Article Text

Abstract
Objectives To investigate whether in rheumatoid arthritis (RA) frequency of local joint inflammation is associated with radiographic joint damage progression in that joint.
Methods Data from 473 patients with RA and available radiographs from the BeSt study were used. Patients were treated to target (Disease Activity Score of ≤2.4) for a median of 10 years. At each study visit every 3 months, joints were assessed for swelling and tenderness. Radiographs of hands and feet were made yearly. A generalised linear mixed model was used to assess the association between the percentage of study visits at which clinical inflammation was observed in a joint (cumulative inflammation) and radiographic joint damage in that same joint. Clinical inflammation was primarily defined as joint swelling (with or without joint tenderness). For secondary analyses, we also investigated joint tenderness without joint swelling. Damage was measured as the percentage of the maximum possible Sharp-Van der Heijde score in a particular joint.
Results Cumulative local joint swelling was associated with local progression of radiographic damage in the same joint (β=0.14, 95% CI 0.13 to 0.15). This association was also found in a subset of joints that were swollen at least once. Cumulative local joint tenderness without concurrent local joint swelling was less strongly associated with local radiographic joint damage progression (β=0.04, 95% CI 0.03 to 0.05).
Conclusions In RA, long-term cumulative local joint inflammation is associated with joint damage progression in the same joint.
- rheumatoid arthritis
- inflammation
- synovitis
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
In early rheumatoid arthritis (RA), joint inflammation is associated with joint damage progression. Since in RA joint inflammation tends to recur in the same joints, joints that are frequently inflamed may be more susceptible for joint damage progression.
WHAT THIS STUDY ADDS
This is the first study in which a frequency-dependent effect of local joint inflammation is shown on local joint damage progression in the same joint on long-term (up to 10 years) follow-up, despite treatment targeted at low disease activity.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
The finding that cumulative joint inflammation is associated with local joint damage progression indicates that clinical joint assessments are a valuable target when treating RA and might indicate that more intensive radiographic follow-up is needed for frequently inflamed joints. To further prevent joint damage, development of new treatment strategies aiming at even stronger inhibition of repeated joint inflammation may be beneficial.
Introduction
Radiographic joint damage progression in patients with rheumatoid arthritis (RA) can result in permanent disabilities and is associated with other negative clinical outcomes.1–3 Earlier and targeted treatment for RA has led to suppression of severe radiographic joint damage progression.4–6 However, in many patients, radiographic damage still occurs.
Radiographic joint damage in RA has been found to be associated with several systemic factors such as high RA disease activity and acute phase marker levels. However, an association between (early) clinical joint inflammation and damage progression has also been found locally.7 8 It has been proposed that joint erosion is a consequence of osteitis accompanying arthritis, and joint space narrowing is a consequence of synovitis causing cartilage destruction.9 10 Recently, we have shown that joints, having been inflamed once, are prone to recurrent local inflammation despite systemic treatment to target.11 This raises the question whether in joints with persistent or recurrent arthritis, local inflammation might have a frequency-dependent effect on local joint damage progression despite targeted, mainly systemic, treatment. A cumulative local effect is plausible but not previously studied with long-term follow-up data.
Here we investigate the association between cumulative joint inflammation over time and the degree of local joint damage progression in patients with newly diagnosed RA who were followed up over a time period of up to 10 years. Since joint tenderness without swelling may also be indicative of inflammation and the relationship between joint tenderness and joint damage progression is debated,12 13 we also assessed the association between cumulative joint tenderness in the absence of joint swelling and damage progression.
Methods
Patients’ data of the BeSt study (BehandelStrategieën, Dutch for treatment strategies) were used for this post hoc analysis. In the BeSt study, patients with early RA according to the American College of Rheumatology 1987 RA criteria and with symptom duration of ≤2 years were randomised into four different treatment strategy arms: (1) sequential monotherapy starting with methotrexate; (2) step-up combination therapy starting with methotrexate; (3) initial combination therapy with methotrexate, sulfasalazine and prednisone; or (4) initial combination therapy with methotrexate and infliximab. Treatment was intensified every 3 months if the treatment target of a Disease Activity Score (DAS) of ≤2.4 was not met. Patients were followed up for up to 10 years. The BeSt study has been described in more detail previously.6 14
Patient and public involvement
Neither patients nor the public were involved in the design, recruitment, conduct or dissemination of the study since this was not common practice at the time the BeSt study was initiated.
