Article Text

Abstract
Objectives Remote assessment of patients with rheumatoid arthritis (RA) has increased during recent years. However, telematic consultations preclude the possibility of carrying out a physical examination and obtaining objective inflammation. In this study, we developed and validated two novel composite disease activity indexes (Thermographic Disease Activity Index (ThermoDAI) and ThermoDAI-CRP) based on thermography of hands and machine learning, in order to assess disease activity easily, rapidly and without formal joint counts.
Methods ThermoDAI was developed as the sum of Thermographic Joint Inflammation Score (ThermoJIS), a novel joint inflammation score based on the analysis of thermal images of the hands by machine learning, the Patient Global Assessment (PGA) and, for ThermoDAI-CRP, the C reactive protein (CRP). Construct validity was tested in 146 patients with RA by using Spearman’s correlation with ultrasound-determined grey-scale synovial hypertrophy (GS) and power Doppler (PD) scores, CDAI, SDAI and DAS28-CRP.
Results Correlations of ultrasound scores with ThermoDAI (GS=0.52; PD=0.56) and ThermoDAI-CRP (GS=0.58; PD=0.61) were moderate to strong, while the correlations of ultrasound scores with PGA (GS=0.35; PD=0.39) and PGA+CRP (GS=0.44; PD=0.46) were weak to moderate. ThermoDAI and ThermoDAI-CRP also showed strong correlations with Clinical Disease Activity Index (ρ>0.83), Simplified Disease Activity Index (ρ>0.85) and Disease Activity Score with 28-Joint Counts-CRP (ρ>0.81) and high sensitivity for detecting active synovitis using remission criteria.
Conclusions ThermoDAI and ThermoDAI-CRP showed stronger correlations with ultrasound-determined synovitis than PGA and PGA + CRP, thus presenting an opportunity to improve remote consultations with patients with RA.
- arthritis, rheumatoid
- outcome assessment, health care
- inflammation
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Remote assessment of patients with rheumatoid arthritis precludes the possibility of conducting a physical examination, making the determination of objective inflammation challenging.
Previous research shows that Thermographic Joint Inflammation Score (ThermoJIS), a novel joint inflammation score based on the computational analysis of thermal images of the hands by machine learning, assesses joint inflammation in patients with rheumatoid arthritis in a rapid, sensitive and automated manner.
WHAT THIS STUDY ADDS
The development and validation of Thermographic Disease Activity Index (ThermoDAI) and ThermoDAI-CRP, two novel composite disease-activity indexes based on ThermoJIS, the Patient Global Assessment and C reactive protein to assess disease activity without the need for formal joint counts.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
ThermoDAI and ThermoDAI-CRP constitute a fast, easy and accurate method for assessing disease activity remotely.
These novel indexes could be used not only to improve clinical practice, but also to decentralised clinical trials.
Introduction
Rheumatoid arthritis (RA) is an inflammatory disease characterised by chronic synovitis, joint destruction and disability. Current therapies, the implementation of treat-to-target strategies and tight control assessments have all been shown to aid improved outcomes.1 2 Different disease activity measurement tools are used in clinical practice and trials. Disease Activity Score with 28-Joint Counts (DAS28), Clinical Disease Activity Index (CDAI) and Simplified Disease Activity Index (SDAI) involve formal joint counts performed by trained professionals, as well as Patient Global Assessment (PGA) of health and laboratory assessment.3 4
Recently, digital innovations in rheumatology have increased exponentially and the use of telemedicine to follow-up of patients with RA has been explored.5–7 As telematic consultations do not allow for the possibility of making formal joint counts, the development of new techniques enabling rheumatologists to obtain objective inflammation in a fast and easy manner could improve remote evaluation of patients with RA .
Thermography is an emerging imaging technique that creates an image of the heat emitted by bodies by capturing the intensity of long wave infrared radiation, which increases with temperature.8 9 In recent years, a new generation of affordable uncooled thermal detectors has been developed. These thermal cameras are compact, easy to use and have shown good performance suitable for medical imaging.10 As inflammatory processes cause warmth and localised hyperaemia, thermography could be useful for detecting arthritis and disease activity. Previous research (both preclinical and clinical) showed thermographically detectable changes in inflamed joints.11–14 Furthermore, we recently developed a novel Thermographic Joint Inflammation Score (ThermoJIS) based on the computational analysis of thermal images of the hands by machine learning to assess joint inflammation in an automated and rapid manner.15
The aim of this study was to develop and validate two new composite disease activity indexes (Thermographic Disease Activity Index (ThermoDAI) and ThermoDAI-CRP) based on ThermoJIS, patient global health assessment and C reactive protein (CRP) levels.
