Article Text

Abstract
Objective To examine how comorbidities in patients with early rheumatoid arthritis (RA) associate with use of different disease-modifying antirheumatic drugs (DMARDs).
Methods We used Swedish nationwide clinical and quality registers to collect comorbidity data for patients diagnosed with RA during 2006–2019 (n=13 505). We compared the use of DMARDs at diagnosis and after 1 year, in relation to comorbidity categories 5 years prior to RA diagnosis and overall comorbidity burden. For each comorbidity category, we also calculated adjusted ORs of being on treatment with other (or no) DMARDs compared with methotrexate (MTX) monotherapy 1 year after RA diagnosis.
Results At RA diagnosis, 68% (n=9178) of all patients were treated with MTX monotherapy, with the lowest proportion in patients with chronic kidney (CKD, 48%, n=50) and respiratory diseases (57%, n=413). At 1 year, most patients still received MTX monotherapy (<11% decrease, across all comorbidity categories). At 1 year, 13% received biological/targeted synthetic DMARDs, with the lowest proportion among patients with malignant diseases (OR=0.69, 95% CI=0.51 to 0.95). Being without DMARD at 1 year was more common among patients with CKD (OR=3.25, 95% CI=2.20 to 4.81), respiratory diseases (OR=1.83, 95% CI=1.32 to 2.53) or a history of hospitalisation due to infection (OR=1.47, 95% CI=1.23 to 1.75), and among patients with higher comorbidity burden and older age.
Conclusion In a nationwide setting with universal healthcare, most comorbid conditions do not limit the initiation or continuation of MTX or other DMARDs in early RA, although patients with certain comorbid conditions, higher comorbidity burden and higher age were somewhat less intensively treated.
- Arthritis, Rheumatoid
- Antirheumatic Agents
- Biological Therapy
- Epidemiology
- Methotrexate
Data availability statement
Requests for data should be directed to the senior author but will be conditioned on the legal premises under which they were collected.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Patients with established rheumatoid arthritis (RA) and certain comorbidities have been shown to receive less intensive disease-modifying antirheumatic drug (DMARD) treatment.
WHAT THIS STUDY ADDS
Among patients with early RA in clinical practice, 68% started with methotrexate (MTX) monotherapy. This treatment was the most commonly used DMARD in all comorbidity categories, although less used in patients with chronic kidney disease (CKD) or respiratory diseases.
At 1 year, 61% of the patients with early RA were still treated with MTX monotherapy and 13% were on a biological/targeted synthetic (b/ts)DMARD. These proportions varied with age and the presence of certain comorbidities, with the lowest b/tsDMARD use among older patients with a history of malignant diseases (5%).
Patients with early RA with a history of certain comorbid conditions—CKD, respiratory, cardiovascular, malignant and infectious diseases—and with a higher comorbidity burden and older age were less intensively treated and more likely to be without DMARD.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Comorbidities and high age are often exclusion criteria in clinical trials, thereby excluding a large part of patients with early RA. Thus, our finding that most patients with early RA with comorbidities start and continue with DMARD therapy in standard care is an important message to patients and their treating rheumatologists.
Introduction
The presence of comorbidities in patients with rheumatoid arthritis (RA) is of importance for several health-related outcomes. The risk of comorbidities in established RA has been thoroughly studied in the last decades, and comorbidities such as cardiovascular diseases are thought to contribute to the excess mortality in RA.1 2 Comorbidities have also been shown to negatively affect RA disease activity and response to disease-modifying antirheumatic drugs (DMARDs).3 4
There is a complex interplay between comorbidities, age and DMARD treatment. Comorbidities may influence the choice of DMARD(s). For instance, tumour necrosis factor (TNF) inhibitors are cautioned in patients with cancer or cardiac insufficiency,5 6 and methotrexate (MTX) is cautioned in patients with chronic kidney disease (CKD) or hepatic insufficiency.7 Conversely, DMARD(s) may result in comorbid side-effects, such as haematological and hepatic toxicity, infections and pneumonitis.7 8 Most randomised trials of DMARDs exclude patients with significant comorbidities, resulting in limited evidence regarding the safety and efficacy in patients with RA with different comorbidities. It is therefore not unexpected that studies have shown that elderly and multimorbid patients are less intensively treated for their RA.9–13 These previous studies have, however, focused on established RA and most have been limited to certain drugs,10 one defined comorbid condition,14 a composite comorbidity score,9 12 or collected information through questionnaires or interviews.12 We have previously shown that the comorbidity pattern among patients with RA differs compared with that in the general population already at RA diagnosis.15
In light of the above, we therefore aimed to investigate the extent to which comorbidities, and the overall comorbidity burden, influence the choice of DMARD at RA diagnosis and the DMARD treatment status at 1 year. Moreover, we assessed the use of MTX monotherapy in relation to comorbidity profile until 3 years after RA diagnosis.
