Article Text

Abstract
Objective Adhesive capsulitis is a common painful shoulder condition. Treatment for the condition remains unsatisfactory. Suprascapular nerve block (SSNB) shows promise as a treatment option for adhesive capsulitis but there are no randomised controlled trials that examine its effect on pain or duration of the condition. The objective of this study was to examine the efficacy of SSNB for the management of adhesive capsulitis.
Methods A randomised double-blind placebo-controlled trial of SSNB and standard therapy versus placebo and standard therapy was performed. In total, 54 patients were enrolled in the study. 27 patients received a glenohumeral joint (GHJ) injection and physiotherapy plus a 3-month SSNB, and 27 patients received a GHJ injection and physiotherapy plus a 3-month placebo injection. Patients were followed to resolution of their symptoms as measured by a combination of range of movement, pain scores, Shoulder Pain and Disability Index (SPADI) scores and perceived recovery scores. The primary outcome measure was time to resolution of symptoms.
Results Participants who received the SSNB reduced the duration of their symptoms of adhesive capsulitis by an average of 6 months (mean time to resolution 5.4 (95% CI 4.4 to 6.3) months vs 11.2 (95% CI 9.3 to 13) months) in the placebo group. They also had reduced pain scores, improved range of movement and lower SPADI scores compared with the placebo group across all time points.
Conclusion SSNB reduced the duration of adhesive capsulitis and resulted in improved pain and disability experience for patients.
Trial registration number Australian New Zealand Clinical Trials Registry (ANCTRN 12615001378516).
- Arthritis
- Physical Therapy Modalities
- Rehabilitation
- Analgesics
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Adhesive capsulitis is a common painful condition of the shoulder. Its cause is unknown and treatment options remain unsatisfactory.
WHAT THIS STUDY ADDS
Suprascapular nerve block is a safe, simple and effective adjunct therapy for the treatment of adhesive capsulitis. It is well tolerated and shortens the duration of the condition substantially while reducing pain and improving range of movement.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Suprascapular nerve block is inexpensive, easy to perform in the clinic and very safe. As a result of these findings, it can be used with confidence as an effective therapy for the management of adhesive capsulitis.
Introduction
Adhesive capsulitis is a common condition characterised by painful restriction of glenohumeral movement (both active and passive) in the absence of joint degeneration sufficient to explain the restriction.1 The basic molecular mechanisms remain poorly understood.2 3 There are associations with several conditions including diabetes, stroke4 and prior trauma.5 The prevalence is between 3% and 5% but rates as high as 20% are reported with diabetes.6 The peak age of onset is between 40 and 60 years, and women are affected at a slightly higher rate.7 Diagnosis is based on history and clinical examination with investigations often being normal.
Adhesive capsulitis has three overlapping phases: the painful phase (typically lasting 2–9 months) associated with concurrent progressive loss of motion; the frozen phase (typically lasting 4–12 months) characterised by considerable restriction in the range of movement and the thawing phase which can last 12–36 months.8 Adhesive capsulitis is generally a self-limiting condition but does not always fully resolve. One study suggested 35% of patients had mild to moderate symptoms and 6% had severe symptoms after 4 years.4
Treatment goals are to relieve pain, improve movement, reduce symptom duration and facilitate a return to normal activities. Options include ‘watchful waiting’, oral medication, exercise, physical therapies, joint injection, hydrodilatation, manipulation under anaesthesia and arthroscopic capsular release. There is currently no consensus about the overall management of the condition and the sequence in which treatments should be offered.9 A recent survey among healthcare practitioners suggested that the treatments selected should depend on the phase of the disease, that aggressive mobilisation should be avoided in the early phase and surgical intervention should be generally reserved for when other interventions failed. Recommended interventions for the painful phase were conservative treatment, physical therapy and intra-articular (IA) steroid injection. For patients in the resolution phase, surgery was the most preferred option (mainly manipulation under anaesthesia and arthroscopic capsular release).9 There is also some evidence of short-term benefit of capsular distension.10