Methods
Patients
The study population was comprised of 146 patients with RA recruited for the validation set of our previous ThermoJIS study.15 A diagram showing the flow of the participants is reported in online supplemental figure S1. Exclusion criteria were as follows: patients less than 18 years of age, subjects with wounds, infections or trauma on the dorsal side of the hands, and those using bandages, cosmetics or other substances that could affect the thermal pattern prior to data collection. The study complied with the Declaration of Helsinki.
Supplemental material
Thermography
For all patients, a thermographic image of the hands was taken using a Thermal Expert TE-Q1 camera with a 6.8 mm lens. Thermal cameras were connected to a smartphone, and a custom mobile app was developed to acquire the raw thermal images (ie, infrared wave intensity). Thermography was performed at outpatient visits prior to ultrasound and physical examination and without an acclimatisation process or controlled room temperature in order to reproduce real-world conditions. The dorsal images of both hands were recorded with the fingers spread. No fixed distance between the camera and the hand was required. The researcher was instructed to frame and focus the image. All thermal images were analysed using the Singularity Biomed in-house software to obtain the ThermoJIS values, which were calculated as follows: first, the images were processed for contrast enhancement, background removal and noise reduction. Subsequently, a collection of local thermal features containing distinctive patterns of inflammation was extracted. Finally, an algorithm based on machine learning was used to analyse the features and obtain the ThermoJIS value. The higher the ThermoJIS value, the greater the confidence of having active synovitis.
Ultrasonography
Ultrasonography of both hands was performed in all patients and was used as a reference standard for the detection and quantification of synovitis. Ultrasound was performed using a GE Logiq 9 with a 9–14 MHz linear array transducer (Milwaukee, Wisconsin, USA). Both the patient and the probe were positioned according to EULAR guidelines.16 All participants underwent an ultrasound assessment (blinded with respect to other study results) consisting of a systematic examination of the wrist, metacarpophalangeal and proximal interphalangeal joints of both hands. Each joint was scored using the Outcome Measures in Rheumatology (OMERACT)-EULAR semiquantitative scoring system (0–3) for grey-scale synovial hypertrophy (GS) and for power Doppler (PD).17 18 At the patient level, an ultrasound sum score of the joints explored was made for GS (GS sum score) and PD (PD sum score). Patients with a GS sum score grade >1 and PD sum score >0 were considered to have active synovitis.
Clinical and laboratory assessments
Clinical and laboratory assessments were performed and included the number of swollen and tender joints in the standard 28-joint count examination in an ungraded fashion (SJC28 and TJC28), the PGA and the Evaluator Global Assessment (EGA) of disease activity based on a visual analogue scale score (0–10), the erythrocyte sedimentation rate and the CRP value.
Calculation of ThermoDAI and ThermoDAI-CRP
ThermoDAI and ThermoDAI-CRP were developed based on the CDAI and SDAI with the aim of being intuitive, simple and available in a remote setting. Calculations of ThermoDAI and ThermoDAI-CRP are the simple linear sum of the outcome parameters: ThermoJIS, PGA and, for ThermoDAI-CRP, the CRP in mg/dL. Thus, the formulas for ThermoDAI and ThermoDAI are as follows:


ThermoJIS values and CRP (mg/dL) were limited from 0 to 10. Therefore, ThermoDAI and ThemoDAI-CRP ranged from 0 to 20 and from 0 to 30, respectively.
ThermoDAI and ThermoDAI-CRP thresholds for remission, low disease activity (LDA) and high disease activity (HDA) were optimised to maximise weighted kappa coefficients with CDAI and SDAI, respectively (ie, different cut-off points were tested and those with the best weighted kappa with the qualitative interpretation of the CDAI and SDAI were selected).
Statistical analysis
Subject characteristics were described using means with SD, medians with IQRs or frequencies with proportions, where appropriate. The number of participants exceeded the sample size in order to obtain robust results. The study population was independent from the development set used to develop ThermoJIS to prevent overfitting. The correlations were calculated using Spearman’s correlation coefficient. Agreements of ThermoDAI and ThermoDAI-CRP with CDAI and SDAI, respectively, were determined using weighted kappa coefficients. Statistical significance was set at p<0.05 (two-sided). The statistical analysis was performed using Python V.3.7, NumPy V.1.19, Scikit-learn V.0.24 and SciPy V.1.4.
