Article Text

Abstract
Objectives This study aimed to evaluate the Disease Activity index for PSoriatic Arthritis (DAPSA) based on a quick quantitative C reactive protein (qCRP) assay (Q-DAPSA) in a multicentre, prospective, cross-sectional study in patients with psoriatic arthritis (PsA).
Methods The assessment of prospectively recruited study patients included joint examination and patient reported outcome (PRO) measures (patient global assessment, patient pain assessment). Following, the DAPSA based on a routine laboratory CRP measurement, Q-DAPSA and clinical DAPSA (cDAPSA) were calculated. Cross-tabulations and weighted Cohen’s kappa were performed to analyse the agreement of disease activity categories. Bland-Altman plots and intraclass correlation coefficients were used to determine the agreement of numerical values regarding CRP and qCRP as well as different disease activity scores.
Results Altogether, 104 patients with PsA could be included in the statistical analysis. With Q-DAPSA, 102 of 104 (98.1%) patients achieved identical disease activity categories in comparison to DAPSA with a weighted Cohen’s kappa of 0.980 (95% CI: 0.952 to 1.000). The agreement between DAPSA and cDAPSA was slightly lower with identical disease activity categories seen in 97 of 104 (93.3%) of patients and with a weighted Cohen’s kappa of 0.932 (95% CI 0.885 to 0.980).
Conclusions The Q-DAPSA showed an almost perfect agreement with the conventional DAPSA regarding identical disease activity categories. Thus, the Q-DAPSA can be used as a timely available disease activity score in patients with PsA with the additional benefit of CRP involvement. Consequently, the Q-DAPSA could facilitate the implementation of the treat-to-target concept in clinical routine and clinical trials.
- Psoriatic Arthritis
- Disease Activity
- Patient Reported Outcome Measures
Data availability statement
Data are available upon reasonable request. De-identified participant data can be made available after approval of a written request for scientific purposes by the corresponding author.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ABOUT THIS SUBJECT?
The Disease Activity index for PSoriatic Arthritis (DAPSA) is one of the preferred tools for disease activity assessment in patients with psoriatic arthritis (PsA) as a part of a treat-to-target (T2T) concept.
WHAT DOES THIS STUDY ADD?
The current study evaluated the DAPSA using a quick quantitative C reactive protein (CRP) assay (Q-DAPSA) in a prospective, multicentre, cross-sectional PsA cohort.
HOW MIGHT THIS IMPACT ON CLINICAL PRACTICE OR FUTURE DEVELOPMENTS?
Due to its immediate availability with the inclusion of an acute phase parameter (CRP), the Q-DAPSA can be used for regular disease activity monitoring and may ease the application of a T2T concept in patients with PsA.
Introduction
Psoriatic arthritis (PsA) is a multifaceted autoimmune disease presenting with arthritis, enthesitis, dactylitis, axial manifestations as well as skin and nail involvement to varying degrees.1
The clinical heterogenity of PsA is reflected by the great extent of composite indices to measure disease activity in patients with PsA.2 Currently, there is an ongoing debate which of these disease activity indices should be used preferably and whether several unidimensional scores, each covering one PsA disease domain, or one multidimensional score encompassing multiple domains should be favoured for disease activity monitoring.3
Regular disease activity evaluation using validated disease activity scores and subsequent modification of medical therapy to reach a predefined therapeutic target is summarised under the term of the ‘treat-to-target’ (T2T) concept.4 Implementing a T2T approach in patients with PsA has shown several advantages compared with routine care, including reduced disease activity concerning joint and skin disease as well as improved quality of life.5 International T2T guidelines do not provide a clear recommendation for one disease activity score to guide therapeutic decisions in patients with PsA but state the Disease Activity index for PSoriatic Arthritis (DAPSA) or Minimal Disease Activity criteria as preferred options.3 Another well-validated composite index is the Psoriatic Arthritis Disease Activity Score (PASDAS),6 which has shown a close relationship with various patient reported outcome (PRO) measures.7
The DAPSA is a continuous composite index focusing on joint involvement in PsA.8 9 It encompasses swollen joint count (SJC) out of 66 joints, tender joint count out of 68 joints, patient global assessment on a visual analogue scale (VAS) ranging from 0 to 10 cm, patient pain assessment on a VAS ranging from 0 to 10 cm and C reactive protein (CRP) in mg/dL.8–10 Since CRP determination is accompanied by a time delay, a clinical DAPSA (cDAPSA) was proposed for the outpatient setting.9 10 The cDAPSA consists of the same parameters as the conventional DAPSA but omits CRP values9 10 and thus enables immediate assessment of disease activity without a time delay while waiting for CRP results. Moreover, the cDAPSA has shown a high agreement with DAPSA in different datasets.11 12
However, the T2T recommendations for axial and peripheral spondyloarthritis (SpA) have stated that clinical remission should comprise the remission of significant signs and symptoms as well as normalisation of acute phase reactants like CRP.3 The rationale for this recommendation was—among others—that elevated CRP values were shown to be an important prognostic parameter for the progression of structural damage in patients with PsA.13–15 This highlights the importance of regular assessment of CRP values and the inclusion of CRP values in disease activity scores for patients with PsA.