One systematic review11 found that IA steroid combined with physiotherapy was the only treatment showing a significant beneficial treatment effect compared with placebo. A second systematic review concluded that the early use of IA corticosteroids in patients with frozen shoulder is associated with better recovery.12
The suprascapular nerve is the major sensory nerve to the shoulder, especially in the posterior and superior aspect, and is an accessible target for blockade. Chronic shoulder pain syndromes in which suprascapular nerve block (SSNB) has been used include rheumatoid arthritis (RA), osteoarthritis (OA) of the glenohumeral joint,13 shoulder pain following stroke,14 shoulder pain with motor neuron disease15 and various rotator cuff disorders.16 The procedure is very safe, with a complication rate of less than 0.6%.17
Studies to date examining the role of SSNB in the management of adhesive capsulitis are limited. A trial using two different methods of SSNB on patients with adhesive capsulitis demonstrated a significant improvement in pain and range of motion (ROM) scores, but follow-up was limited to only 60 min.18 A second study showed an additional benefit of SSNB to a physical therapy programme, but again the outcome measurements were short term.19 A randomised trial (30 patients) compared the effects of SSNB with IA shoulder injections for adhesive capsulitis with a longer follow-up period.20 This found that SSNB produced faster onset and more effective analgesia compared with IA injections. Improved shoulder function (measured by abduction and external rotation) was also observed. These effects lasted up to 3 months. One further study using bupivacaine alone showed improvement in pain for a month.21 There have been no trials to date combining standard therapy with SSNB.
Given the limited results of most treatments and the encouraging results to date with SSNB, we undertook a randomised, double-blind placebo-controlled study of IA glenohumeral joint injection and physiotherapy (the most effective conservative therapy currently recommended)12 with or without SSNB, to examine the efficacy of SSNB in the treatment of adhesive capsulitis.
Methods
Patients were referred to the rheumatology service in the Southern Adelaide Local Health Network for consideration. Inclusion criteria were age ≥18 years, pain and stiffness in predominantly one shoulder for >2 months, and restriction of passive motion greater than 30° in two or more planes, measured with a gravity inclinometer. Patients were reviewed by a rheumatologist, and an X-ray and shoulder ultrasound were performed.
Exclusion criteria included severe pain at rest, systemic inflammatory disease, radiological evidence of OA of the glenohumeral joint or fracture, reason to suspect a complete rotator cuff tear, allergy to local anaesthetic, pregnancy, surgery to the shoulder in the last 12 months or likely not to comply with follow-up.
The study was prospectively registered with the Australian New Zealand Clinical Trials Registry (ANCTRN 12615001378516). A power calculation determined that 20 subjects would be required in each arm to detect an improvement in abduction of 90° compared with an improvement of 30° with usual therapy (80% power significance of 0.05).
All participants gave written informed consent. Following enrolment, demographic data were collected. Patients were then randomised using a concealed envelope system to two treatment groups. Participants, the metrologist and the treating physiotherapist were blinded to the allocation.
The first group received an IA injection into the glenohumeral joint with 20 mg of triamcinolone and 2 mL of 2% local anaesthetic plus a physiotherapist-directed exercise programme and a 12-week SSNB. The second group received the IA injection plus physiotherapy and a 12-week placebo injection into the subcutaneous tissue over the suprascapular fossa. The IA injection was performed with the patient prone, identifying the coracoid process and injecting lateral to this into the glenohumeral joint line. The SSNB was performed with the patient sitting and the rheumatologist working from behind, using anatomical landmarks.13 Briefly, the spine of the scapular and the angle of the scapular are identified, and a perpendicular line is drawn from the angle of the scapular. The injection point is located approximately 2 cm lateral to the intersecting point between this line and the line of the spine of the scapular in the upper outer quadrant, over the suprascapular fossa. Ten milligrams of 0.5% bupivacaine plus 40 mg methylprednisolone are injected deep into the fossa to achieve an indirect SSNB. The placebo was injected into the same location, with the same preparation, using 2 mL of normal saline subcutaneously. Patients were blinded to the intervention. All injections were performed by the same person, who had no role in the ongoing clinical assessment.
