Article Text

Abstract
Objectives Muscle soreness occurs after exercise and also in musculoskeletal diseases, such as fibromyalgia (FM). However, the nosography and pathoetiology of morbid soreness in FM remain unknown. This study aimed to investigate the morbid soreness of FM, evaluate its therapeutic responses and probe its pathophysiology with metabolomics profiling.
Methods Patients with newly diagnosed FM were prospectively recruited and completed self-report questionnaires pertaining to musculoskeletal symptoms. The phenotypes and metabotypes were assessed with variance, classification and correlation analyses.
Results Fifty-one patients and 41 healthy controls were included. Soreness symptoms were prevalent in FM individuals (92.2%). In terms of manifestations and metabolomic features, phenotypes diverged between patients with mixed pain and soreness symptoms (FM-PS) and those with pain dominant symptoms. Conventional treatment for FM did not ameliorate soreness severity despite its efficacy on pain. Moreover, despite the salient therapeutic efficacy on pain relief in FM-PS cases, conventional treatment did not improve their general disease severity. Metabolomics analyses suggested oxidative metabolism dysregulation in FM, and high malondialdehyde level indicated excessive oxidative stress in FM individuals as compared with controls (p=0.009). Contrary to exercise-induced soreness, lactate levels were significantly lower in FM individuals than controls, especially in FM-PS. Moreover, FM-PS cases exclusively featured increased malondialdehyde level (p=0.008) and a correlative trend between malondialdehyde expression and soreness intensity (r=0.337, p=0.086).
Conclusions Morbid soreness symptoms were prevalent in FM, with the presentation and therapeutic responses different from FM pain conditions. Oxidative stress rather than lactate accumulation involved phenotype modulation of the morbid soreness in FM.
Trial registration number NCT04832100.
- Fibromyalgia
- Outcome and Process Assessment
- Outcome Assessment
- Health Care
- Patient Reported Outcome Measures
Data availability statement
Data are available upon reasonable request. Raw and analysed data will be shared upon written request to the corresponding author from any qualified investigator.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- Fibromyalgia
- Outcome and Process Assessment
- Outcome Assessment
- Health Care
- Patient Reported Outcome Measures
WHAT IS ALREADY KNOWN ON THIS TOPIC
Soreness is a common somatic complaint of the musculoskeletal regions and negatively interferes with quality of life.
Whether soreness symptoms manifest in musculoskeletal pain disorders, such as fibromyalgia (FM), remains less investigated.
WHAT THIS STUDY ADDS
Morbid musculoskeletal soreness is prevalent in FM, with manifestations and clinical impacts different from pain.
Conventional treatment for pain control fails to alleviate soreness symptoms in FM despite its efficacy on pain.
Patients with FM with prominent soreness symptoms showed divergent phenotypes and metabotypes as compared with those without.
FM cases with prominent morbid soreness discomforts showed decreased plasma lactate but increased malondialdehyde levels.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Assessment of soreness symptoms in FM could provide valid approaches for phenotype classification, thereby benefiting disease evaluation and pathophysiology investigations.
Introduction
The International Association for the Study of Pain defines pain as “An unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage”.1 Relatively, soreness is another familiar somatosensation that predominantly occurs in the musculoskeletal regions.2 In most cases, soreness manifests after intense exercise and negatively interferes with daily activities.2–6 Acute-onset soreness after exercise is associated with acute lactate accumulation, and musculoskeletal micro-injury results in delayed onset muscle soreness (DOMS).2–6 Despite its common occurrence after physical activity, soreness sensation is not exclusive to exercise but also occurs in disease conditions not related to exertion or tissue damage, such as in fibromyalgia (FM).3 Currently, the prevalence and manifestations of morbid soreness symptoms in FM remain little surveyed3; furthermore, its underlying mechanism is largely unknown.
FM is a prevalent musculoskeletal disorder characterised by chronic widespread pain.7 8 Unlike other pain disorders (eg, low back pain and DOMS), the pathogenesis of FM does not involve muscular tissue injury or overexertion.7 Also, the widespread nature of musculoskeletal discomforts in FM defines the illness and differentiates it from other localised pain disorders.7–9 Apart from myalgia, patients with FM also have generalised morbid soreness without exercise or workout.3 The non-exertional soreness might interfere with quality of life and result in intolerance to rehabilitation or physical activity.3 10 11 Despite our comprehensive understanding of pain symptoms in FM, the soreness nosography in FM is less understood; furthermore, the clinical impact of soreness on the disease remains to be investigated.