In other studies, we could already validate a qCRP-based Ankylosing Spondylitis Disease Activity Score (ASDAS-Q) in patients with axial SpA16 17 and a qCRP-based Simplified Disease Activity Index (SDAI-Q) in patients with rheumatoid arthritis (RA).18 In the current study, we aimed to evaluate a DAPSA using a quick quantitative CRP assay (so called Q-DAPSA). The Q-DAPSA could be beneficial for the disease activity assessment in patients with PsA due to fast clinical availability while still including the CRP as objective disease activity parameter.
Methods
Patients and assessments
This multicentre, cross-sectional pilot study was performed as part of a larger, overaching study project to evaluate the performance of different rheumatologic disease activity scores based on a qCRP assay, including a qCRP-based ASDAS17 and a qCRP-based SDAI.18
Participants were recruited between January 2020 to October 2020 from five different rheumatologic centres located in Berlin, Germany, including three rheumatologic outpatient practices and two specialised academic university hospitals. Patients were eligible for study participation if they were ≥18 years of age, had a clinical diagnosis of PsA and had given written informed consent.
Patients with signs of an acute infection or with a previously known clinically significant anaemia (haemoglobin concentration <10 g/dL or <6.2 mmol/L) were excluded from study participation.17 The clinical evaluation involved clinical parameters of DAPSA including joint counts, patient’s self-assessment of disease activity in the last 7 days (on a VAS from 0 cm=inactive to 10 cm=very active) and patient’s self-assessment of joint pain in the last 7 days (on a VAS from 0 cm=no pain to 10 cm=most severe pain).
Routine laboratory CRP was determined in several certified laboratories by a conventional method (usually, a turbidimetric assay) according to routine clinical care, while ESR and qCRP values were measured locally. For qCRP measurement, the ‘QuikRead go’ instrument (Aidian Oy, Espoo, Finland, software V.7.5.1 and 7.6.2) and the reagent kits ‘QuikRead go wrCRP+Hb’ (Aidian Oy) were used. In the majority of study participants, qCRP was measured using whole blood from the blood collection system, which would have been disposed otherwise.17 For this purpose, blood was taken from the blood collection system (this refers to the tubing system of the butterfly needle) using a microcapillary of the qCRP test. Ethylenediaminetetraacetic acid (EDTA) or heparin whole blood could be equally used for the qCRP testing, when the blood collection system was no longer available.17
The haematocrit concentration influenced the measurement range of qCRP values, for haematocrit concentrations of 40–45%, the qCRP measurement range was 0.5–200 mg/L (0.05–20 mg/dL).19 The qCRP testing is possible for samples with a haematocrit concentration between 15% and 75%.19 Studies for the validation of the ‘QuikRead go’ products were implemented according to the Clinical and Laboratory Standards Institute guidelines, EP5-A3.19 20 The qCRP measurement was implemented as described in the assay instructions19 and takes approximately 2 min.18 All qCRP values were displayed in mg/L with one decimal place by the measuring instrument.19 Quality controls using the ‘QuikRead go wrCRP Control’ (Aidian Oy) solution were conducted one time per week.17 19
The price for the qCRP testing machine is 1252.10€, and the price for the qCRP testing kits (QuikRead go wrCRP+Hb Kit) for the performance of 50 tests is 142.02€ (2.84€ per test). The control solution costs 19.00€ and lasts for several months. All prices mentioned refer to a list provided by the respective company (Aidian Oy) in September 2021.
DAPSA and Q-DAPSA were calculated according to Schoels et al9 and cDAPSA according to Schoels et al.10 For CRP or qCRP values below the lowest limit of detection, a value of 0.00 mg/dL was assumed for further calculations. To analyse the proportion of identical numerical values, values of DAPSA, Q-DAPSA and cDAPSA were rounded to one decimal place.
Patients were assigned to the following disease activity categories with DAPSA and Q-DAPSA: remission=DAPSA ≤ 4; low disease activity=DAPSA > 4 and ≤ 14; moderate disease activity=DAPSA > 14 and ≤ 28; and high disease activity=DAPSA > 28.10 Disease activity classification for cDAPSA was: remission=cDAPSA ≤ 4; low disease activity=cDAPSA > 4 and ≤ 13; moderate disease activity=cDAPSA > 13 and ≤ 27; and high disease activity=cDAPSA > 27.10
Outcomes
The primary outcome was the proportion of patients with identical disease activity category assignments by DAPSA and Q-DAPSA.