Clinical assessment
Assessment of joint swelling (yes/no) and joint tenderness (yes/no) of hand and foot joints was performed every 3 months by trained nurses. Cumulative joint inflammation was primarily defined as the percentage of available study visits at which a joint was swollen, as joint inflammation is more strongly associated with joint swelling than with tenderness.15 16 A percentage of study visits were used to account for differences in follow-up duration and missing assessments during follow-up (91 753/527 958 data points). For secondary analyses, we calculated the percentage of study visits at which a joint was tender but not concurrently swollen.
Radiographic assessment of hand and foot radiographs was performed yearly. Radiographic joint damage was assessed according to the Sharp-van der Heijde method by two independent observers who were blinded for patient identity, clinical outcomes and time order. The intraclass correlation coefficient between the two readers was 0.96 (95% CI 0.95 to 0.97). For the analyses, the mean score of the two readers was used. Per joint, damage was expressed as the percentage of the maximum possible score to account for differences in maximal scores between joints. Maximum joint space narrowing scores range from 0 to 4 (normal to bony ankylosis or complete luxation); erosion scores ranged from 0 to 5 in hand joints (no erosions to complete bone collapse) and 0 to 10 in feet joints (0–5 per bone in one joint). For radiographic assessment of the wrist, the radioulnar, radiocarpal, intercarpal and carpometacarpal joint scores were added together, resulting in a maximum damage score of 54 for the wrist (joint space narrowing and erosions combined). Only joints with baseline clinical and radiographic assessments and at least 1-year follow-up were included in the analyses. Joints were followed up until the last moment at which information on both clinical inflammation and radiographic joint damage were available. For individual joints that were not radiographically assessable on a time point with available radiographic assessments for other joints (for example, because of presence of a prosthesis), the last observation for that joint was carried forward (310/15 846 joints).
Statistical analysis
Association between cumulative joint inflammation and radiographic joint damage
To assess the association between cumulative joint inflammation over time and local radiographic joint damage progression in the same joint, we used a generalised linear mixed model with joints clustered within patients to account for the dependency of different joints within one person. The model was adjusted for baseline joint damage and follow-up duration. The analysis was repeated for erosions and joint space narrowing separately.
For a sensitivity analysis, we included only joints that had complete follow-up (both baseline and 10-year follow-up clinical and radiographic assessments available). To assess both the short-term and long-term association between joint inflammation and joint damage, the analysis was stratified for two time periods: baseline to year 2 (adjusted for baseline joint damage) and years 2–10 (adjusted for damage at year 2).
To better assess whether the local effect of joint inflammation on damage progression is a frequency-dependent effect (opposed to only an effect of ever occurrence of joint inflammation), the primary analysis was repeated in joints that were clinically inflamed at least once.
Effect of treatment strategy arm
Since previously, after 1 year in the BeSt study, no association between clinical joint inflammation and radiographic joint damage was found in participants of the BeSt study who were initially treated with infliximab (treatment strategy arm 4),8 we assessed whether the association was different for different treatment strategies by adding an interaction term between cumulative joint swelling and treatment strategy arm. In case of a significant interaction, a stratified analysis was done.
Local or general inflammatory effect
To identify whether the association between cumulative local joint inflammation and joint damage is a local or a general inflammation effect, we additionally adjusted the primary analysis for the mean DAS score over time. In addition, we did a permutation test with 1000 permutations to study whether local joint damage progression was better predicted by joint swelling in the same joint than by joint swelling in randomly selected other joints, which is indicated by a p value of <0.05.17 A 95% CI for this p value is reported to address the uncertainty of the estimated p value introduced by testing only a selection (ie, 1000 permutations) of all possible permutations.
Stratification for anticitrullinated protein antibody (ACPA)
Since patients with ACPAs have been found to have more severe radiological joint damage,18 we hypothesised an association between local joint inflammation and radiographic damage might only exist in ACPA-positive patients. Therefore, we added an interaction term between cumulative joint swelling and ACPA status. In case of a significant interaction, a stratified analysis was done.