Physiotherapy involved individualised mobilisation and stretching exercises and up to six sessions of exercise prescription/demonstration over a 6-week period. The exercise programme comprised physiological movements in all three planes of motion. Patients were encouraged to stretch into stiffness, holding each stretch for 20 s up to six times, for a total of 2-minute stretching. The programme was to be completed twice per day. Pain was not a limiting factor unless the intensity of pain remained elevated for more than 60 min in which case patients were encouraged to modify the intensity of their exercises.22 23 At 12 weeks, the patients were reassessed, and further management offered in terms of a repeat SSNB (or placebo). If the patients’ pain and range of movement scores had returned to normal and they were satisfied with the outcome, they were discharged from the study, otherwise follow-up continued with repeat offers of injection therapy every 12 weeks until resolution of symptoms or participant satisfaction with their recovery.
Pain and disability were measured on the Shoulder Pain and Disability Index (SPADI). A reduction of 40% on the ‘total’ SPADI scale was considered sufficient improvement.24 Full abduction was defined as equal to or greater than 160°, full external rotation was defined as equal to or greater than 45°.25 Pain was assessed using 100 mm Visual Analogue Scale (VAS) for pain with a 20 mm reduction on the VAS26 considered adequate improvement. A patient-perceived recovery questions (measured on a Likert scale, 1–5) was also asked at each of the follow-up assessments. The scale ranged from 1 to 5 with 1 equal to ‘worse’, 2 ‘unchanged’, 3 ‘improved but unsatisfactory’, 4 ‘improved satisfactory’ and 5 ‘improved good to very good’. Scores of 4 or 5 were considered satisfactory. Finally, satisfaction with treatment results was asked with a score of 8 out of 10 on a Likert scale considered very satisfied. At baseline and at each follow-up, the SPADI27 28 and VAS were used to measure pain and disability. Active and passive abduction, flexion and external rotation were measured by a metrologist using an inclinometer.29 The patient-perceived recovery question was also asked at each follow-up assessment.
The primary outcome measure was time to resolution. Secondary outcomes were differences in active flexion, abduction and external rotation, the difference in VAS, and the difference in total SPADI score and in the perceived rate of recovery.