Secondary outcome measures were:
The proportion of patients with identical disease activity categories by DAPSA and cDAPSA.
The proportion of identical numerical values for DAPSA and Q-DAPSA and for DAPSA and cDAPSA.
The proportion of identical numerical values for qCRP and routine laboratory CRP.
Identical numerical values of DAPSA/Q-DAPSA/cDAPSA and CRP/qCRP were expected if the numerical values were equivalent up to the first decimal place.
Sample size
Similar to our other study,18 this is a pilot study for the evaluation of the Q-DAPSA, and, thus, we set a sample size of 100 patients with PsA.
Statistical analysis
Methods of descriptive statistics were used to analyse clinical and laboratory information, demographic data and disease activity scores. The NSAID equivalent score (modified formula according to Dougados et al21) was applied to quantify the intake of non-steroidal anti-inflammatory drugs (NSAIDs).17
NSAID equivalent score21=NSAID equivalent dose 
The agreement of disease activity categories by DAPSA and Q-DAPSA as well as DAPSA and cDAPSA was analysed using cross-tabulations and weighted Cohen’s kappa. The agreement of the numerical values by different DAPSA scores and CRP versus qCRP was evaluated with Bland-Altman plots and intraclass correlation coefficient (ICC).
ICC and the corresponding 95% CIs were calculated using a mean rating (k=2), absolute agreement, two-way mixed-effect model. Statistical analysis was performed with SPSS Statistics (IBM, Armonk, New York, V.27) and Microsoft Excel (Microsoft Corporation, Redmond, Washington, Office V.2019).17
Participants who had missing values for routine laboratory CRP or qCRP were excluded from statistical analyses.
Patient and public involvement statement
Patients and the public were not involved in the design, conduct, reporting or dissemination plans of this study.
Results
Demographic and clinical characteristics
In total, 110 patients with PsA were eligible and have given written informed consent to participate in the study. Six of these patients could not be included in the statistical analysis: One patient withdrew his written informed consent after study participation, in two patients no current routine laboratory CRP was available, two patients had a missing qCRP value due to a technical error of the qCRP testing device and in one patient no laboratory parameters were available due to non-appearance for blood sampling.
Overall, 104 PsA participants with available values of routine laboratory CRP and qCRP were included in the statistical analysis, while ESR values were available for 97 of these patients.
Table 1 and online supplemental table S1 show relevant demographic, clinical and treatment data. Mean age of the included patients was 51.2 years; mean disease duration 7.1 years and 55 (52.9%) patients were woman. Ten (9.6%) patients were treated with systemic glucocorticosteroids, 43 (41.3%) patients received NSAID therapy, 37 (35.6%) patients were treated with a conventional synthetic disease modifying anti-rheumatic drug (csDMARD), 3 (2.9%) patients were treated with a targeted synthetic DMARD (tsDMARD) and 53 (51.0%) patients received a biological DMARD (bDMARD) therapy. Elevated routine laboratory CRP values (≥ 0.5 mg/dL) were observed in 22 (21.2%) patients while routine laboratory CRP values ≥2.0 mg/dL were seen in five (4.8%) patients.
Supplemental material
Demographic, clinical, laboratory and treatment characteristics
Comparison of routine laboratory CRP and qCRP
The mean routine laboratory CRP and qCRP values were 0.52±1.39 mg/dL and 0.62±1.58 mg/dL, respectively (table 1). Identical numerical values of routine laboratory CRP and qCRP were seen in 14 of 104 (13.5%) patients. The mean difference of both CRP measurement methods was 0.10±0.41 mg/dL with differences ranging from −0.17 to 3.97 mg/dL. One patient showed a difference between CRP and qCRP>1.0 mg/dL (difference of 3.97 mg/dL). A difference of≤1.0 mg/dL and>0.5 mg/dL between both CRP values was observed in three patients (differences of 0.84 mg/dL, 0.71 mg/dL and 0.51 mg/dL).