Joint tenderness without joint swelling
We repeated the aforementioned analyses for joint tenderness in the absence of concurrent joint swelling. Here, the percentage of available visits at which a joint was tender but not concurrently swollen was used.
Inflammation occurring before or after joint damage development
To exclude the influence of joint inflammation occurring after the development of joint damage on the association, the original model was also repeated for the time period until joint damage was first observed.
To further study the possibility that an association between clinical inflammation and local damage is determined by joint swelling occurring after damage developed, we compared two multilevel mixed-effect logistic regression models (online supplemental data 1). With these models, we assessed whether baseline joint inflammation was more predictive of joint damage at the end of follow-up or vice versa (ie, baseline joint damage predicting for joint swelling during follow-up).
Supplemental material
Intermittent joint swelling episodes
We also investigated whether intermittent joint swelling, which is more likely to be a sign of synovitis than of other causes of swelling, was associated with joint damage progression (online supplemental data 1).
All analyses were performed in Stata V.SE16.
Results
Of the 473 patients with at least 1-year follow-up, 377 (80%) had any radiographic damage at the end of follow-up. The median patient-level Sharp van der Heijde score progression from baseline was 1.5 (IQR 0–8.25). Patient characteristics are described in online supplemental table 1.
Supplemental material
Of the 15 846 joints of the 473 included patients, 16% (2495) had radiographic joint damage (damage score ≥0.5) at the end of follow-up. Damaged joints had a mean±SD damage score of 2.5±3.5 (wrist excluded: 2.2±2.0). Median follow-up time was 41 (IQR 25–41) study visits (ie, 10 (IQR 6–10) years). Of the joints with damage at the end of follow-up, 46% (1141/2483) was swollen at baseline vs 35% (4725/13 316) of the joints without damage. The median percentage of visits at which joint swelling was observed was 6 (IQR 0–17) (ie, 2 (IQR 0–4) visits) for joints with damage and 3 (IQR 0–8) (ie, 1 (IQR 0–2) visit) for joints without damage. The time order of joint inflammation and joint damage (measured yearly) is described in figure 1.

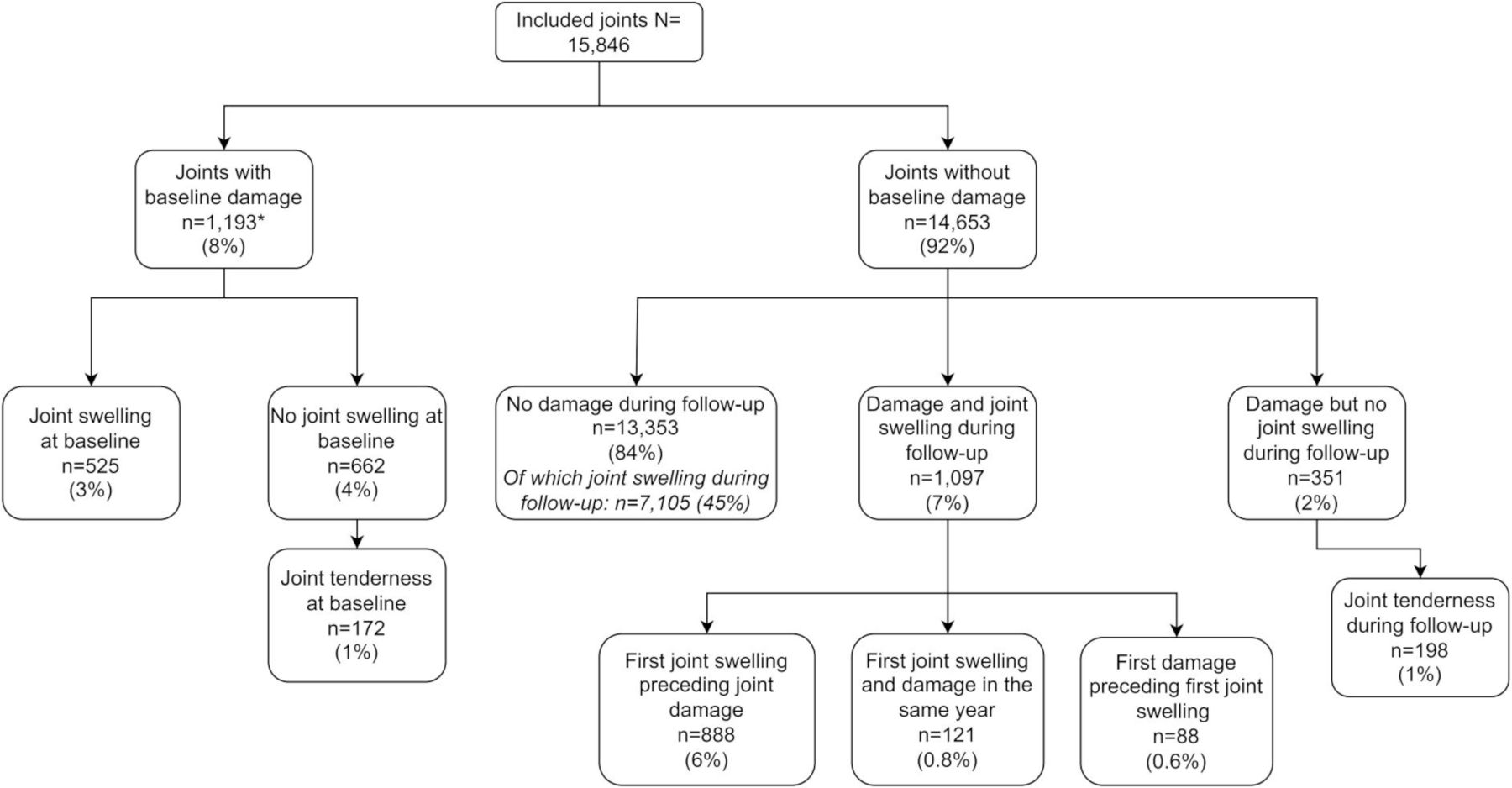{kind=link}
Time order of joint inflammation and damage development. * No baseline joint swelling assessment available for 6 joints.
Association between cumulative joint inflammation and radiographic joint damage