Subjects and methods
Data sources
In this nationwide population-based study, we used register linkages to identify patients with early RA and retrieve information about their comorbidities and RA treatments, as previously described.16–18 In brief, we used data from the Swedish Rheumatology Quality Register (SRQ), which covers over 85% of all patients with RA in Sweden19 to retrieve information about the date of RA diagnosis, symptom duration, treatment and RA serological status. Comorbidity data were collected from the National Patient Register (NPR), which contains data on diagnoses from hospital discharge and also non-primary outpatient care visits through International Classification of Diseases, 10th revision (ICD-10) codes and cancer diagnoses from the Cancer Register. In addition, we used data from the Prescribed Drug Register (PDR) covering all prescribed and dispensed drugs in Sweden; the Education Register and the Total Population Register. A short description of the registers used is listed in online supplemental table 1 and time periods used for the different analyses in online supplemental table 2 and online supplemental figure 1.
Supplemental material
Patients
From SRQ, we included all patients who were registered with early RA (symptom duration <1 year) from 1 January 2006 to 31 December 2019. We excluded patients with data conflicting with the early RA definition (eg, patients registered with other rheumatic diseases in NPR more than 1 year before their RA diagnosis in SRQ, and/or with DMARDs prescribed more than 1 month before the RA diagnosis) (see figure 1 and online supplemental table 3 for excluded diagnoses and drugs). Patients were considered seropositive if they were registered in SRQ with an ICD-10 code for RA as rheumatoid factor (RF) and/or anticitrullinated protein antibodies (ACPA) positive (M05, M06.0L, M06.8L) and as seronegative if coded as RF negative and ACPA either negative or unspecified (M06.0, M06.0M, M06.0N, M06.8M, M06.8N).

Flow chart showing numbers of included and excluded patients with incident RA. RA, rheumatoid arthritis; SRQ, Swedish Rheumatology Quality Register.
Comorbidity data and follow-up
Comorbidity information from 5 years before and up to 1 year after RA diagnosis was collected by linking the study population to NPR and to the Cancer Register to receive ICD-10 codes from hospital discharge and non-primary outpatient care. To extend the search for depression, diabetes, hyperlipidaemia, hypothyroidism and hyperthyroidism and dementia, which are often treated in primary care but for which there are specific treatments, we used drug dispensation data on antidepressants, oral antidiabetics, insulin, lipid-lowering, thyroid, antithyroid and antidementia drugs from the PDR from 18 months before to 1 year after RA diagnosis (see online supplemental table 4 for Anatomical Therapeutic Chemical (ATC) Classification and ICD codes used). Vital status and residency during follow-up were assessed through the Total Population Register. Information on highest attained educational level was assessed through linkage to the Education Register.
Comorbidity categories and comorbidity burden
We defined 31 comorbid conditions and grouped these into 10 categories (cardiovascular, non-cardiac vascular, malignant, endocrine, gastrointestinal, infectious, chronic kidney, neurological, psychiatric and respiratory diseases), in analogy with our previous paper15 (see online supplemental table 4 for ICD and ATC codes). Infectious diseases were restricted to hospitalisation with an ICD code for an infectious disease as main diagnosis.