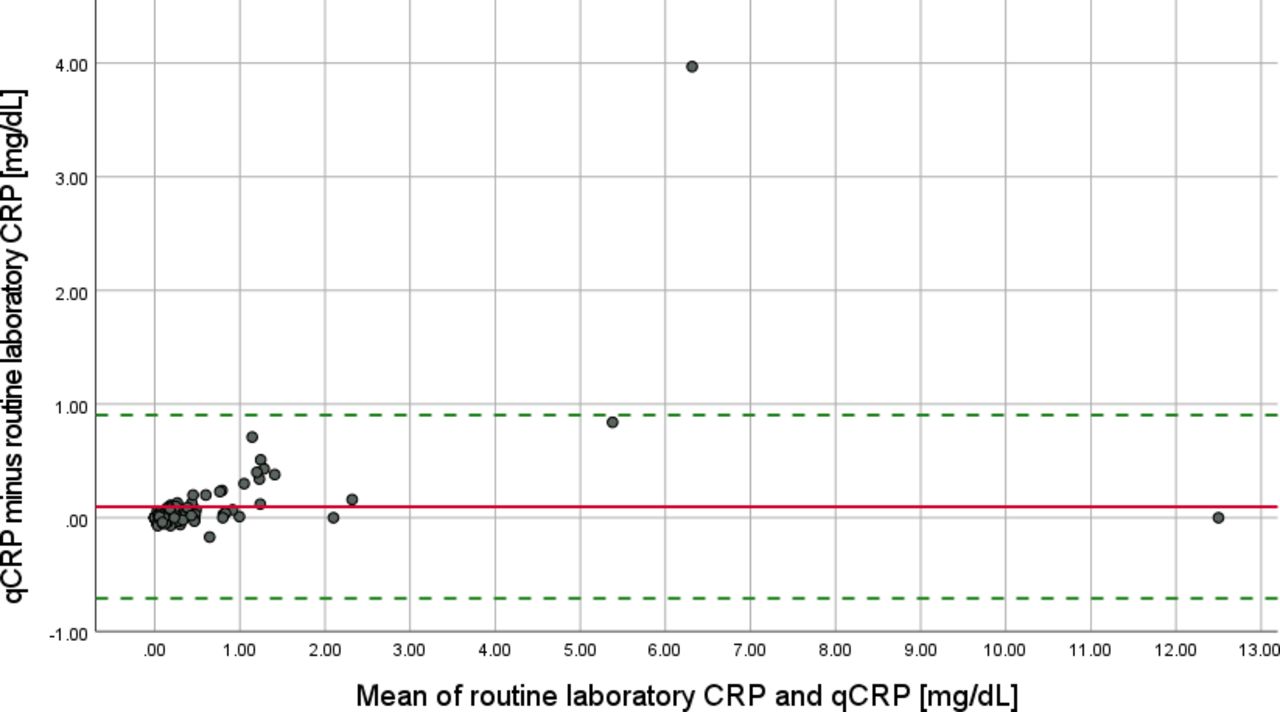
The agreement of numerical values by routine laboratory CRP and qCRP is illustrated by a Bland-Altman plot (figure 1). The 95% limits of agreement were located at −0.71 and 0.90 mg/dL . ICC for both CRP measurement methods was 0.980 (95% CI 0.969 to 0.986), shown in table 2.
ICC for different CRP measurement methods and disease activity scores

Bland-Altman plot for routine laboratory CRP and qCRP. The solid line marks the mean difference between routine laboratory CRP and qCRP (0.0973 mg/dL). The dotted lines indicate the 95% limits of agreement (−0.7083 to 0.9029 mg/dL). CRP, C reactive protein; qCRP, quick quantitative CRP.
Comparison of DAPSA, Q-DAPSA and cDAPSA
The Q-DAPSA provided identical disease activity categories as the DAPSA in 102 of 104 (98.1%) patients with a weighted Cohen’s kappa of 0.980 (95% CI 0.952 to 1.000), also shown in table 3A. The two patients with different disease activity categories both had DAPSA and Q-DAPSA values near the cutoffs of disease activity categories (patient 1: DAPSA 4.00; Q-DAPSA 4.20; patient 2: DAPSA 13.99; Q-DAPSA 14.02) (online supplemental table S2A).
