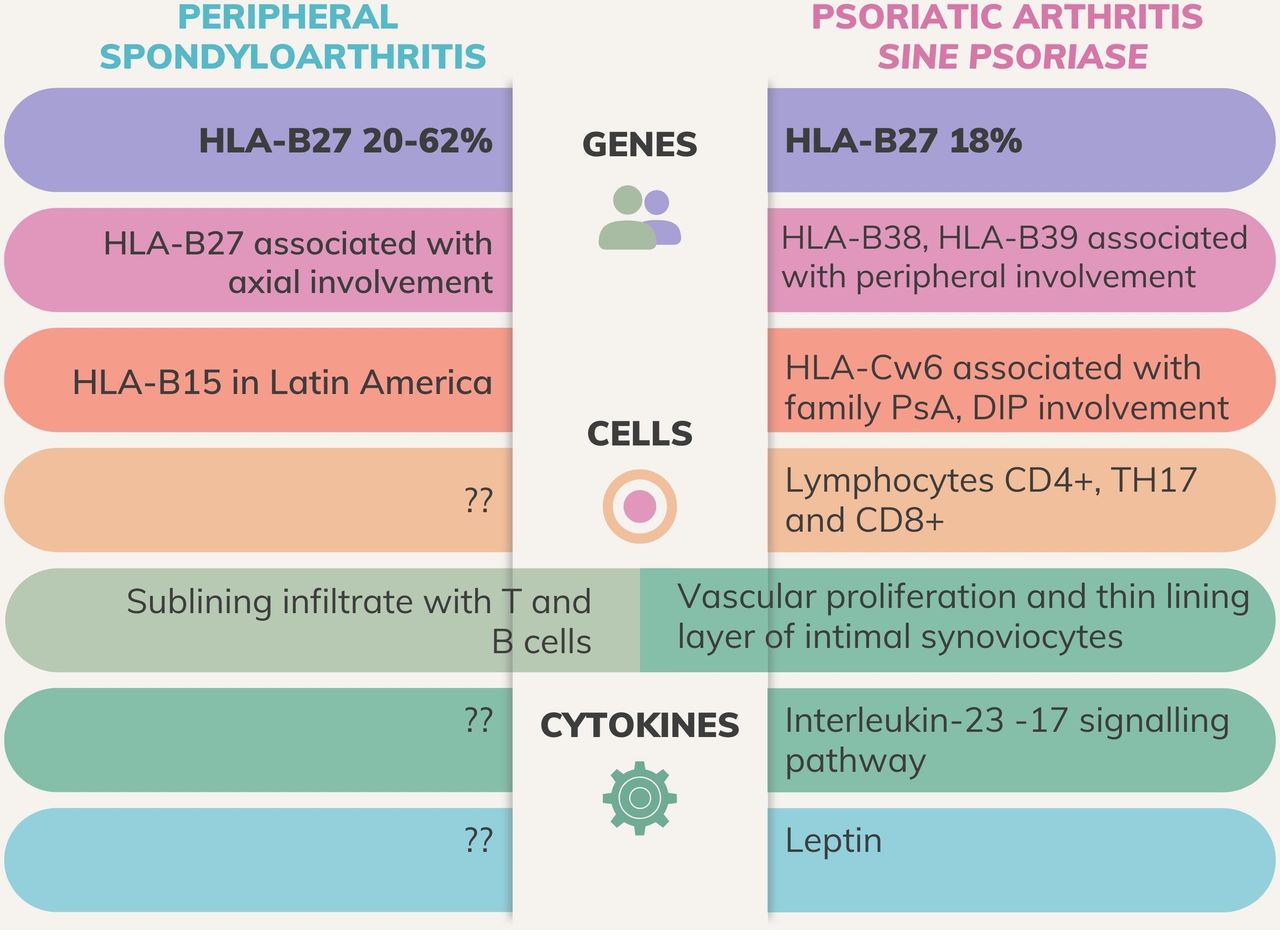
When mentioning genetic factors, Human Leucocyte Antigen (HLA)-B27 is one of the common features holding the SpA group together. In pSpA, the prevalence of HLA-B27 ranges from 27% to 62.3%.5 17 18
It is estimated that genes within the Major Histocompatibility Complex (MHC) account for less than 50% of the heritable aspects.11 HLA-B27 has a low prevalence in the non-axSpA, which indicates that it does not define disease diagnosis. For example, HLA-B15 was significantly associated with SpA in a Latin-American study, and almost exclusively in patients with pSpA.40
In PsA, data from the PerSpA study confirmed the lower prevalence of HLA-B27, that is, 18.2%.5 In other studies among patients with psoriasis, HLA-B27 was associated with an early development, whereas HLA-Cw6 was associated with a delayed onset of PsA.26 41–43 Moreover, HLA-B27 was also associated with axial involvement and symmetric sacroiliitis in PsA,38 44 whereas it was negatively associated with a family history of psoriasis.38
Moreover, in PsA, HLA-Cw6 was associated with the family history of psoriasis, dactylitis and the impairment of distal interphalangeal joints (DIP),38 45 and Scarpa et al suggested including HLA-Cw6 in the definition of PsA sine psoriase. Several other MHC alleles are found in PsA including HLA-B08, HLA-B38 and HLA-B39; the latter two are mostly associated with peripheral polyarticular involvement.38
Other non-MHC genes related to PsA have been studied. The killer-cell immunoglobulin-like receptor (KIR) genes have a prominent role in the genetic susceptibility to PsA. Some alleles, notably KIR2DS2, tend to interact with HLA-C molecules inducing an inflammatory response.46
In contrast, the association with other MHC alleles, particularly HLA-Cw6, in pSpA was not well studied.
Pathophysiology
A disease can be defined by its phenotype or by its underlying pathophysiology; when considering the latter definition, different phenotypes may be the result of the same intrinsic cellular and molecular mechanisms. Therefore, bringing up the resemblance in the pathophysiology of pSpA and PsA sine psoriase adds to the cohesion of the SpA group.