We used the Rheumatic Disease Comorbidity Index (RDCI) as a measure of disease burden. RDCI is a weighted index that covers lung diseases, cardiovascular diseases, hypertension, fractures, depression, diabetes, cancer and ulcer/stomach problems (online supplemental table 5).20–22 As an alternative approach to assess disease burden, we further retrieved information on the number of dispensed drugs, that is, the number of unique ATC codes dispensed during the 18 months leading up to the RA diagnosis.
Antirheumatic treatment
Information on antirheumatic drug use was collected from SRQ, from 1 month prior until 12 months after the RA diagnosis. The antirheumatic treatment was categorised into five groups: (1) MTX monotherapy, (2) conventional synthetic (cs)DMARDs excluding MTX, (3) MTX combination therapy with other csDMARDs, (4) biological/targeted synthetic (b/ts)DMARDs with or without other csDMARDs, (5) no DMARD treatment. Information about DMARD use at 30 days before to 30 days after RA diagnosis in SRQ was counted as DMARD use at RA diagnosis. MTX monotherapy is the standard first-line DMARD therapy in early RA, and retention of this treatment indicates good effect and tolerance. We therefore extended the evaluation of MTX monotherapy to 36 months after RA diagnosis. We chose to use SRQ as our source of drug information because bDMARDs administered through infusion are only found in SRQ, and SRQ enables a better control of drug discontinuation than the PDR.
Statistical analysis
We evaluated the distribution of comorbidities at baseline and at 1 year. We used McNemar’s test to investigate whether the proportions of patients with each comorbidity category at RA diagnosis differed from the corresponding proportions at 1 year.
We also evaluated the distribution of treatment categories at baseline and at 1 year. Within each comorbidity category, we used the Bhapkar test (ie, the McNemar’s extension to multinomial data) to compare the distribution of treatment categories at RA diagnosis and at 1 year. Within each comorbidity category and each treatment category, we used the Χ2 test to compare the proportion of patients treated versus not treated with this treatment at RA diagnosis and at 1 year. We used the Χ2 test to assess if the distribution of DMARD use at 12 months differed in relation to the RDCI. The Χ2 test was also used to compare the distribution of DMARD use at 12 months between the seropositive and seronegative subsets, for each comorbidity category.
For each comorbidity category, we further used multinomial logistic regression to estimate ORs with 95% CIs for being treated with a specific treatment category (using MTX monotherapy as reference) at 1 year after RA diagnosis. Three different models were used: crude, adjusted for sex and age, and a full model also adjusting for other potential confounders associated with comorbidity risk and treatment: smoking, educational level, serological status and also comorbidity burden (RDCI). Analyses were performed overall and stratified by age over and under 65 years. Patients who died or emigrated within the first year after RA diagnosis were excluded from the analysis comparing MTX monotherapy with other DMARDs in the different comorbidity categories, but kept when comparing the treatment distribution at RA diagnosis and follow-up at 1 year. We handled missing data for smoking, educational level and serological status by adding a separate category for those lacking information. As a sensitivity analysis, we performed a log-binomial regression for all ORs above 3.0. We also evaluated the proportion of patients in each comorbidity category who were treated with MTX monotherapy at diagnosis, 12 months and 36 months. All statistical analyses were performed in SAS V.9.4.
Results
A total of 13 505 patients with early RA were included in the study (figure 1); 68% (n=9113) were female, 69% (n=9255) had seropositive RA. The median age was 62 years (IQR 21), and was slightly higher among seronegative (65 years, IQR 20) compared with seropositive patients (61 years, IQR 21). There were 27% (n=3652) who had less than 10 years of education and 27% (n=3598) who had over 12 years (table 1).
Baseline characteristics
Prevalence of comorbidity categories at RA diagnosis and at 1 year
Table 2 and online supplemental table 6 show the number and proportion of patients with each of the comorbidity categories, and the number of comorbidity categories per person, at the time of RA diagnosis and at 1 year. Overall, the increase in prevalence of comorbidity categories at 1 year compared with at RA diagnosis was proportionally higher among patients with seronegative RA.