Statistical analyses were undertaken using STATA V.16.30 Descriptive statistics using Χ2 tests and t-tests were used to compare the demographic characteristics. Cross-sectional analyses were undertaken at baseline, 3 months, 6 months and 9 months, to compare ROM, VAS and SPADI scores between groups, at each time point, using t-tests. The primary outcome (mean time to recovery) was determined. The difference between the two groups was examined over time using t-tests and survival analysis. Finally, longitudinal analyses using multilevel linear mixed models were undertaken to compare differences over time for the secondary outcomes.
Results
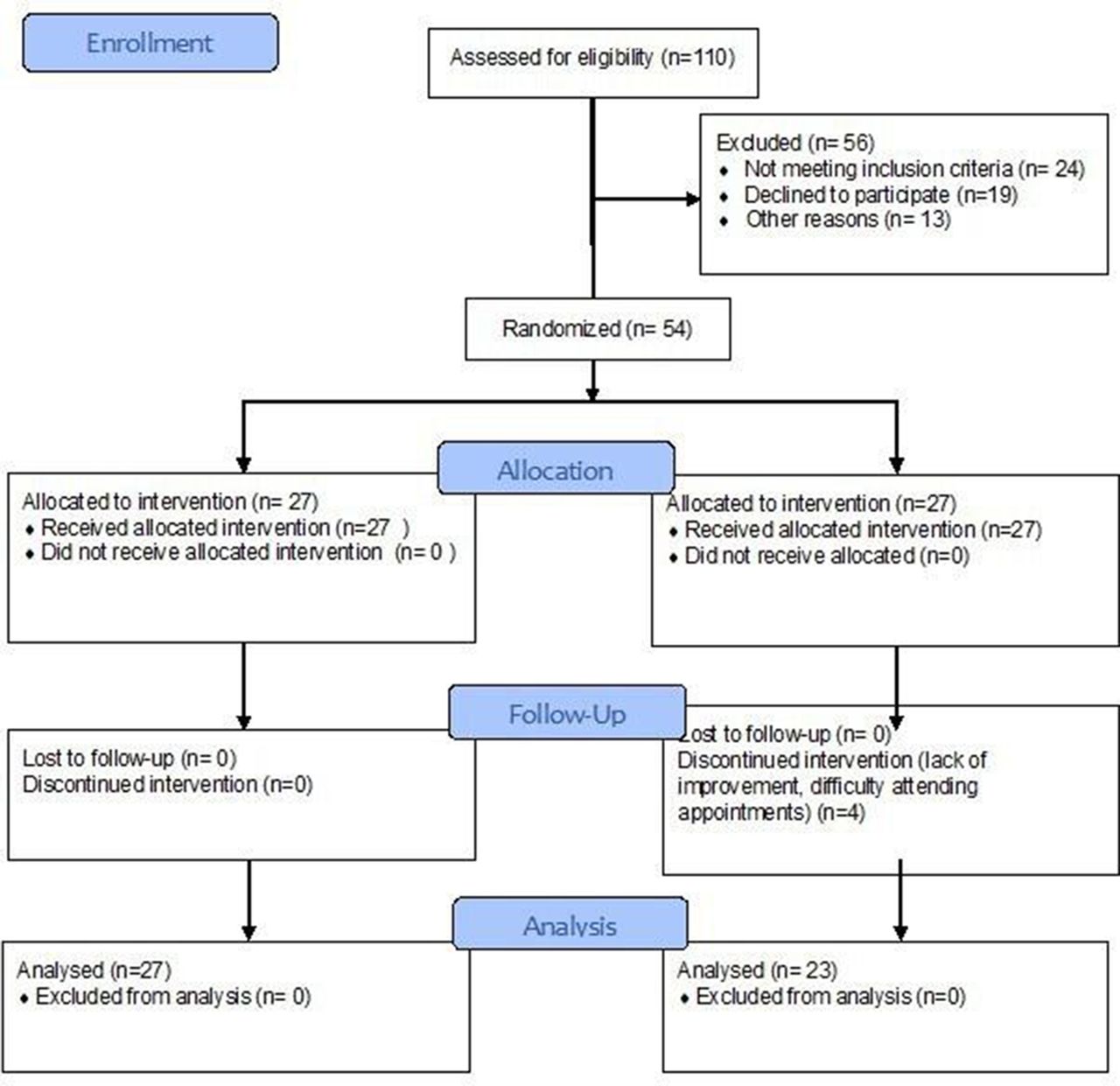
A total of 110 patients were identified; 74 were screened and 20 patients excluded. Of those initially identified, 6 had resolved, 15 were not interested and 8 had an alternative treatment planned. Of those excluded, 8 had an alternative explanation for the shoulder problem (OA, RA, rotator cuff disease), 10 did not meet the diagnosis, 4 had significant comorbidities and 1 reported anaphylaxis to local anaesthetic. Therefore, 54 patients were randomised to take part in the study (35 women, 19 men, mean age 54 (32–72) years). During the study, four patients withdrew (all in the placebo group). Reasons for withdrawal were failure to improve (2) and difficulty getting to the appointments (2). A total of 50 patients completed the study, 27 in the active arm and 23 in the placebo arm (figure 1).

Consolidated Standards of Reporting Trials flow diagram.
Table 1 summarises the demographic data. There were no significant differences between the placebo and active groups. There were also no statistically significant differences between the two groups in terms of ROM, VAS and SPADI scores. The left shoulder was involved in 30 patients (55%) and 80% of all patients had prior therapy for the shoulder (25% injection alone, 40% injection plus physiotherapy, 15% physiotherapy alone).
Demographic characteristics of study participants
Following exclusion of the four participants who withdrew, the mean time to resolution for the placebo group was 11.2 (95% CI 9.3 to 13.1) months. For the active group, the mean time was 5.4 (95% CI 4.4 to 6.3) months. There was a statistically significant difference between the two groups (t=6.02, p<0.001). This difference was maintained even when the four withdrawals were included in the analysis (data not shown). The Kaplan-Meier curve for the time to resolution (figure 2) also demonstrates a statistically significant difference between the two groups (log rank test p<0.001).