Histopathology studies of synovial biopsies found that PsA, either oligoarticular or polyarticular, resembles that of other SpA subtypes (ankylosing spondylitis and undifferentiated SpA), whereas both groups can be differentiated from rheumatoid arthritis (RA) based on these same synovial features, confirming that peripheral synovitis in PsA belongs to the SpA concept. In all SpA subtypes, vascularity and neutrophil and CD163+ macrophage counts were greater. Whereas in RA, lining layer thickness and the number of CD83+ dendritic cells were greater. No significant differences were observed between PsA and other forms of SpA.47 PsA synovitis is characterised by a sublining infiltrate with T and B cells, vascular proliferation and a relative thin lining layer of proliferating intimal synoviocytes.48 PsA also associates with genetic polymorphisms involved in the interleukin (IL)-23–IL-17 signalling pathway.49 In fact, synovial fluid of PsA patients includes increased levels of CD4+, especially Th17 and CD8+. Frequencies of polyfunctional T-cells correlated with disease activity.50 Trauma or biochemical stress at tendon insertion leads to the production of IL-23, which activates Th17 cells and releases IL-22 and TNF, which leads to inflammation erosion and bone formation. IL-22 activates osteoblasts as well, leading to the formation of enthesophytes in peripheral entheses and joints. Inflammation in the synoviocytes, along with higher levels of TNF and IL-17, leads to activation of osteoclasts via RANKL expression which leads to bone resorption.51
One major proof of the pivotal role of the IL-23/IL-17-axis in PsA is the success of monoclonal antibodies targeting these cytokines. Indeed, IL-23-driven enthesitis has been postulated to be the culprit of inflammation in SpA, as a results of a disrupted barrier integrity in patients with psoriasis.52 Moreover, several innate immune cells express IL-23 receptor and can produce IL-17 in pSpA.53 However, this hypothesis was not confirmed in the non-psoriatic subtypes of pSpA and in PsA sine psoriase yet.