Number of patients with the reported comorbidity categories at RA diagnosis and 12 months after diagnosis
DMARD use at RA diagnosis and at 1 year, by comorbidity category
At RA diagnosis, 68% (n=9178) of the patients received MTX monotherapy. However, MTX was used less in patients with certain comorbidities, in particular patients with CKD (48%, n=50) and respiratory diseases (57%, n=413) (figure 2 and online supplemental table 7).

The distribution of treatment categories in patients with RA, all patients and divided in comorbidity categories at RA diagnosis (A) and at 12 months (B). Total number of patients: 13 505. Comorbidity data from baseline (see online supplemental table 7 for exact numbers). The proportion of treatment categories at RA diagnosis and at 12 months was compared using the Bhapkar test. The p value was <0.0001 for all the comorbidity categories, except for the CKD, where the patients were too few to get a result with this test. b/tsDMARDs, biological/targeted synthetic disease-modifying antirheumatic drugs; CKD, chronic kidney disease; csDMARDs, conventional synthetic disease-modifying antirheumatic drugs; MTX, methotrexate; RA, rheumatoid arthritis.
The use of b/tsDMARDs, and MTX in combination with other csDMARDs, increased from diagnosis to 1 year in all comorbidity categories. At 1 year, use of MTX monotherapy had decreased by 7% units (with a range of −11% to +2% in the different comorbidity categories), with 61% (n=8282) of patients with RA in overall cohort treated with MTX monotherapy, including 39% (n=41) of patients with CKD and 47% (n=341) of patients with respiratory diseases. When looking at total MTX use, including combination with csDMARDs and/or b/tsDMARDs, MTX use had instead increased, in all comorbidity categories except CKD, by overall 6% units (online supplemental table 8). Furthermore, 33% (n=35) of the patients with CKD, 21% (n=254) with cardiovascular disease, 20% with respiratory diseases (n=144) and with a history of hospitalisation due to infectious diseases (n=164) were not on any DMARD at 1 year, compared with 13% (n=1778) of patients overall (figure 2 and online supplemental table 7). The patients with CKD and respiratory diseases were, however, older, which might have affected the tendency to treat; in CKD with a median age of 71 years (IQR 15), in respiratory diseases with a median age of 68 years (IQR 16), compared with a median age of 62 years (IQR 21) in the whole patient group.
Treatment with b/tsDMARDs also differed by comorbidity category. At 1 year, 13% (n=1799) of all patients were on a b/tsDMARD (with or without combination with MTX or other csDMARDs), compared with 8% of patients with a history of cardiovascular (n=96) or malignant (n=46) diseases. However, the decreased use in these comorbidity categories was mainly confined to older patients (table 3).
Association of comorbidity categories and antirheumatic treatment categories (b/tsDMARDs or no treatment), compared with methotrexate (MTX) monotherapy, at 12 months after RA diagnosis, stratified by age
DMARD use at 1 year, by comorbidity burden
Patients with a higher comorbidity burden, as measured by RDCI, received less DMARD treatment at 1 year after RA diagnosis (p<0.0001, figure 3), but the differences were nevertheless small and most patients were treated with a DMARD. Thus, among patients with an RDCI of 0, 89% were treated with a DMARD, compared with 84% of those with an RDCI of 2 or more. Very small differences between the RDCI categories were observed for b/tsDMARD use (RDCI=0: 14% and RDCI ≥2: 12%). When comorbidity burden was defined by number of dispensings, patients who used the highest number of non-RA-related drugs were the least often treated with a DMARD at RA diagnosis (online supplemental figure 2).