Accordingly, we aimed to investigate the soreness nosography of FM and compare it with pain symptoms. We also probed the clinical impact of soreness symptoms and determined its response to current treatment. Additionally, we used metabolomics to explore the neurobiology of this morbid phenomenon and compared the metabolomic expression between FM groups of different soreness phenotypes. Understanding the nosography of non-exertional soreness in FM could help advance our understanding of the disease and design better therapeutic strategies.
Methods
Study participants
This prospective investigation was carried out in accordance with the Declaration of Helsinki. Adults with complaints of chronic diffused pain at the outpatient department of Kaohsiung Medical University Hospital were consecutively enrolled over a 2-year period from July 2017 to June 2019 (online supplemental figure S1). We also prospectively recruited age-matched and sex-matched healthy subjects without FM or other chronic musculoskeletal pain disorders as healthy controls (HCs). Written informed consent was obtained from all patients. Participants were interviewed by experienced neurologists (C-HH or K-WL), and those who fulfilled the 2011 American College of Rheumatology criteria for FM were recruited.12 To investigate the manifestations and metabolomic phenotypes without pharmacological intervention, we recruited only patients with newly diagnosed primary FM before initiation of pharmacotherapy. None of the participants were under treatment with antidepressants, antiepileptic or antipsychotic drugs. Also, to avoid the metabolomic interference resulting from other medical conditions (eg, comorbid autoimmune diseases), only patients with primary FM were recruited for an adequate comparison.
Supplemental material

Non-exertional soreness in patients with FM and characterisation of phenotypes by soreness assessments. (A) Prevalence of pain and soreness symptoms in FM. (B) Distribution of pain and soreness symptoms in the body (χ2 test). (C) Correlation analysis of pain and soreness manifestations in given body regions (Pearson correlation test). Pearson correlation coefficients are labelled in each area. For detailed statistical values, refer to online supplemental table S1. (D) Correlation between intensity and diffuseness in pain (left) and soreness (right) symptoms. (E) Left, correlation between WPI and WSI in FM. Right, correlation between NRS-P and NRS-S in FM. (F) Principal component analysis score plot for patients with FM-P and patients with FM-PS based on WPI, WSI, NRS-P and NRS-S. (G, H) Symptom severity of pain (G) and soreness (H) in FM-P and FM-PS (unpaired t-test). (I, J) Effect of current treatment on (I) pain intensity (NRS-P, left) and diffuseness (WPI, right) and (J) soreness intensity (NRS-S, left) and diffuseness (WSI, right) in FM-P and FM-PS (two-way analysis of variance). B, basal status; FM, fibromyalgia; FM-P, fibromyalgia with pain dominant symptoms; FM-PS, fibromyalgia with mixed pain and soreness symptoms; NRS-P, Numerical Rating Scale for Pain; NRS-S, Numerical Rating Scale for Soreness; PCA, principal component analysis; wk, week; WPI, Widespread Pain Index; WSI, Widespread Soreness Index. Values are mean±SD. The resulting p values for the comparison of pain/soreness severity and diffuseness (I and J) symptoms were adjusted by the Bonferroni correction, with p <0.0125 considered statistically significant. *p<0.05, **p<0.01, ***p<0.001 correlation between pain and soreness (C), comparison between groups (G and H) or comparisons with B (I and J; Dunnett’s post-hoc test). ###p<0.001 compared with the other group at each time point (I and J: Dunnett’s post-hoc test). ns, not significant.