The percentage of visits at which a joint was swollen was associated with the degree of radiographic joint damage progression in the same joint (β=0.14, 95% CI 0.13 to 0.15); that is, for the average joint, the total damage score is 0.14% higher for each per cent increase in the number of study visits at which the joint was swollen. This corresponds to a 0.13 unit increase in total Sharp-van der Heijde score of a joint for each additional visit at which the joint was swollen.
The association between cumulative joint inflammation and radiographic damage was found for both joint space narrowing and erosions, with the strongest effect for joint space narrowing (table 1).
Association between cumulative joint swelling over time and local joint damage progression
When repeating the analyses in 10-year completers only, we confirmed an association between cumulative local joint swelling and local radiographic damage (β=0.25, 95% CI 0.23 to 0.26).
Stratification for the time periods baseline—year 2 and years 2—10 showed an association between cumulative joint swelling and joint damage in both time periods, with the strongest effect from year 2 to year 10 (table 1).
Effect of treatment strategy arm
Adding an interaction term between treatment strategy arm and cumulative joint swelling to the primary analysis showed a statistically significant interaction (p<0.001), indicating that the association between cumulative joint swelling and damage progression is different per treatment strategy. After stratification for treatment strategy arm, we found an association between cumulative joint swelling and local radiographic joint damage progression in all treatment arms. This association between joint swelling and damage was strongest in the methotrexate monotherapy arm and least strong in the combination therapy arm with initial infliximab (table 2).
Association between cumulative joint swelling over time and local joint damage progression stratified for treatment strategy arm
Analysing only joints that were swollen at least once confirmed that the association between joint inflammation and radiographic progression is dose dependent (table 1); that is, not only the fact that joints were inflamed but also the number of times they were inflamed is related to the degree of progression.
Local or general inflammatory effect
Adjustment of the primary analysis for DAS over time did not change the results. Furthermore, the permutation test showed that local joint damage progression was better predicted by the frequency of joint swelling of that joint than by joint swelling frequency of other joints (p<0.001, 95% CI 0 to 0.037). These results indicate a local, rather than a general, inflammation effect.