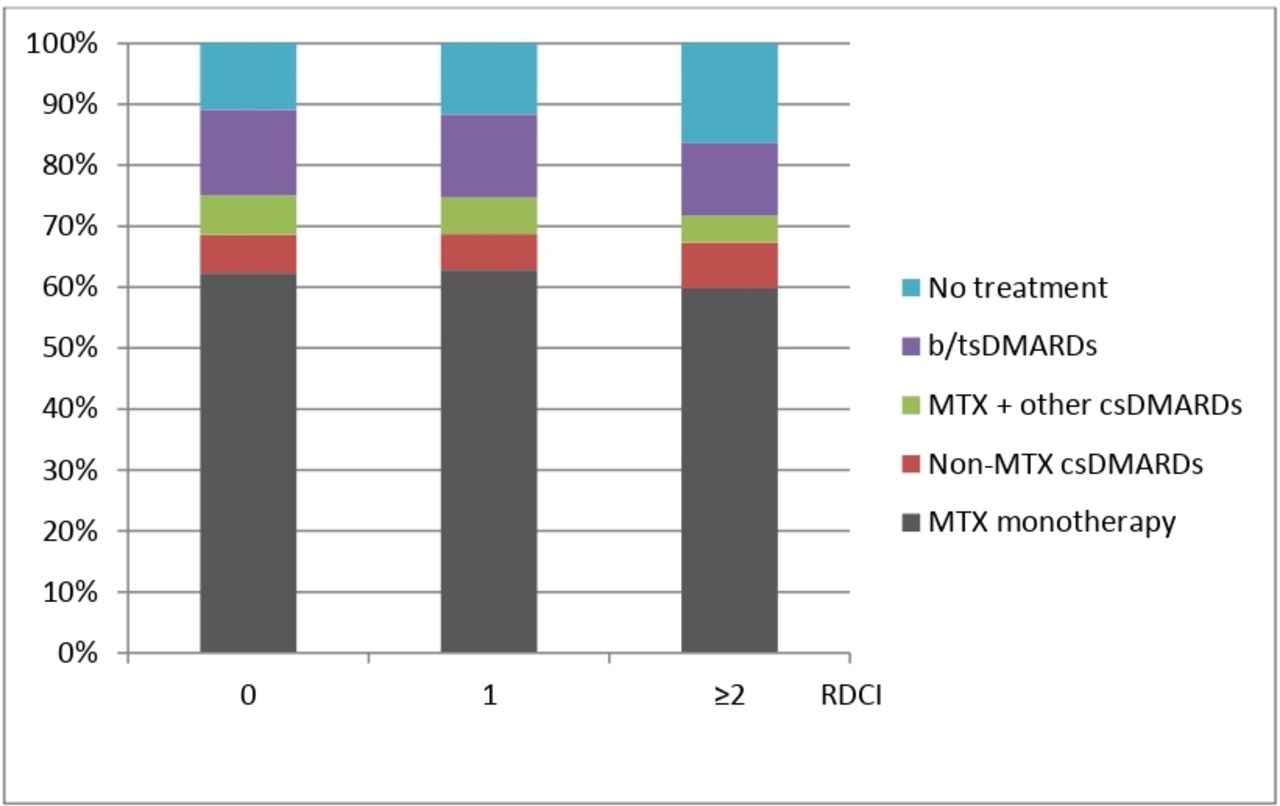
Proportion of treatment categories related to Rheumatic Disease Comorbidity Index (RDCI) at 12 months from RA diagnosis: 7082 (53%) of the patients had an RDCI of 0, 3091 (23%) had an RDCI of 1 and 3200 (24%) had an RCDI of ≥2. Mean RDCI 1.0 (SD 1.4). Maximal possible value of RDCI: 9. Global p<0.0001, calculated by Χ2 test. b/tsDMARDs, biological/targeted synthetic disease-modifying antirheumatic drugs; csDMARDs, conventional synthetic disease-modifying antirheumatic drugs; MTX, methotrexate; RA, rheumatoid arthritis.
DMARD use at 1 year compared with MTX monotherapy, by comorbidity category
Next, using MTX monotherapy, the standard first-line DMARD in RA, as a reference, we evaluated, for each comorbidity category, the OR for being in one of the four other treatment groups, with adjustment for potential confounding factors. There was an increased risk of being without any DMARD treatment at 1 year for patients with a history of CKD (OR=3.25, 95% CI 2.20 to 4.81), hospitalisation due to an infection (OR=1.47, 95% CI 1.23 to 1.75) or respiratory diseases (OR=1.83, 95% CI 1.32 to 2.53) (figure 4 and online supplemental table 9).