When comparing the adipokine pattern (serum levels of TNF-α, IL-6, leptin, resistin, visfatin and ghrelin) between 42 PsA patients with clinically evident psoriasis and 38 PsA patients sine psoriase, fulfilling the CASPAR criteria,54 leptin was associated with female gender and body mass index (BMI), and a close association between resistin and IL-6 was found in PsA with clinically evident psoriasis, whereas a positive association between leptin levels and BMI and C reactive protein (CRP) was found in PsA sine psoriase patients.
Considering extrinsic factors, several environmental factors were found to be associated with PsA in different studies: upper respiratory tract streptococcal infection, physical trauma, rubella vaccination, oral ulcers, occupations that involve lifting weights, obesity, mechanical stress and trauma.51 55 56 Smoking was shown to be protective in one study.56
Areas of differences and similarities in the genetic susceptibility between pSpA and PsA sine psoriase were presented in figure 1. Many areas of unmet research needs, particularly in the physiopathological pathways of pSpA are highlighted.

Genetic susceptibility and physiopathology in peripheral spondyloarthritis and psoriatic arthritis sine psoriase: differences, similarities and areas of research needs. DIP, distal interphalangeal.
Classification criteria: ASAS pSpA and CASPAR criteria
The first criteria that addressed SpA in general were the Amor criteria published in 199057 and the European Spondyloarthritis Study Group (ESSG) published in 1991.58 The Amor criteria were based on a points system, including a list of suggestive clinical, radiologic and laboratory features. Each feature contributed with 1–3 points to the total score, and a score of ≥6 points classified a patient as having SpA. The ESSG criteria focused on two entry criteria (inflammatory back pain (IBP) and asymmetrical oligoarthritis) and required at least one clinical or radiological criterion. Both the Amor and the ESSG criteria performed similarly in terms of sensitivity (88.5% and 86.6%, respectively) and specificity (91.9% and 91.1%)59 but lacked specificity when applied to patients at an early disease stage.60
At that time, only the subsequent appearance of skin or nail psoriasis could establish the diagnosis of PsA sine psoriase retrospectively. However, in 2006, the CASPAR criteria were published, having a sensitivity of 91.4% and a specificity of 98.7% for PsA8 and surpassing the performance of the previous classification for PsA.37 61 In addition, a patient can fulfil the CASPAR criteria without the presence of skin psoriasis; therefore, patients could be classified as having PsA sine psoriase when having articular clinical manifestations and a family history of psoriasis in first or second-degree relatives, or even without a family history of psoriasis (ie, in patients with dactylitis, negative rheumatoid factor and radiological evidence of juxta-articular new bone formation). The CASPAR criteria have proven to be also sensitive in early PsA.56
Thereafter, ASAS established the classification criteria for axSpA in 20099 and for pSpA in 2011.2 The performance of these classification criteria was excellent both in axSpA (sensitivity 82.9%, specificity 84.4%) and in pSpA (sensitivity 77.8%, specificity 82.9%). Furthermore, while tested prospectively in the ASAS cohort, the ASAS pSpA criteria also showed a high positive predictive value (89.5%) for pSpA as diagnosed by the rheumatologist after a 4-year follow-up.62 Moreover, a systematic literature review evaluated the performance of the ASAS criteria in 9 studies with 5739 patients with SpA62 and showed a high pooled specificity (87%) but a lower sensitivity (63%) of the ASAS pSpA criteria and a positive likelihood ratio of 4.7.