Results
Characteristics
All subjects tolerated the procedure well, and no adverse effects were observed. Characteristics of the patients are presented in table 1. The distribution of ThermoJIS is shown in online supplemental figure S2.
Characteristics of the study population
Associations between ThermoDAI and ThermoDAI-CRP with ultrasound
The Spearman’s correlation for the different indices and the ultrasound scores are shown in table 2. The PGA showed a weak correlation with the ultrasound scores. The sum of CRP to PGA only showed a small improvement. ThermoDAI showed a moderate correlation, and the ThermoDAI-CRP showed a strong correlation with the PD sum score. Both ThermoDAI and ThermoDAI-CRP showed a higher correlation than ThermoJIS. ThermoJIS correlation with TJC28 + SJC28 + EGA was 0.37 (p<0.001) (online supplemental figure S3).
Correlation between different indices and ultrasound scores
Associations between ThermoDAI and ThermoDAI-CRP with common indices used in clinical practice
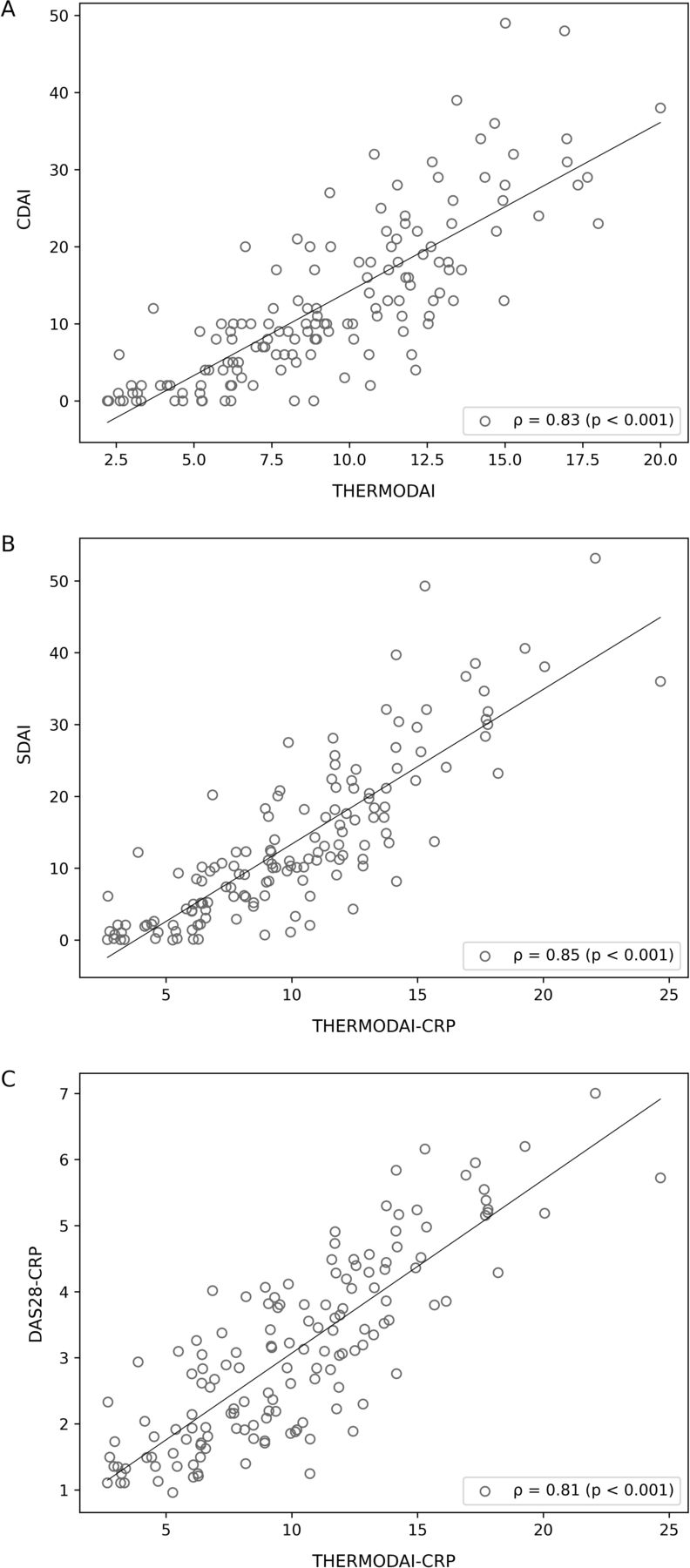
ThermoDAI and ThermoDAI-CRP showed a strong correlation with CDAI (ρ=83; p<0.001) and SDAI (ρ=0.85; p<0.001), respectively (figure 1A,B). The correlation of ThermoDAI-CRP with DAS28-CRP (ρ=0.81; p<0.001) was also strong (figure 1C).