ORs of the different treatment categories compared with standard treatment methotrexate (MTX) monotherapy at 12 months, divided by comorbidity categories (full model). The full model was adjusted for sex, age, smoking, educational level, serological status and Rheumatic Disease Comorbidity Index. Results calculated by multinomial logistic regression (see online supplemental table 9 for exact numbers. b/tsDMARDs, biological/targeted synthetic disease-modifying antirheumatic drugs; CKD, chronic kidney disease; csDMARDs, conventional synthetic disease-modifying antirheumatic drugs.
Furthermore, when b/tsDMARD use at 1 year was compared with MTX monotherapy, patients with CKD (OR=2.09, 95% CI 1.25 to 3.48), respiratory diseases (OR=1.89, 95% CI 1.34 to 2.67) and endocrine diseases (OR=1.23, 95% CI 1.05 to 1.45) were more likely to be treated with a b/tsDMARD. In contrast, patients with a history of malignant diseases were less often treated with a b/tsDMARD (OR=0.69, 95% CI 0.51 to 0.95).
When a complete case analysis (ie, excluding patients with missing data) was used instead, no noticeable changes in the ORs were observed. A sensitivity analysis using log-binominal instead of multinomial logistic regression also resulted in similar findings (online supplemental table 10).
DMARD use at 1 year, stratified by age
Since most comorbidities increase with age, we repeated the analysis comparing MTX monotherapy at 1 year with the four other DMARD treatment categories with the same adjustments, but separately for patients below versus above 65 years (table 3 and online supplemental table 11 for detailed results). At 1 year after RA diagnosis, the older patient group was more often on MTX monotherapy or without treatment, in comparison with the younger patients, within most comorbidity categories. In the younger patient group, b/tsDMARDs were prescribed in 14%–23% within the different comorbidity categories, whereas it was prescribed about half as often in the older patient group, with the exception of CKD where the b/tsDMARD use remained similar in the two age groups.
DMARD use at 1 year, stratified into seropositive and seronegative subset
Among the seropositive patients, 15% (n=1369) were treated with a b/tsDMARD at 1 year after RA diagnosis, compared with 10% (n=392) of the seronegative patients (online supplemental table 12). The lower b/tsDMARD use in the seronegative group was seen within several of the comorbidity categories as well as among the patients with none of the comorbidity categories. The seronegative patients were also less often treated with a DMARD, with 16% (n=624) among the seronegative subset and 12% (n=1085) among the seropositive subset, being without DMARD at 1 year.
MTX monotherapy at follow-up
We further evaluated the proportion of patients in each comorbidity category who initiated and continued with MTX monotherapy by 36 months of follow-up. Overall and for all comorbidity categories, this proportion decreased over time (figure 5 and online supplemental table 13), and the slope was similar in all the categories except for the patients with a history of malignant diseases where the proportion of patients on MTX monotherapy increased at 12 months before decreasing at 36 months. The lowest use of MTX monotherapy, at all time points (0, 12 and 36 months), was among patients with a history of CKD, respiratory or infectious comorbidities.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Proportions of patients in the different comorbidity categories that remain on methotrexate monotherapy at RA onset, 12 and 36 months after diagnosis. Comorbidity data at RA onset refer to reported comorbidities 5 years before up to RA diagnosis. Comorbidity data at 12 and 36 months refer to the comorbidity situation 5 years before to 12 months after RA diagnosis (see online supplemental table 13 for exact numbers). RA, rheumatoid arthritis.
Discussion
In this large, nationwide, register-based study, we demonstrated that, across all comorbidity categories investigated, a majority of patients with early RA were treated with DMARDs, and that MTX was the most commonly used DMARD. However, patients with a history of CKD, respiratory, malignant or infectious diseases, as well as those with a higher comorbidity burden and higher age, received less intensive DMARD treatment (ie, were not treated with MTX, b/tsDMARDs or any DMARDs), compared with patients overall. Furthermore, the overall decline in the proportion of patients on MTX monotherapy during the first year was 7% units, and the total MTX use, including combination therapy, actually increased by 6% units, indicating a generally good tolerance.