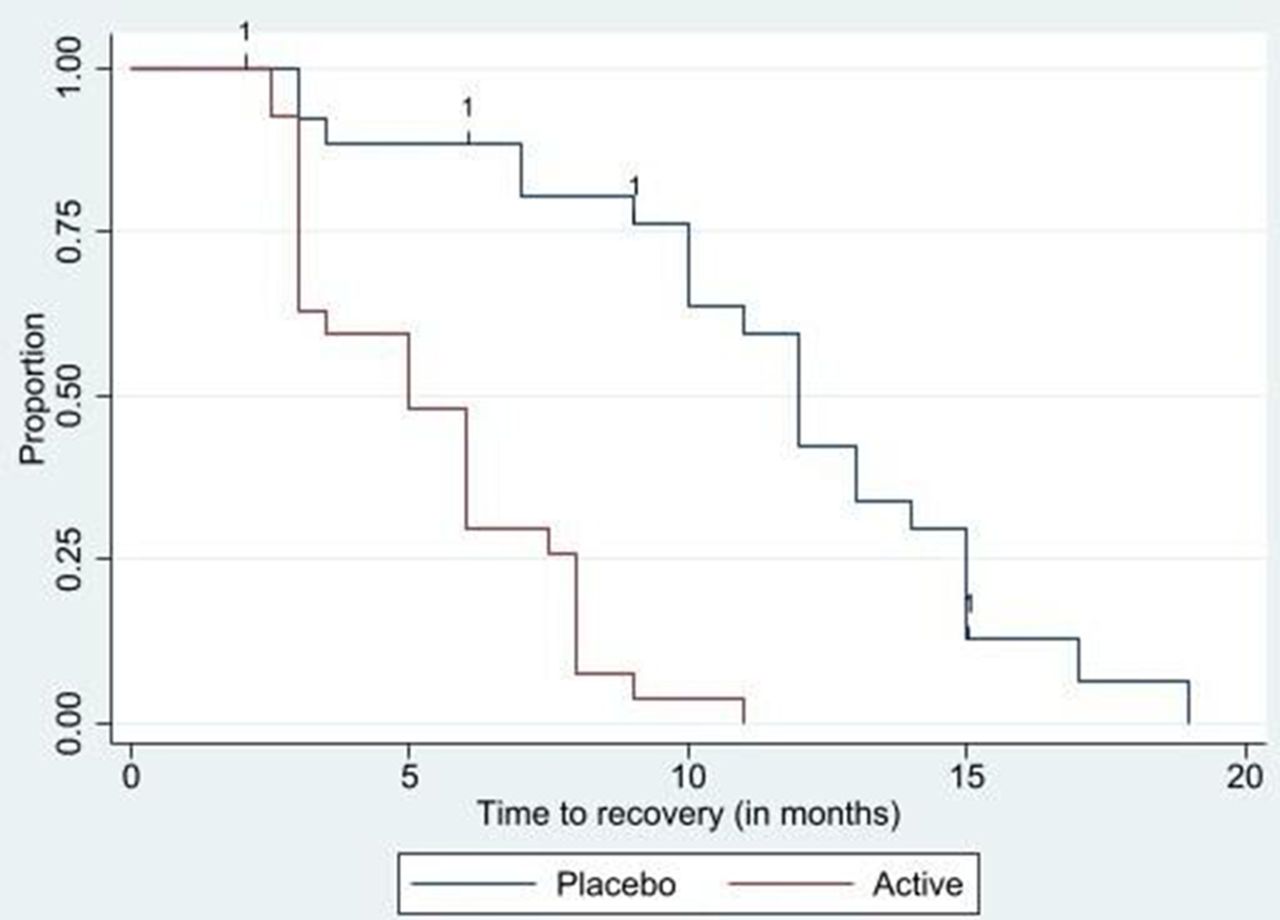
Kaplan-Meier curve of time to recovery. 1 indicates time of censored participant.
Table 2 presents the ROM, SPADI and VAS scores at 3 months, 6 months and 9 months. There were statistically significant differences at each time point between the groups, particularly for active ROM and SPADI scores. For active abduction, improvements between active and placebo groups were statistically significant at each time point.