(A) Disease activity categories by DAPSA versus Q-DAPSA and (B) disease activity categories by DAPSA and cDAPSA
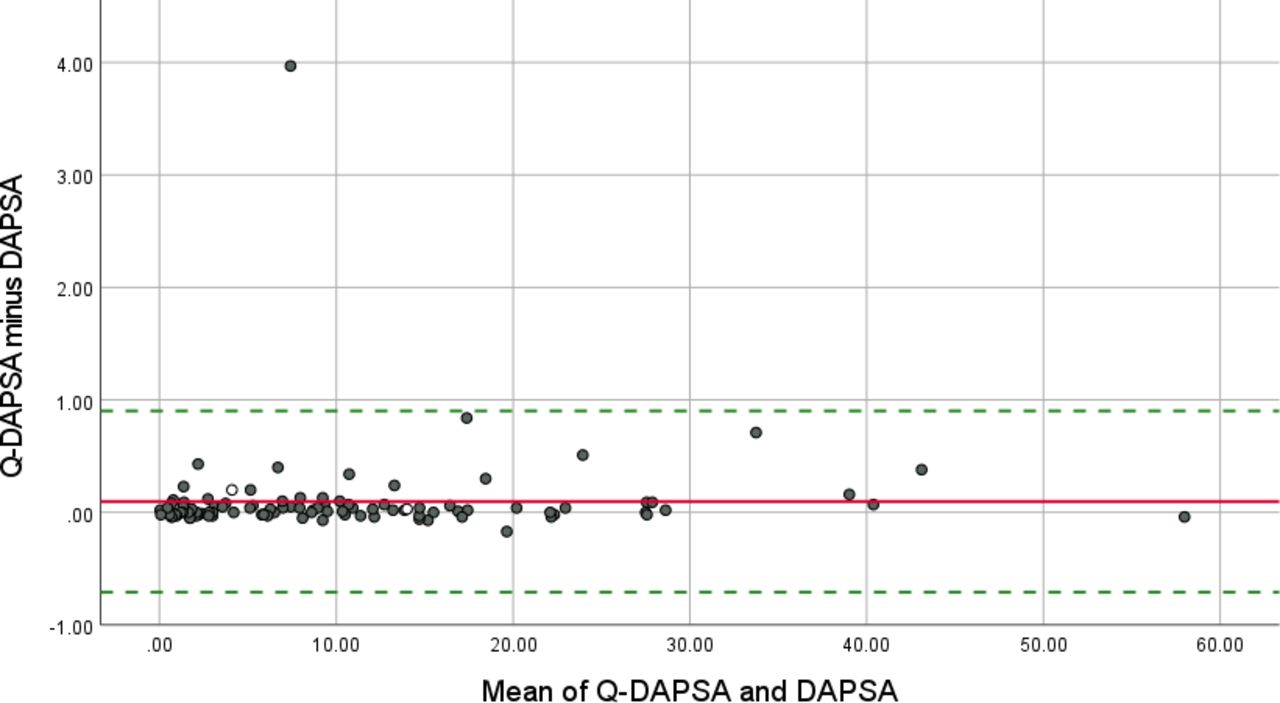
DAPSA and Q-DAPSA showed identical numerical values in 60 of 104 (57.7%) patients when values were rounded to one decimal. Mean of the differences between DAPSA and Q-DAPSA was 0.1±0.4 with differences ranging from −0.2 to 4.0. ICC for DAPSA and Q-DAPSA was 1.000 (95% CI 0.999 to 1.000) (table 2). A Bland-Altman plot illustrates the agreement of numerical values by DAPSA and Q-DAPSA (figure 2).

Bland-Altman plot for Q-DAPSA and DAPSA. Difference in disease activity category between Q-DAPSA and DAPSA: same disease activity category Higher disease activity category with Q-DAPSA (one category higher with Q-DAPSA) The solid line marks the mean difference between Q-DAPSA and DAPSA (0.097). The dotted lines indicate the 95% limits of agreement (−0.708 to 0.903). X-axis and Y-axis indicate the ‘mean of Q-DAPSA and DAPSA’ as well as ‘Q-DAPSA minus DAPSA’ in DAPSA points. DAPSA, Disease activity index for PSoriatic Arthritis; Q-DAPSA, DAPSA calculated with a quick quantitative C reactive protein assay.
Comparing DAPSA and cDAPSA, 7 of 104 (6.7%) patients were assigned to different disease activity categories (table 3B). The cDAPSA produced a higher disease activity category than the DAPSA in five of these seven patients—all of these five patients had DAPSA, Q-DAPSA and cDAPSA values close to the cutoffs of respective disease activity categories and routine laboratory CRP levels ≤0.79 mg/dL. The two patients with higher disease activity categories by DAPSA in comparison to cDAPSA showed high CRP and qCRP levels (routine laboratory CRP was 4.96 and 4.33 mg/dL, respectively) (online supplemental table S2B). Weighted Cohen’s kappa for the comparison of disease activity categories by DAPSA and cDAPSA was 0.932 (95% CI 0.885 to 0.980) (table 3B).