Several comorbid conditions, including CKD, respiratory, malignant and previous severe infectious diseases, should prompt caution when selecting therapy for patients with RA, due to concerns regarding, for example, nephrotoxicity, pneumonitis, cancer recurrence or susceptibility to infections. Patients with a history of these comorbidities are usually excluded from randomised clinical trials. The proportion of non-DMARD-treated patients was rather large in this study; overall, 13% at 12 months and higher in several comorbidity categories, such as CKD. This could reflect that the study is based on routine care, but it is also important to note that glucocorticoid treatment was outside the scope of this study and non-DMARD-treated patients could, thus, have been treated with glucocorticoids. A few observational studies including patients with established RA have shown that elderly and multimorbid patients receive less intensive antirheumatic treatment,9–12 but studies in early RA are scarce. In the present study, we showed that there is a difference in DMARD use, with a tendency of less intensive treatment already in early RA for patients with certain comorbidities, higher comorbidity burden and higher age. However, it is important to note that most comorbid conditions did not limit the initiation or continuation of DMARDs in early RA.
The prevalence of comorbidities increases with age. In a previous study, we demonstrated that 10% of patients with RA 18–49 years of age, 24% of patients 50–74 years and 42% of patients ≥75 years of age had two or more of our defined comorbidity categories at RA diagnosis.15 In our present study, we observed that older patients with early RA received less intensive DMARD treatment. This is in line with previous studies in established RA.9–12 One register-based study found that patients with RA onset above 60 years of age received biological and combination DMARD treatment less frequently than younger patients, despite comparable disease duration, severity and activity.11 In another study from the international collaboration COMORA, the odds of bDMARD use decreased by 11% for each additional comorbidity, adjusted for age and other confounders.9 A Japanese study on patients with established RA with questionnaire-based comorbidity data reported as an age-adjusted composite score showed that patients with a higher comorbidity score were less likely to be treated with MTX and bDMARDs.12 In our study, the pattern of less intensive treatment among older patients was particularly evident for b/tsDMARDs. In patients 65 years and older, treatment with b/tsDMARDs was around two times lower than in patients under 65 years, for almost all comorbidity categories.
The pattern of lower b/tsDMARD use among older patients observed in our study was especially pronounced for patients with a history of malignant diseases. This is not unexpected, since the molecular mechanism of TNF inhibitors has raised concerns regarding increased cancer risks.5 However, several large studies have in recent years shown reassuring results, without increased cancer risks (with a possible exception for non-melanoma skin cancer) for patients with RA on TNF inhibitors and other bDMARDs.23–27 Thus, although our results from patients with early RA diagnosed in 2006–2019 suggest that rheumatologists are cautious of treating older patients with a history of cancer with b/tsDMARDs, it will be interesting to see whether bDMARD prescription in this patient subgroup will increase in the future.
The lower use of b/tsDMARDs seen in the seronegative subset may in part be attributed to the higher age of the seronegative patients. RF and ACPA are also considered to be markers of poor prognosis with higher risk of erosive disease.28 Seropositivity is, thus, a factor to be taken into account in, for example, the European Alliance of Associations for Rheumatology (EULAR) recommendations for the management of RA, why it may affect the propensity to treat seropositive patients more intensively.29 In a previous study, we showed that there were some differences in comorbidity prevalence between seropositive and seronegative patients already at RA diagnosis, for example, higher prevalence of interstitial and chronic obstructive pulmonary disease in seropositive patients, whereas seronegative patients had a higher prevalence of type 2 diabetes.15 In this study, there was a tendency of lower MTX and higher cs/b/tsDMARD use among the seropositive patients with respiratory disease, but the results were not significant.
Our study has several strengths. It is the first study to investigate DMARD treatment in relation to comorbidities in RA from diagnosis and onwards, and also one of the largest studies on comorbidities in RA. Furthermore, it is nationwide and performed in a country with universal access to subsidised healthcare, thereby minimising bias in cohort selection. We had nationwide coverage of information about a large number of comorbidities and all classes of DMARDs. This register-based (as opposed to self-reported) approach to comorbidity assessment avoids the risk of recall bias. Moreover, in the analysis comparing MTX monotherapy use with other DMARDs at 1 year, we could adjust for important confounders that can potentially affect both the presence of comorbidities and DMARD use, such as smoking, age, educational level and serological status. Since many clinical trials do not include patients with a higher comorbidity burden and/or elderly patients, and a large part of all patients with RA belong to these groups, studies based on real-life data are of particular importance.