ROM, VAS, SPADI and perceived rate of recovery at baseline, 3, 6 and 9 months
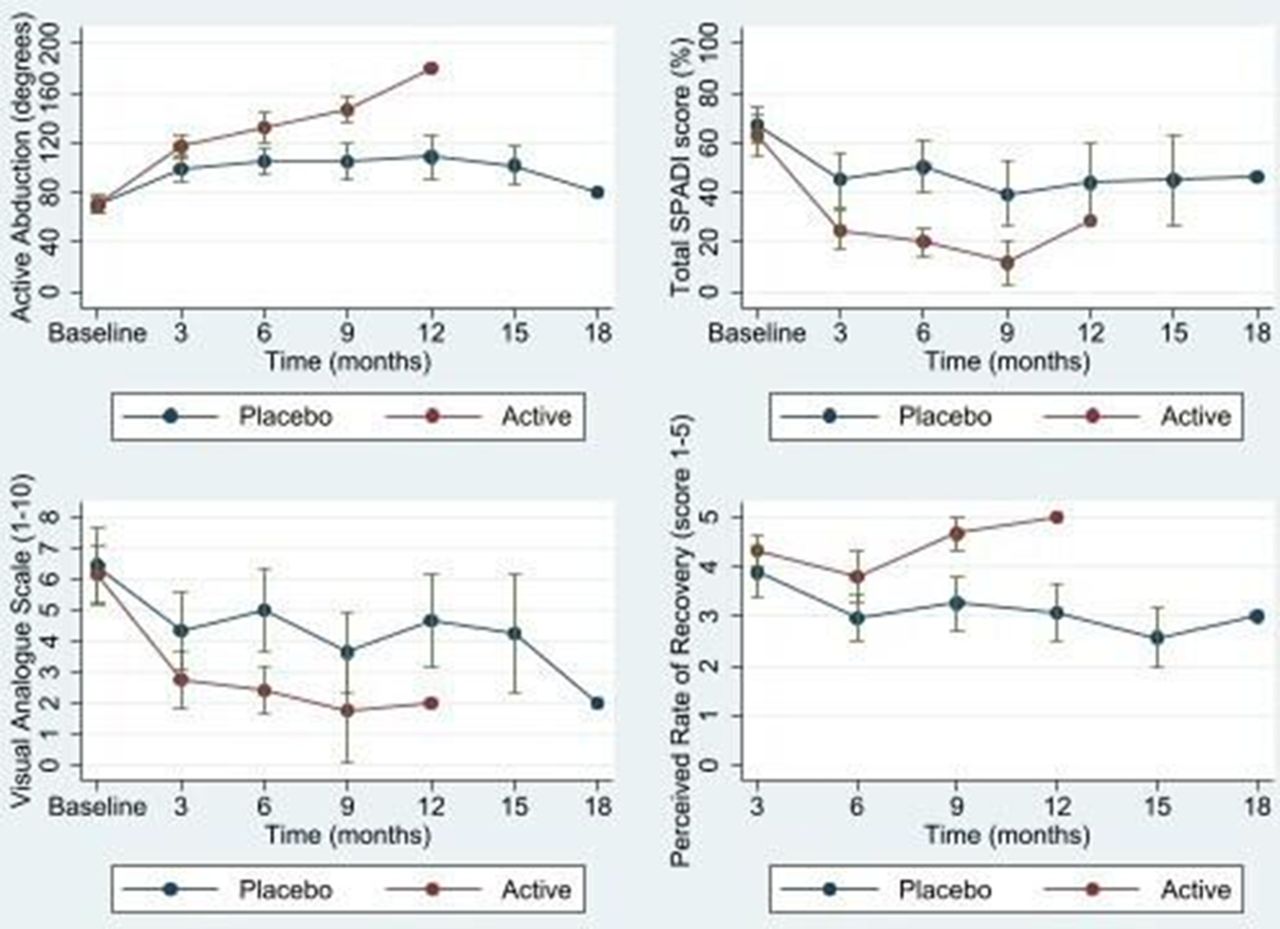
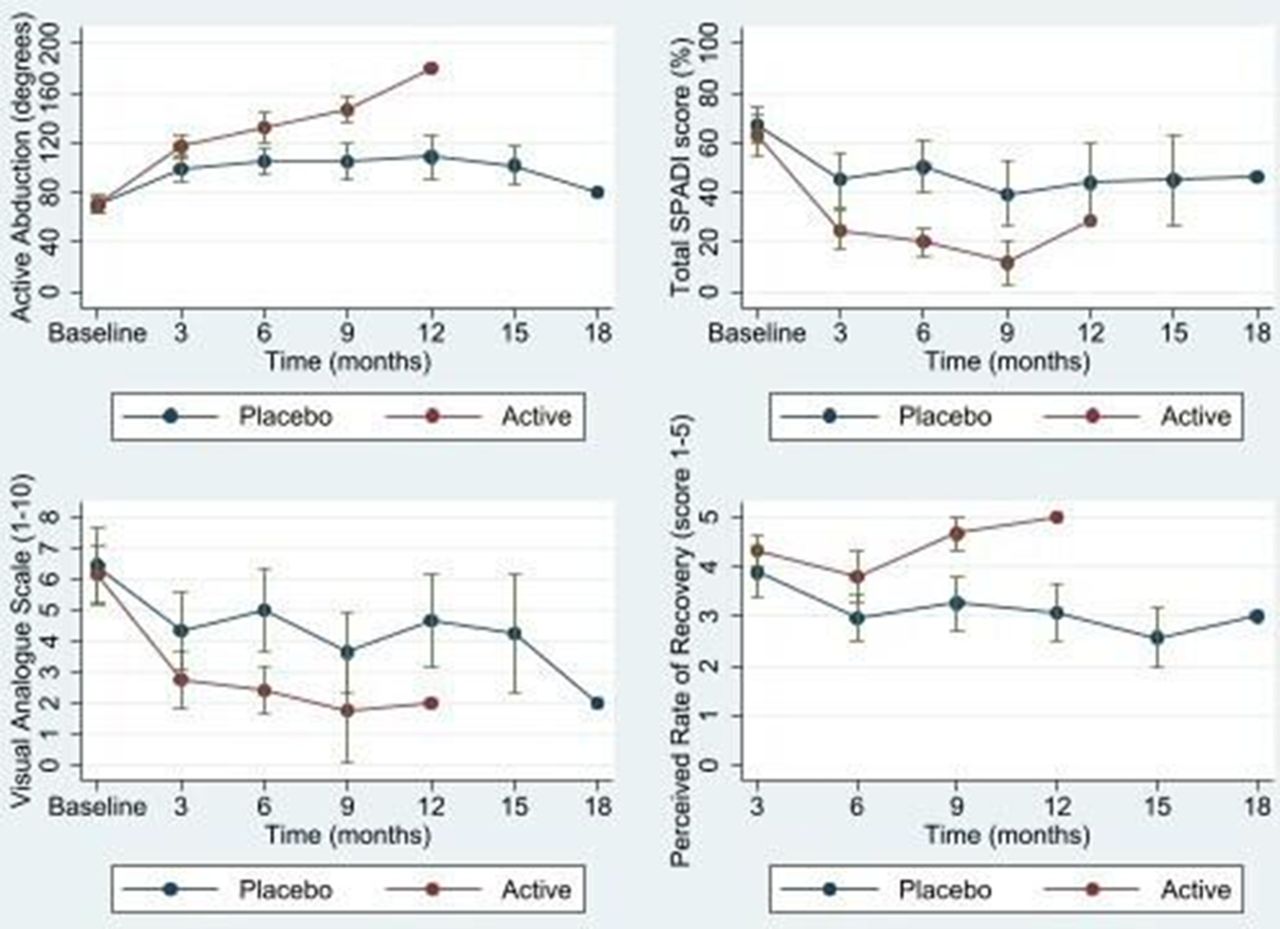
Figure 3 shows the difference until time of resolution for active abduction, the total SPADI score, the VAS and the perceived rate of recovery. The range of active flexion, extension and external rotation over time was examined using multilevel models and indicated that there was a significantly higher ROM for the active group (p<0.001) for all three movements. An interaction term was then included in the model between the groups and the number of visits. The interaction was also significant for all three movements and demonstrates that the increase in ROM was larger over a shorter time in the active group compared with the placebo group.