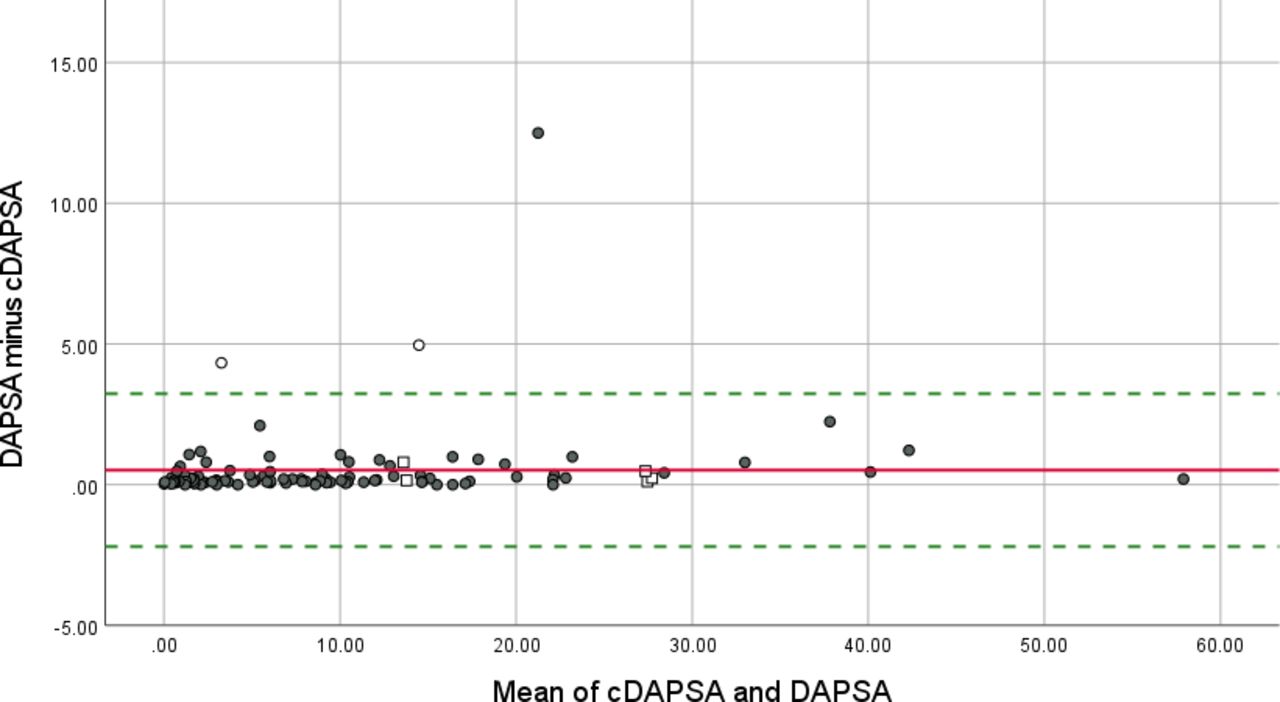
Identical numerical values by cDAPSA and DAPSA were observed in 11 of 104 (10.6%) patients when values were rounded to one decimal. Mean of the differences between DAPSA and cDAPSA was 0.5±1.4 with differences ranging up to 12.5 points. The ICC for DAPSA and cDAPSA was 0.995 (95% CI 0.992 to 0.997) as shown in table 2. The agreement of numerical values by DAPSA and cDAPSA is shown in a Bland-Altman plot (figure 3).
{kind=link}
{kind=link}
{kind=link}
Bland-Altman plot for cDAPSA and DAPSA. Difference in disease activity category between cDAPSA and DAPSA: higher disease activity category with cDAPSA (one category higher with cDAPSA). Same disease activity category. Higher disease activity category with DAPSA (one category higher with DAPSA). The solid line marks the mean difference between cDAPSA and DAPSA (0.520). The dotted lines indicate the 95% limits of agreement (−2.197 to 3.237). X-axis and Y-axis indicate the ‘mean of cDAPSA and DAPSA’ as well as ‘DAPSA minus cDAPSA’ in DAPSA points. cDAPSA, clinical DAPSA; DAPSA, Disease Activity index for PSoriatic Arthritis.
Discussion
This analysis aimed to evaluate the DAPSA using a qCRP assay. The Q-DAPSA resulted in identical disease activity categories in 98.1% of patients with PsA compared with the conventional DAPSA, while identical numerical values according to both scores were observed in 57.7%. Determination of qCRP needs only one drop of blood and qCRP values are available within 2 min after blood sampling, making the Q-DAPSA a quickly available and precise method to monitor disease activity in patients with PsA.
The investigated cohort reflects a typical PsA cohort as the mean age was about 51 years, the gender ratio was almost equally distributed and patients received a broad variety of different medical therapies including systemic glucocorticoids, NSAIDs, csDMARDs, bDMARDs and tsDMARDs. Additionally, our cohort included recently or newly diagnosed patients with PsA as well as patients with longstanding disease. The study was performed as a multicentre design, with patients with PsA being recruited from various rheumatologic centres with different settings—including university hospitals and outpatient practices, therefore giving a broad representation mimicking a real-life situation in Germany.
In the current study, mean qCRP values were slightly higher than mean routine laboratory CRP values. This is in line with the results for the validation of ASDAS-Q16 17 and SDAI-Q.18 As observed in our other studies in axial patients with SpA16 17 and patients with RA,18 the tendency for slightly higher qCRP values showed almost no influence on the disease activity classification since DAPSA and Q-DAPSA resulted in identical disease activity categories in 98.1%. Analysing the two patients with discordant disease activity categories of DAPSA and Q-DAPSA, both showed DAPSA and Q-DAPSA values very close to the cutoffs of the respective disease activity categories and only small deviations of routine laboratory CRP and qCRP values (online supplemental table S2).