{kind=link}
Association between the ThermoJIS and common indices used in clinical practice. (A) Correlation between the ThermoDAI and CDAI; (B) correlation between the ThermoDAI-CRP and SDAI; (C) correlation between the ThermoDAI-CRP and DAS28-CRP. CDAI, Clinical Disease Activity Index; CRP, C reactive protein; DAS28, Disease Activity Score with 28-Joint Counts; SDAI, Simplified Disease Activity Index; ThermoDAI, Thermographic Disease Activity Index; ThermoJIS, Thermographic Joint Inflammation Score.
Discrimination assessments of ThermoDAI and ThermoDAI-CRP
Optimal thresholds for remission, LDA and HDA were 5.3, 10.3 and 13.2 for ThermoDAI and 6.4, 10.9, 14.1 for ThermoDAI-CRP. Weighted kappa coefficients of ThermoDAI and ThermoDAI-CRP with CDAI and SDAI were both 0.73.
The sensitivity for detecting active synovitis using the remission thresholds was 88% for CDAI, 88% for SDAI, 81% for DAS28-CRP, 96% for ThermoDAI and 88% for ThermoDAI-CRP. The specificity was 29% for CDAI, 30% for SDAI, 65% for DAS28-CRP, 30% for ThermoDAI and 35% for ThermoDAI-CRP.
Discussion
In this study, we have characterised ThermoDAI and ThermoDAI-CRP, two novel disease activity indexes based on the analysis of thermal images of hands by machine learning (ThermoJIS), the PGA and the CRP. ThermoDAI has been developed to be intuitive and simple to use (linear sum of the components). ThermoDAI-CRP can be easily calculated from ThermoDAI by summing the CRP.
ThermoDAI and ThermoDAI-CRP showed higher correlations with ultrasound scores than PGA or PGA + CRP. ThermoDAI-CRP even showed a strong correlation with PD, similar to common indices used in clinical practice. These findings suggest that ThermoJIS, PGA and CRP are synergic and can overcome the correlations of the individual components, thereby providing an accurate evaluation of synovitis. Furthermore, ThermoDAI and ThermoDAI-CRP showed strong correlations with CDAI, SDAI and DAS28-CRP.
In 2011 the American College of Rheumatology, the EULAR and the OMERACT groups published the most influential and authoritative definitions of remission: the Boolean-based and SDAI index-based definitions, which are considered to be stringent.19 The selected remission criteria of ThermoDAI and ThermoDAI-CRP were at least as stringent as SDAI for detecting active synovitis.
All of these properties make these novel indexes promising for assessing disease activity remotely, especially when physical examinations are not possible. However, this study is cross-sectional in nature. Therefore, longitudinal studies involving a new cohort of patients with RA are needed to validate sensitivity-to-change and to determine treatment response thresholds before applying them for patient follow-up.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by (1) Name: CEIm del Hospital Universitari de Bellvitge ID: PR307/19 and AC044/16.(2) Name: Comissió de Recerca del CSA ID: PR8/2019. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
The authors thank the Spanish Foundation of Rheumatology for providing medical writing/editorial assistance during the preparation of the manuscript (FERBT2022). We are also grateful to the patients for their participation.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors IM-I and MAM-L conceived and designed the study. IM-I, CM and JAN acquired the data. IM-I and MAM-L analysed the data, interpreted the results and drafted the manuscript. JN, CG-V and JMN provided critical comments on the design and results. All the authors revised and approved the final version of the manuscript. IM-I is the guarantor for this paper.
Funding This study was funded Singularity Biomed, Sant Cugat del Vallès, Spain.
Competing interests IM-I and MAM-L are cofounders and shareholders of Singularity Biomed.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.