Overlap between the ASAS pSpA and the CASPAR classification criteria
Patients with peripheral musculoskeletal disease (arthritis, or enthesitis, or dactylitis) with and without skin psoriasis may fulfil both CASPAR and ASAS pSpA classification criteria systems (figure 2). For example, in the absence of psoriasis, according to the CASPAR criteria, patients can be classified as having PsA sine psoriase if they have arthritis or enthesitis or inflammatory spine disease plus three of the following: family history psoriasis, dactylitis, negative rheumatoid factor and juxta-articular bone formation on radiographs (the latter being a late sign of the disease). On the other hand, according to the ASAS criteria, patients can be classified as pSpA (without psoriasis) based on a wider range of features: arthritis, enthesitis or dactylitis plus one (Inflammatory Bowel Disease (IBD), preceding infection, HLA-B27, uveitis, sacroiliitis on imaging) or two (arthritis, enthesitis, dactylitis, IBP, family history of SpA) SpA features. Thus, in the absence of psoriasis, the ASAS pSpA criteria are more inclusive as they encompass extra-musculoskeletal manifestations (EMMs) as well as HLA-B27 and sacroiliitis.

Overlapping and distinctive features of the Assessment of SpondyloArthritis international Society (ASAS) peripheral spondyloarthritis criteria and the Classification Criteria for Psoriatic Arthritis (CASPAR) criteria, with and without psoriasis (sine psoriase). A patient with arthritis, dactylitis, family history of psoriasis and spondyloarthritis, and negative rheumatoid factor would fulfil both ASAS pSpA criteria and CASPAR PsA sine psoriase criteria simultaneously. PsA, psoriatic arthritis; pSpA, peripheral spondyloarthritis.
Nevertheless, although the ASAS pSpA classification criteria may be more inclusive of all SpA subtypes, some may argue that splitting this cluster of conditions may be more appropriate. Therefore, more disease-based classification criteria are still requested.11
Studies have analysed the magnitude of the overlap between the CASPAR and the ASAS pSpA criteria. For instance, the Leiden Early Arthritis Clinic cohort study63 evaluated the performance of both criteria in diagnosing pSpA and PsA using the rheumatologist’s diagnosis as the gold standard. Of the 150 patients diagnosed with PsA, 75 fulfilled both the ASAS and CASPAR criteria, 58 fulfilled the CASPAR criteria and 3 fulfilled the ASAS criteria only. However, patients having PsA sine psoriase were not evaluated. The ASAS and CASPAR criteria were found to be respectively specific for pSpA and PsA (89.8% and 95.6%, respectively); however, the ASAS criteria lacked sensitivity for both PsA and pSpA (52% and 48.7%, respectively), whereas CASPAR had an 88.7% sensitivity for PsA. Nevertheless, this finding was attributed to the fact that patients included in this cohort were manifesting early signs of arthritis, whereas other cohorts included other features such as dactylitis and enthesitis and other pSpA features with a longer course of disease. Although the potential of overlap might be slightly insufficient to consider pSpA and PsA as one entity, one must consider that patients enrolled in this study presented early symptoms of arthritis; therefore, a longer disease course may potentialise this overlap.
Also, the performance of the different sets of criteria was evaluated in the multinational COMOSPA study that comprised 3942 patients diagnosed by the rheumatologist.64 Although the performance status of ASAS and CASPAR criteria might not be reliable since most patients presented with symptoms of axSpA, the potential of overlap between both sets of criteria was significant. In fact, 12.3% of the cohort fulfilled the ASAS pSpA criteria, and 21.6% fulfilled the CASPAR criteria. Also, 62% of patients satisfying the ASAS pSpA criteria fulfilled the CASPAR criteria simultaneously. The authors concluded that by satisfying multiple sets of criteria, the cohesion of the SpA group is maintained and that most rheumatologists worldwide picture SpA as a unique entity of similar conditions.
In another study including 100 patients attending a psoriasis dermatology clinic,65 17% of the patients fulfilled both CASPAR and ASAS pSpA classification criteria. The duration of psoriasis and the prevalence of nail involvement (88% vs 49%) were higher in patients who met CASPAR criteria compared with those without arthritis.