The Bland-Altman plot for routine laboratory CRP and qCRP (figure 1) shows one patient with a rather high difference of 3.97 mg/dL between routine laboratory CRP and qCRP. Routine laboratory CRP of this patient was 4.33 mg/dL, and qCRP was 8.33 mg/dL. A reasonable explanation for this high deviation could be problems in the handling of the sample and in the performance of the qCRP analysis—but possible theories remain speculative due to the cross-sectional design of the study: In absolute high CRP values with high concentrations of CRP in the patient’s blood sample, small differences in the sample’s quantity for the qCRP tests may result in rather high differences between qCRP and CRP values. The blood sample for the qCRP test is taken with a microcapillary that draws exactly 10 microlitres, but failure to wipe off the excess blood on the outside of the microcapillary can lead to falsely elevated qCRP values. Another reason could be a delayed collection of the blood sample from the blood collection system. Here, the blood in the blood collection system can coagulate and a higher amount of serum (and fewer erythrocytes) may be drawn up into the microcapillary, which may alter the measured qCRP concentration. A possible solution for this problem is a timely transfer of the blood in the blood collection system into the microcapillary or using blood from EDTA or heparin tubes where blood coagulation is inhibited.
DAPSA and cDAPSA showed an almost perfect agreement regarding identical disease activity categories (in 93.3% of patients, weighted Cohen’s kappa 0.932). Five patients showed higher disease activity categories with cDAPSA compared with DAPSA (online supplemental table S2). All of these patients had rather low routine laboratory CRP values (< 0.8 mg/dL) and consequently similar DAPSA and cDAPSA values. The different disease activity categories in these five patients arose from the slightly lower cDAPSA cut-off values for low, moderate and high disease activity in comparison to the conventional DAPSA cut-off values. The two patients with lower disease activity categories by cDAPSA in comparison to DAPSA had high routine laboratory CRP values (4.33 and 4.96 mg/dL) and consequently rather high deviations between the numerical DAPSA and cDAPSA values (online supplemental table S2). This may indicate that DAPSA and Q-DAPSA could be more suitable to detect high systemic inflammation in a proportion of patients with PsA in comparison to cDAPSA. Interestingly, the patient with PsA with the highest CRP value in our study (routine laboratory CRP and qCRP=12.5 mg/dL) achieved an identical disease activity category by DAPSA/Q-DAPSA and cDAPSA despite a high numerical difference of 12.5 points between DAPSA and cDAPSA (figure 3). The DAPSA and Q-DAPSA values for this patient were 27.50, and the cDAPSA value was 15.00, all indicating moderate disease activity. The DAPSA and Q-DAPSA values were very close to the upper DAPSA cut-off value of moderate disease activity (≤28) while the cDAPSA value was close to the lower cDAPSA cut-off value of moderate disease activity (>13).
Gonçalves et al reported a similar, but slightly lower proportion of agreement between DAPSA and cDAPSA: 88.3% of patients with PsA showed identical disease activity categories by cDAPSA and DAPSA with a kappa of 0.840.11 Van Mens et al investigated the performance of different remission and low disease activity definitions in patients with PsA with quiescent disease according to the treating rheumatologist.12 They found an almost perfect agreement for remission (kappa 0.959) and low disease activity (0.988) by DAPSA and cDAPSA.12 Moreover, they found similar proportions of elevated CRP values in patients in remission according to scores using CRP values (DAPSA, PASDAS) in comparison to scores not including CRP (cDAPSA, Very Low Disease Activity).12 They concluded that determination of CRP values does not have an additional benefit for the assessment of remission and low disease activity in patients with PsA.12 These results underline the importance and clinical usefulness of fully clinical scores in general and the cDAPSA for disease activity assessment in patients with PsA. However, the study by van Mens et al used a preselected dataset of patients with quiescent disease according to the treating rheumatologist.12 In this patient group, normal CRP values would be expected in the majority of cases. In a non-pre-selected group of patients with PsA, the proportion of elevated CRP values might be higher, and CRP might have a stronger influence on disease activity assessment.
Several studies showed the importance of CRP as a prognostic parameter for structural progression in PsA patients.13–15 Borst et al investigated the influence of time-averaged SJC and time-averaged CRP values on structural progression and found intermediate progression when only one variable was positive and highest progression rates when both variables were positive.15 They concluded that CRP values are independently associated with structural progression in patients with PsA.15 These findings highlight the importance of regular CRP determination in patients with PsA and show possible advantages of disease activity scores that also consider the biochemical inflammation in PsA.