Study design
The demographic and clinical data for patients and controls were obtained by questionnaires and interviews with the same specialist throughout the study. Patients were asked to assess their muscular discomforts in terms of pain and soreness separately. The intensity and diffuseness of pain symptoms were assessed with a Numeric Rating Scale for Pain (NRS-P; 0–10) and Widespread Pain Index (WPI; based on the American College of Rheumatology criteria). By analogy to the NRS-P and WPI, participants were asked to rate their soreness severity and report the distribution of soreness symptoms with the NRS for Soreness (NRS-S) and Widespread Soreness Index (WSI) to evaluate soreness symptoms of FM.13 The WSI questionnaire is based on the WPI design and comprises a list of 19 areas for soreness assessment, and patients mark the number of body parts where they have experienced soreness symptoms during the last week (online supplemental figure S2). Participants were asked to report their soreness and pain symptoms respectively. The Revised Fibromyalgia Impact Questionnaire (FIQR) was used to investigate the impact of musculoskeletal symptoms on disease severity and functional capacity.14 The questionnaire consists of 21 individual questions across three linked components, including function (domain 1 of FIQR), overall impact (domain 2) and symptoms (domain 3). Both patients and HCs were asked to report their musculoskeletal symptoms in a week and complete FIQR.

Metabolomic profiling in FM and comparison between subgroups of FM. Peak intensity expression of metabolites (A) upregulated and (B) downregulated in patients with FM versus HCs. (C) Heatmap of metabolomic differences between FM-P, FM-PS and HC groups. Individual samples (horizontal axis) and significantly dysregulated metabolites (four upregulated and seven downregulated; vertical axis) were separated by hierarchical clustering (Ward’s algorithm), with the dendrogram scaled to represent the distance between each branch (distance measure: Euclidean correlation). The heatmap displays a relative increase in expression of each metabolite in red and a decrease in blue. (D) Heatmap of group-averaged metabolomic differences between FM-P, FM-PS and HC groups. FM, fibromyalgia; FM-P, fibromyalgia with pain dominant symptoms; FM-PS, fibromyalgia with mixed pain and soreness symptoms; HCs, healthy controls; AMP, adenosine monophosphate. *p<0.05, **p<0.01, ***p<0.001 compared with HCs (Kruskal-Wallis Test).
Patients underwent three evaluations were conducted to assess clinical manifestations and therapeutic responses, including the initial interview and two scheduled follow-ups at 2 and 4 weeks (online supplemental figure S1). At the first visit, a comprehensive interview and the FIQR were administered, and laboratory tests were performed. Pharmacotherapy was initiated at the first visit and adjusted with a stepwise approach according to the individual conditions, with monotherapy with imipramine being used in the initial encounter for all patients. The first follow-up was arranged 2 weeks later, and therapeutic responses were assessed and reported by patients. Monotherapy with imipramine was retained for patients who reported satisfactory control of symptoms. For patients who reported poor therapeutic response but refused the dosage increase because of drug intolerance, pregabalin was added as combination therapy. The second follow-up was arranged 2 weeks later, and therapeutic responses of patients were recorded again. No non-steroidal anti-inflammatory drugs, morphine or opioid-analogue drugs were used for pain control during follow-up. HCs underwent a single interview without follow-up or pharmacal intervention.
Statistical analysis
Clinical data
Data are expressed as mean±SD. Sample size was calculated with use of G* Power V.3.1.9.2, with α=0.05 significance level and 80% power (β=0.20). The determination of effect size was based on previous literature and power analysis,15 16 and the optimal sample size for each group was at least 20 given the aforementioned information. Two-tailed p<0.05 was considered statistically significant in all tests. SPSS V.20 was used for analysis. We performed the Shapiro-Wilk test to check the normality of data before examining the difference between groups, with the data being found normally distributed with p value >0.05 overall. Differences between groups were assessed with Student’s t-test or one-way analysis of variance (ANOVA) as appropriate. The changes before and after treatment were compared by ANOVA. Resulting p values for the comparison of clinical outcomes were adjusted by the Bonferroni correction. Pearson correlation was used to assess the correlation between parameters.
To explore any phenotypic differences among patients in terms of musculoskeletal symptoms, cluster analysis was used to identify distinct groups of patients with FM based on manifestations of pain and soreness severity (NRS-P, NRS-S, WPI and WSI). The k-means clustering algorithm was used and patients with similar manifestations were classified into two meaningful subgroups. Principal component analysis (PCA) was used to explore the intrinsic clustering and relevant subgroups of patients from unlabeled data.