Although classification criteria are helpful to better characterise diseases after clinical diagnosis, the distinction between pSpA and PsA sine psoriase based on these criteria may be viewed as artificial, because of a potential circular analysis bias. In the absence of an appropriate biomarker for either disease, we are compelled to use the imperfect classification criteria, which may be validated against the physician’s opinion (diagnosis), the current gold standard to define a disease. Nevertheless, these classification criteria need to be validated in large and diverse cohorts whenever this is possible. Ultimately, it should always be highlighted that any classification criteria, although providing a framework for the identification of individual patients, should be differentiated from diagnostic criteria to avoid misdiagnosis and subsequent overtreatment.10 Diagnostic criteria for pSpA and PsA have not been validated. The classification criteria define the diseases for the purpose of enrolling patients in clinical trials and provide guidance to clinicians, yet the definitive diagnosis should be based on the rheumatologist’s evaluation.
Disease phenotype and burden
Disease phenotype
To date, the diagnosis of pSpA and PsA is essentially clinical.10 In pSpA, peripheral arthritis is found in 79%–98% of the cases, followed by enthesitis in 41%–63% and dactylitis in 12%–49%.5 17 18 22 Conversely, arthritis was found in 85.7% of PsA,5 and dactylitis was a more prominent feature in PsA sine psoriase with a prevalence of 62%, compared with enthesitis, which was found less frequently in 35% (table 1 and figure 3).39

{kind=link}
{kind=link}
{kind=link}
Prevalence of spondyloarthritis features in peripheral spondyloarthritis and psoriatic arthritis sine psoriase: differences and similarities. DIP, distal inter-phalangeal joints; IBD, inflammatory bowel diseases; IBP, inflammatory back pain; LL, lower limbs; N/A, not applicable.
The type of joints involved is different between pSpA, where the articular topography mostly involves mainly the large joints of the lower limbs in more than half of the cases.5 66 whereas the DIP joints of the hands are primarily affected in PsA sine psoriase in 40%–71%.38 39
As for the number of involved joints, oligoarthritis was found in 45% of patients with pSpA and 40% with PsA sine psoriase, whereas polyarthritis was found in 44% of patients with pSpA and 35% of patients with PsA sine psoriase.5 39
Axial involvement was found in 12%–55% of patients with pSpA,4 5 18 including 30%–35% with sacroiliitis on MRI and in 12%–35% in patients with PsA sine psoriase.39 67
Finally, HLA-B27 was found in 27%–62% of patients with pSpA,5 17–19 whereas it was rarely found in PsA sine psoriase and was negatively associated with the family history of psoriasis.38
Importantly, according to Olivieri et al,37 PsA sine psoriase is clinically identified by dactylitis and/or DIP arthritis, HLA-Cw6, and a family history of psoriasis. Furthermore, the nail examination should always be performed, since in patients with PsA sine psoriase, the nail changes occurred before the onset of clinically apparent psoriasis in 88% of the PsA patients.28 31
Extra-musculoskeletal manifestations
Anterior uveitis (AU) was found in 1.2%–20.3% of patients with pSpA, significantly more frequently in HLA-B27-positive subjects.5 17–19 22 The estimated prevalence of AU in PsA is 2%–25%.39 68 In a cohort of 372 patients having SpA, AU was associated with enthesitis but negatively associated with both PsA and dactylitis.69 AU may precede the clinical features of SpA, may be present at diagnosis or may complicate the SpA clinical course66 (table 1), and its variable prevalence may be due to different classification criteria and lengths of follow-up used in the different studies.