{kind=link}
{kind=link}
{kind=link}
Differences between the active and placebo groups until the time of resolution: (A) active abduction ROM, (B) total SPADI % score, (C) VAS, (D) the perceived rate of recovery. ROM, range of motion; SPADI, Shoulder Pain and Disability Index; VAS, Visual Analogue Scale.
SPADI scores were statistically significantly lower (better) over time for the active group compared with the placebo (p<0.001) and the decline in score was over a shorter period in the active group (p<0.001). A similar pattern was observed with the VAS. Finally, the patient perceived rate of recovery (higher score indicates higher satisfaction) was significantly higher in the active group (p<0.001) and decreased as the number of visits increased. The rate of recovery was larger in the active group over a shorter period.
Discussion
This study establishes that SSNB is a valuable adjunct therapy for the treatment of frozen shoulder. By adding this treatment to already proven effective therapies, we have been able to significantly reduce the duration of the disease by on average approximately 6 months. Additionally, we have achieved clinically significant reductions in pain, improved function and excellent patient satisfaction with this approach. This contrasts with many currently available therapies.
Most intervention studies reported as having had improvement in pain scores or range of movement scores have relatively short-term outcomes.13 IA injection plus physiotherapy appear to have the most significant positive outcomes31 and the patients in our ‘placebo’ arm improved in a similar fashion to studies using this technique. However, the SSNB is known to provide excellent prolonged analgesia for a variety of shoulder problems, and we hypothesise that this extra analgesia facilitated the effect of the active physiotherapy programme over and above the benefit from the IA corticosteroid. This approach is also consistent with qualitative research suggesting that patients value a focus on pain management in frozen shoulder above other approaches.32
Our focus on disease duration added complexity to the study design and recruitment. We intended to design a study which focused on the duration of disease because this is of major importance to patients. Recruitment into the study was a laborious process as an understanding of frozen shoulder in the community (including many healthcare providers) is poor,8 and so many of the patients potentially referred for consideration of the study did not meet the criteria. It is possible that some of the patients referred but not included in the study did in fact have earlier frozen shoulder (the painful phase). We invited all individuals who had a painful shoulder only to contact us if they started to ‘freeze’, but none did so we have confidence that we did not miss many early frozen shoulders. With the combination of X-ray, ultrasound and clinical examination, we have confidence that those included in the study did indeed have frozen shoulder as their diagnosis, although we should point out that the majority of these also had at least one other abnormality noted on imaging.33
We designed the study to allow the injection therapy to be performed in the clinic. That is, the procedures were not performed under imaging control. Although some argue that radiologically guided injection of the glenohumeral joint may lead to superior outcomes, we have previously demonstrated that this is not the case for the SSNB.34 In any case, we wanted the treatment to be as practical, cheap and efficient as possible.
The study was recruited appropriately based on the power calculations, but the results would have naturally been more robust with larger numbers. Recruiting was challenging and is an issue that others undertaking intervention studies for frozen shoulder have also encountered.32 Strengths of the study include the longitudinal follow-up until resolution and the use of an active comparator group that reflected current best practice. In other words, the outcomes of the active group were over and above current best practice. Given the safety and convenience of the intervention,18 we can be confident in recommending SSNB as a highly useful adjunct therapy.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by the Southern Adelaide Local Health Network Ethics Committee (approval no. 359.15). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
The involvement of our patients and their referring medical practitioners and physiotherapists is gratefully acknowledged. The work of Maurice Shanahan in entering the data for analysis is acknowledged.
References
Footnotes
Twitter @CatherineL_Hill
Contributors MS was responsible for the design, recruiting and writing of the study. TKG was responsible for the analysis and writing of the study. EB was responsible for recruiting and patient assessment and follow-up. CLH helped design the study and contributed to the write-up. GB contributed to patient recruitment and write-up. TM contributed to the design of the study, assessment and patient follow-up and writing the study. All authors gave final approval of the version to be published and agreed to be accountable for all aspects of the work. MS accepts full responsibility for the finished work and/or the conduct of the study, had access to the data and controlled the decision to publish.
Funding This study was supported by a project grant from Arthritis Australia.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.