Stratification for ACPA
The ACPA-stratified analysis (interaction term p<0.001) showed an association between cumulative joint swelling and local joint damage progression for both ACPA-positive (172 patients, 5742 joints) and ACPA-negative patients (276 patients, 9280 joints), but the association was stronger in ACPA-positive patients (β=0.20, 95% CI 0.18 to 0.21, vs β=0.06, 95% CI 0.05 to 0.07).
Joint tenderness without joint swelling
The results for joint tenderness in the absence of concurrent joint swelling are shown in table 3. We did find an association between cumulative joint tenderness without joint swelling, but the effect sizes were smaller. The result of the permutation test (p<0.001, 95% CI 0 to 0.037) indicated that the association between joint tenderness and damage was a local effect as well.
Association between cumulative joint tenderness in the absence of joint swelling and local joint damage progression
Inflammation occurring before or after joint damage development
After exclusion of the time period after damage had developed, we still found an association between the frequency of joint swelling and joint damage (table 1). The association between baseline joint swelling and local joint damage at the end of follow-up was stronger than the association between baseline joint damage and the joint ever being swollen during follow-up (OR 1.39, 95% CI 1.30 to 1.49, vs OR 1.08, 95% CI 1.04 to 1.12), indicating that joint swelling preceding joint damage was more important for the association between joint inflammation and damage than joint damage preceding joint swelling.
Intermittent joint swelling episodes
We also found a positive association between the number of intermittent joint swelling episodes and local joint damage progression (β 1.10, 95% CI 1.03 to 1.18).
Discussion
In this post hoc analysis of the BeSt study in which patients with early RA were treated to target DAS of ≤2.4 for 10 years, we found a statistically significant association between the frequency of joint inflammation over time and local radiographic joint damage progression in the same joint. The mean damage score per joint at the end of follow-up was 0.41. On average, the joint damage score increased with 0.13 with each additional study visit at which joint swelling was observed. The association between cumulative inflammation and local joint damage was stronger for joint space narrowing than for erosions. Joint swelling was associated with local joint damage on short term (years 0–2) and even more on long term (years 2–10). We also found an association between joint tenderness (in absence of concurrent joint swelling) and damage progression, but this association was weaker.
Together, these results indicate that clinical joint inflammation has a cumulative and local effect on the extent of joint damage progression, both in early and longer existing disease, despite intensive targeted treatment.
Our finding that cumulative joint inflammation is associated with joint damage progression is in line with previous research, although to our knowledge this is the first study to assess the association of cumulative joint swelling (rather than only presence or absence of joint swelling) and local radiographic joint damage over a long time period. Previously, it has been described that both joint swelling and tenderness are associated with local radiographic damage after 1 year.7 8 19 However, for erosions, there are also studies reporting a weak or no association with joint inflammation.20 21 In these studies, the analyses were either at a patient level or at a joint level while not considering the dependency of different joints within one person. In our study, where we accounted for dependency of joints within patients, we did find an association between (cumulative) joint swelling and erosions on a joint level. The association was less strong than for joint space narrowing, although caution is needed when comparing results of different generalised mixed models. A possible explanation is that clinical joint inflammation is more associated with synovitis than with osteitis, which are assumed to be related to joint space narrowing and erosions, respectively.9 10
Previously, in participants of the BeSt study who were initially treated with infliximab, no association was found between joint swelling and radiographic joint damage progression after 1 year. Other studies have also described a disconnect between disease activity and radiographic damage progression in patients using tumour necrosis factor inhibitor therapy.22–24 Our results do not show a complete disconnect between inflammation and damage progression on long term in this patient group, although the association between inflammation and damage is less strong than in the other treatment arms. This despite the fact that infliximab was also a treatment option in the other treatment strategy arms (in case of insufficient disease activity suppression after previous treatment steps (number dependent on treatment arm)).25
Several studies have reported that joint swelling reflects synovitis better than joint tenderness does.15 16 However, since subclinical inflammation has been found to be associated with radiographic damage,26 we also analysed the association between cumulative tenderness in the absence of swelling and radiographic damage. Recently, it has been described that in joints that are tender but not swollen, the association between tenderness and synovitis depended on RA disease duration: only in patients with a disease duration of less than 2 years this association was statistically significant.13 The association between joint tenderness without swelling and radiographic damage progression might therefore also be absent later in the disease course. However, we found a comparable association between cumulative tenderness and damage progression both in the period from baseline to the second study year and from the second study year to the end of follow-up, although the associations were less strong than in the analyses for joint swelling.