The main limitation of our study is that only comorbidity diagnoses for specialised healthcare were available. We compensated for this by adding prescribed drugs as an additional comorbidity source for comorbidities that had a specific treatment, for example, antidiabetic drugs. However, for some comorbidities, like CKD, the prevalence was lower than expected, indicating a possible underascertainment of mild CKD. MTX is mainly eliminated by the kidneys and is not recommended if creatinine clearance is less than 30 mL/min. In this study, we were not able to distinguish between the different stages of CKD. It is thus possible that patients with CKD who received treatment with MTX had a mild CKD and/or received a low dose. The results from this study should not be interpreted as MTX is a safe treatment for patients with severe renal insufficiency. Further, grouping of comorbidities into categories can be challenging (eg, regarding asthma, chronic obstructive and interstitial pulmonary disease as a single entity, respiratory diseases), for instance, if included comorbidities would affect the outcome in different directions, the effects may cancel out each other. Also, we used comorbidities as binary variables, whereas in clinical practice, many comorbidities represent a spectrum from mild to severe disease.
We based the DMARD categorisation on Swedish and EULAR guidelines, with MTX being by far the most commonly used first csDMARD in clinical practice in Sweden. An alternative approach would have been to separate non-MTX csDMARD monotherapy from csDMARD combination therapy with or without MTX. However, as the group with non-MTX csDMARD use was small (6%), it is not likely that it would have changed the results to any larger extent. In our main analyses, we used drug information from SRQ due to difficulties to interpret prescription data at follow-up when evaluating whether a patient is still taking the DMARD, and the lack of information about intravenous DMARDs in the PDR. We found a slightly higher prevalence of prescribed DMARDs in PDR compared with SRQ at RA diagnosis, which indicates that the reported drug information in SRQ is, although high, not complete (online supplemental table 14). There is thus a risk of overestimating the proportion of patients without DMARDs when only using SRQ drug data. However, the difference in the proportion of patients without treatment was rather consistent across the comorbidity categories (3.5%–5.7% lower in SRQ compared with PDR), indicating that the type of comorbidity would not have a large impact on the results.
To conclude, our study demonstrates that most patients with early RA do receive and continue on standard DMARD therapy, despite comorbidities. Since patients with comorbidities and higher age constitute the majority of all patients with early RA, this is an important message to patients and to their treating rheumatologist.
Data availability statement
Requests for data should be directed to the senior author but will be conditioned on the legal premises under which they were collected.
Ethics statements
Patient consent for publication
Ethics approval
The Stockholm Regional Ethics Review Board, Sweden, approved the study (DNR 2015/1844–31/2).
Acknowledgments
The authors would like to thank Dr Jonas Söderling for technical assistance with database extraction, and all the clinicians and patients registering in the Swedish Rheumatology Quality Register as well as in other registers used in this study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors All authors contributed to the design of the study and the interpretation of study results. LT performed the analyses, with support of the other authors. All authors participated in writing the manuscript and approved the final version. LT is guarantor of the study.
Funding This work was supported by research grants from the Swedish Research Council, ALF funding from Stockholm County and Karolinska Institutet, grants from King Gustaf V’s 80-year foundation, the Swedish Rheumatism Foundation, NORDFORSK, Swedish Heart Lung Foundation, the Swedish Cancer Society and Karolinska Institutet/Region Stockholm funds.
Competing interests JA has received grants from Abbvie, AstraZeneca, BMS, Eli Lily, MSD, Pfizer, Roche, Samsung Bioepis, Sanofi and UCB; these entities have entered into agreements with Karolinska Institutet with JA as principal investigator, mainly in the context of safety monitoring of biologics via ARTIS/Swedish Biologics Register. SS is a part-time employee of deCODE genetics, unrelated to this work. The other authors have declared no conflicts of interest.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.