Other less frequent eye manifestations can also occur in PsA, such as dry eye syndrome and retinal microvascular abnormalities. However, these symptoms may be attributed to the presence of skin psoriasis.70 Therefore, to determine whether the presence of such symptoms is related to skin manifestations, a subset of patients having PsA sine psoriasis were evaluated. The results showed the presence of dry eye syndrome and subclinical abnormalities in visual function in PsA sine psoriasis. Furthermore, the patients included had moderately to severe disease activity index, which attributes these eye symptoms to systemic inflammation.71
IBD were found in 4%–17% of patients with pSpA.17–19 22
Disease burden
Data on pSpA found a median Patient Global Assessment score of 38–45 mm, a mean tender joint score of 1–3.3, a mean swollen joint score of 1–1.2,5 17 18 a mean Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) of 3.5–4, Ankylosing Spondylitis Disease Activity Score - C Reactive Protein (ASDAS-CRP) of 2.3–2.6 and Bath Ankylosing Spondylitis Functional Index (BASFI) of 1.7. In pSpA patients, 21% had a temporary disability to work. The disease burden in PsA sine psoriase is poorly explored and cannot be extrapolated from PsA, since the presence of skin lesions might contribute to the general burden of disease. However, in all cases where pSpA was combined with axial manifestations or with PsA, patients had a higher disease activity and higher scores in all patient-reported outcomes compared with the purely axial pSpA patients.18 22 From the perspective of inflammatory burden, inflammatory markers seem to be slightly higher in PsA sine psoriase (mean erythrocyte sedimentation rate (ESR) 36 mm/hour) compared with pSpA (mean ESR 7.5–18 mm).6 17 19 39
Therapeutic guidelines
Specific treatment guidelines for pSpA are scarce, given the poorly defined nature of the disease, the lack of validated outcome measures and dedicated clinical trials in this indication (table 2). The treatment of pSpA was addressed in a section of the ASAS-European League of Associations for Rheumatology (EULAR) management recommendations for axSpA published in 2017, with an update expected in 2022.72 The current ASAS-EULAR recommendations advise beginning a course of non-steroidal anti-inflammatory drugs (NSAIDs) as a first-line agent, taking risks and benefits into account. Local corticosteroids injections are recommended as well. In case of failure of this initial strategy, conventional synthetic disease-modifying antirheumatic drugs (cs-DMARDs), namely sulfasalazine, are proposed. In patients with persistently high disease activity despite these conventional treatments, biological DMARDs (b-DMARDs), such as tumour necrosis factor alpha inhibitors (TNFi) or interleukin (IL)-17 should be considered.
Treatment recommendations for peripheral spondyloarthritis and psoriatic arthritis
In 2021, specific guidelines for pSpA were published by the National Institute for Health and Care Excellence (NICE).73 The NICE guidelines also recommend starting with conventional non-biological therapy, with NSAIDs or corticosteroids injections (local or intramuscular) as adjunct therapies to manage symptoms. A trial of two cs-DMARDs is recommended before stepping up therapy. In case of failure, several options were proposed, but no explicit algorithm was suggested. Apremilast (a phosphodiesterase 4 inhibitor) and TNFi are proposed in case pSpA was still active after the failure of conventional therapy, that is, more than three tender and swollen joints. IL17i, Ustekinumab (an IL12/23 inhibitor) and Janus Kinase inhibitors were recommended as third-line therapy after failure of at least one b-DMARD. Guselkumab (an IL23 inhibitor) was recommended as a third-line therapy for active pSpA and at least one b-DMARD failure.
Regarding PsA sine psoriase, an extrapolation from the PsA treatment guidelines can be proposed,15 although the presence of absence of psoriasis may sensibly impact the outcome of a specific therapy. PsA is also considered by some as the prototype of pSpA, and extrapolations from PsA to pSpA treatment are observed in real-world studies.5
The worldwide approval of several biological treatments in the PsA indications are based on randomised controlled trials, whereas biological treatments are off label for patients with non-psoriatic pSpA.
The American College of Rheumatology, EULAR and GRAPPA developed recent management guidelines for PsA,15 74 75 based on the dramatic increase in treatment options.
The GRAPPA recommendation is based on the different domains (including arthritis, enthesitis and dactylitis) to provide treatment choices for PsA.15 The EULAR management recommendations for PsA has a sequential approach focusing on peripheral arthritis, suggesting the order in which drugs should be prescribed. In patients with active disease despite NSAIDs and local injections, a classical step-up treatment schedule is proposed with cs-DMARDs, followed by a b-DMARD, such as a TNFi or a biological targeting IL-12/–23 or IL-17, or a targeted synthetic DMARD (ts-DMARD).