One might argue that the association between cumulative joint inflammation and damage progression is determined by joint swelling and tenderness occurring after the development of damage. However, we also found the association after excluding the time period after damage development. Moreover, baseline joint swelling was more predictive for damage development than vice versa.
Strengths of our study are the frequent clinical and radiographic assessments, the long follow-up duration and the assessment of a local dose–response relationship between inflammation and radiographic damage. Clinical assessments every 3 months were carried out by dedicated personnel who were trained and retrained and who followed up the same patients for a long time period. Furthermore, we performed the analyses on a joint level, clustering joints within patients to account for the dependency of outcomes between joints of one patient. Apart from analysing the results on a joint level, we also performed extra analyses (adjustment for DAS and permutation tests) to indicate a local effect of joint inflammation and radiographic damage.
Our study also has some limitations. First, we only assessed hand and foot joints and can therefore not draw conclusions about the association between clinical inflammation and joint damage in other joints. Another limitation is that we could not compare one to one the results of the analysis of joint erosions and joint space narrowing. Nevertheless, we showed that for both types of joint damage, there was an association with cumulative joint inflammation. Another statistical challenge was the permutation test: in the original model, we adjusted for covariates, and with the permutation test, only one variable (cumulative joint inflammation) was permuted, resulting in an outcome (radiographic joint damage) that is adjusted for non-permuted covariates. However, when we did the permutation test for the univariable analysis and when we permuted the outcome instead of joint inflammation, we observed the same results. Furthermore, we cannot infer a causal effect of cumulative joint inflammation on local radiographic damage based on our analyses, although we did show that the association between them was at least partly determined by joint inflammation preceding joint damage. There was also no imaging available to assess inflammation, but joints were assessed clinically by trained personnel, and we showed that intermittent joint swelling episodes were associated with damage progression, more likely corresponding with synovial inflammation than other causes of joint swelling. Lastly, we did not replicate our findings in a population with more joint damage. However, the BeSt population reflects well the current treat-to-target situation in which radiographic joint damage is limited.
To conclude, we investigated local patterns of joint inflammation and radiographic joint damage and found that on both short and long terms, cumulative clinical joint inflammation, in particular joint swelling, is associated with local radiographic joint damage progression despite long-term intensive targeted treatment. Our results suggest that this is a local effect that is not sufficiently inhibited by targeted treatment, even though systemic inflammation is suppressed. The results also indicate that swollen and, to a lesser extent, tender joint counts are a valuable treatment target. Further research is needed to find new treatment strategies to further prevent joint damage. Furthermore, additional radiographic follow-up might be needed for joints with (frequent) clinical inflammation.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Medisch Ethische Toetsingscommissie Leiden (ID: P02.189). The participants gave informed consent to participate in the study before taking part.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors Concept and design and drafting of the manuscript: SLH, SAB and CFA. Acquisition of data: YPMG-R, MG-Y, WFL, MvO and TWJH. Analysis and interpretation: SLH, SAB, XMEM and CFA. Revised the manuscript critically and read and approved the final manuscript: all authors. Guarantors: SLH, SAB and CFA.
Funding The original BeSt study was funded by a research grant from the Dutch College of Health Insurances (OG 99-026) with additional funding from Schering-Plough BV and Centocor Inc. The authors, not the sponsors, were responsible for the study design, the collection, analyses and interpretation of all data, the writing of this article and the decision to publish.
Competing interests The original BeSt study was funded by a research grant from the Dutch College of Health Insurances (OG 99-026) with additional funding from Schering-Plough BV and Centocor. The authors, not the sponsors, were responsible for the study design, the collection, analyses and interpretation of all data, the writing of this article and the decision to publish.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.