As in our parallel studies,17 18 all study centres were located in Berlin that can be discussed as a limitation. On the other hand, with a population of 3.7 million inhabitants22 and an even larger catchment area, this can be assumed as representative for the wider German population. Other limitations of our pilot study include the cross-sectional design and the rather small study population of 104 patients with PsA. However, after these first positive proof-of-concept results, the performance of Q-DAPSA should be validated in larger cohorts of patients with PsA, in different populations as well as in a longitudinal design to test its sensitivity to change in the future. As a further potential limitation of our study, it might be discussed that patients included were solely selected based on their clinical diagnosis of known PsA by their treating rheumatologist and the fulfilment of the Classification criteria for Psoriatic Arthritis criteria23 has not been assessed systematically in this study cohort. Furthermore, the number of patients who were not included in the study due to meeting at least one exclusion criterion (signs of an acute infection or previously known clinically significant anaemia) was not recorded systematically. Therefore, another possible limitation of this study is that we are not able to specify the number of excluded patients due to meeting any of these exclusion criteria. A further limitation might be that the used qCRP assay only provides results for haematocrit values between 15%and 75%.19 However, haematocrit values out of this range are expected to only rarely appear in patients with PsA in clinical routine.
In conclusion, the Q-DAPSA showed an almost perfect agreement with the conventional DAPSA, is timely available in clinical routine and additionally includes an acute phase parameter. Therefore, the Q-DAPSA could be used as one possible option for disease activity assessment in patients with PsA and may ease the performance of the T2T concept in clinical trials and clinical routine.
Data availability statement
Data are available upon reasonable request. De-identified participant data can be made available after approval of a written request for scientific purposes by the corresponding author.
Ethics statements
Patient consent for publication
Ethics approval
The ethical principles of the Declaration of Helsinki and Good Clinical Practice (GCP) were complied. The study and all study-specific measurements were approved in advance by the responsible ethical committee of the coordinating study centre (Charité-Universitätsmedizin Berlin, Berlin, Germany, EA4/208/19). All included participants provided written informed consent prior to any study procedures. The reporting of the study was performed in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
The authors would like to deeply thank Braun T, Doerwald C, Deter N, Höppner C, Igel S, Lackinger J, Lorenz C, Lunkwitz K, Mandt B and Zernicke J for their practical support and coordinating the study. This work was previously presented as a poster at the EULAR congress 2021, at the 'Deutscher Rheumatologiekongress' 2021 and at the ACR Congress 2021.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
FP and JS are joint first authors.
Twitter @ProftDr, @mprotopopov
Contributors FP and JS both contributed equally to this work. FP: guarantor of this work, conceptualisation, funding acquisition, investigation, methodology, project administration, writing—original draft, writing—review and editing. JS: formal analysis, investigation, project administration, writing—original draft. HB, JB, GRB, HH, HK, KK, SL, MP, JR, VR, SZ: investigation, writing—review and editing. BM: conceptualisation, investigation, writing—review and editing. MT: conceptualisation, methodology, writing—review and editing. MV: formal analysis, methodology, software, validation, writing—review and editing. DP: conceptualisation, funding acquisition, investigation, methodology, writing—review and editing.
Funding This work was partially supported by an unrestricted research grant from Novartis [MAIN457A_FVMH0]. Testing kits were provided free of charge from Aidian Oy, Finland.
Competing interests FP: reports grants and personal fees from Novartis, Lilly and UCB and personal fees from AbbVie, AMGEN, BMS, Celgene, Janssen, Hexal, MSD, Pfizer and Roche outside the presented work. JS: nothing to disclose. HB: nothing to disclose. JB: personal fees from AbbVie, Affibody, BMS, Galapagos, Gilead, Janssen, Lilly, Medac, MSD, Novartis, Pfizer, Roche, Sanofi-Aventis, Sun Pharma and UCB outside the presented work. GRB: personal fees from AbbVie, Amgen, BMS, Galapagos, Lilly, MSD, Pfizer, Roche and Sanofi outside the presented work. Editor-in-Chief of RMD Open. HH: Personal fees from AbbVie, MSD, Janssen, Roche, Pfizer, Sobi and Novartis and support for attending meetings and/or travel from AbbVie, MSD, Janssen, Roche, Pfizer and Sobi outside the presented work. HK: nothing to disclose. KK: nothing to disclose. SL: nothing to disclose. BM: nothing to disclose. MP: personal fees from Novartis and support for attending meetings and/or travel from UCB outside the presented work. JR: support for attending meetings and/or travel from Novartis, UCB and AbbVie outside the presented work. VRR: nothing to disclose. MT: personal fees from AbbVie and support for attending meetings and/or travel from UCB outside the presented work. MV: nothing to disclose. SZ: nothing to disclose. DP: reports grants and personal fees from AbbVie, Eli Lilly, MSD, Novartis and Pfizer, and personal fees from Bristol-Myers Squibb, Janssen, UCB, Biocad, GlaxoSmithKline, Galapagos, Gilead, Moonlake, Medscape, Peervoice and Samsung Bioepis outside the presented work.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.