There are only a few RCTs, all involving TNFi,3 4 76 77 which provide some evidence although insufficient for regulatory approval for pSpA treatment.10 As a consequence, the use of TNFi in non-psoriatic PsA is considered ‘off label’ by regulatory agencies worldwide, extrapolated from PsA treatment algorithms, unless patients also have active axSpA or active IBD, which are among the Food and Drug Administration (FDA)-approved and European Medicines Agency-approved indications for these agents. These regulatory factors clearly limit the management of patients with pSpA and PsA sine psoriase.
Areas of future research
While considering differences and similarities between pSpA and PsA sine psoriase, this review identified areas of unmet research needs.
First, the genetic susceptibility of the diseases should be investigated as it would provide insights for the correct definition.
Second, exploring the physiopathological pathways of both diseases in parallel could help identifying patterns of similarities or differences.
Third, the classification criteria of both diseases should be validated in diverse cohorts from different ethnicities and geographical regions. Ideally, the cohorts should have a follow-up that is long enough to differentiate between the patients who develop psoriasis many years after the onset of PsA and those who never develop psoriasis during their lifetime. Future cohorts should also address the heterogeneous nature of PsA (symmetrical polyarthritis, oligoarthritis, axial PsA, etc).
Future research may benefit from artificial intelligence technologies, which have already started to be applied in axSpA and general PsA,78 79 although with some methodological and ethical limitations.
Finally, conducting dedicated pharmacological clinical trials in these specific populations, although limited by the potential low sample sizes, may provide insightful hints, as sometimes going from bench to bedside would help us reach better definitions of the diseases.
Conclusions
pSpA appears to be a more inclusive term compared with PsA sine psoriase. In theory, more patients can be classified as having pSpA (according to the currently existing criteria) than PsA sine psoriase, since the former may also include EMMs, HLA-B27 and sacroiliitis. In practice, this is also translated by the prevalence derived from epidemiological studies, independent of whether they are based on classification criteria or rheumatologist-based diagnosis.
Areas of similarities between both entities include the age of onset, number of joints involved and prevalence of axial involvement. However, some areas of differences were also identified based on the reported prevalence, as patients with pSpA have a male gender predominance, higher prevalence of enthesitis and involvement of large joints of the lower limbs, whereas patients with PsA sine psoriase have a higher prevalence of dactylitis and involvement of hand DIPs.
On the other hand, the presence of peripheral manifestations on top of any SpA subset was associated with a higher disease burden. In addition, the same general treatment algorithm may apply regarding therapy: starting with NSAIDs, stepping up to cs-DMARDs, then to b-DMARDs or ts-DMARDs. The characterisation of both disease entities is limited by the scarcity of dedicated studies, particularly the poor characterisation of the genetic susceptibility and physiopathological patterns and by the lack of appropriate biomarker. Moreover, classification may be hindered by a circular analysis bias.
In conclusion, based on the available data and taking into account the potential risk of circular analysis bias, the difference between pSpA and PsA sine psoriase appears to go beyond semantics. Despite many similarities, the few differences at the epidemiological, genotypic and phenotypic levels should drive scientific efforts to reach a better characterisation of pSpA as an individual disease. Accordingly, randomised clinical trials should target patients with a well-defined pSpA to identify effective therapies in this population.
Ethics statements
Patient consent for publication
References
Footnotes
Twitter @nellziade
Contributors XB and NZ designed the concept of the review. MBA and NZ performed the literature search and drafted the manuscript. All the authors made substantial contributions to the design of the work, the interpretation of the studies, the draft and the revision of the manuscript.
Funding We acknowledge support by the Open Access Publication Funds of the Ruhr-Universität Bochum.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.