Metabolomics data
The statistical information of metabolomics is described in detail in the online supplemental material 1.
Results
Non-exertional soreness is prevalent in FM
We enrolled 51 patients with newly diagnosed FM and 41 HCs for the final analysis (online supplemental figure S1). Demographic data and symptom assessments are summarised in table 1. Soreness complaints were highly prevalent (92.2%) in FM individuals, along with pain (100%) (figure 1A). In comparison, five cases of HCs reported pain symptoms (12.2%) and five reported soreness (12.2%). No patient with FM reported physical exertional events within 2 weeks. Most of the recruited patients (49 of 51 cases; 96.1%) received combination therapy of tricyclic antidepressant and pregabalin (online supplemental figure S1). Patients with FM were intolerant of daily activities as assessed by domain 1 of FIQR (table 1). The distribution of pain and soreness symptoms did not differ among body regions in general (figure 1B); notably, the distribution of pain symptoms was not related to that of soreness (figure 1C; online supplemental table S1). The soreness intensity score (NRS-S) was moderately correlated with soreness diffuseness (WSI; r=0.576, p<0.001), with no correlation between pain intensity score (NRS-P) and pain diffuseness (WPI) (figure 1D). We also found a modest correlation between pain and soreness intensity (r=0.302, p=0.031) but not diffuseness (r=0.061, p=0.670) (figure 1E).
A comparison of demographic data and clinical manifestation between patients with fibromyalgia and healthy controls
Next, we evaluated the clinical correlation of pain/soreness intensity (NRS-P and NRS-S scores) and FIQR (disease severity) scores (online supplemental table S2). Pain intensity was significantly correlated with FIQR score (r=0.434, p=0.001) but not soreness intensity (r=0.216, p=0.128). Participants with high pain intensity reported high disease impact on their life (domain 2) and complained of worse FM symptoms (domain 3). They also reported worse conditions of fatigue, skin allodynia and insomnia. In comparison, high soreness intensity was correlated with intolerance to static activity (sitting for 45 min; r=0.425, p=0.002) and high stiffness levels (r=0.317, p=0.023). Conventional therapies reduced pain scores significantly in 4 weeks (NRS-P from 6.96 to 4.88; p<0.001), but with no significant improvement in soreness (NRS-S from 5.67 to 4.33; p=0.024, p value being adjusted by Bonferroni correction with <0.0125 considered statistically significant) (online supplemental table S3). Also, 23 patients (45.1%) achieved ≥30% pain reduction after treatment, and 20 patients (39.2%) achieved ≥30% soreness reduction. Also, the treatment effectively relieved disease severity as assessed by the FIQR (from 53.66 to 41.93; p=0.012).
Assessments of non-exertional soreness allow for characterising phenotypes in FM
The k-means clustering algorithm classified patients with similar musculoskeletal symptoms into two meaningful groups. Unsupervised PCA revealed intrinsic clusters of two subgroups (figure 1F). Both groups of patients reported similar pain scores (NRS-S=7.15±2.14 vs 6.71±2.93; p=0.540) and diffuseness (WPI=8.96±4.54 vs 9.96±4.71; p=0.446), whereas 27 patients (52.9%) reported significantly prominent soreness intensity (7.19±1.98 vs 3.96±2.79) and diffuseness (10.96±3.41 vs 2.79±2.32) than the others (both p<0.001; online supplemental table S4). Therefore, these patients with salient soreness symptoms in addition to pain were designated as the group of mixed pain and soreness symptoms (FM-PS). On the other hand, those patients without or with minor soreness symptoms were designated as the group of pain dominant symptoms (FM-P).
The mean age was lower for FM-PS than patients with FM-P, with no difference in sex ratio (online supplemental table S4). Symptom severity and FIQR scores did not significantly differ between the groups. The two groups had comparable distribution of pain symptoms, but soreness symptoms were significantly greater in FM-PS than FM-P in all body regions (online supplemental table S5). The correlation of pain and soreness distribution in the body regions was in general unremarkable in both groups (online supplemental tables S6 and S7). In the FM-PS group, WPI and WSI scores were significantly correlated (p=0.039), as were NRS-S and NRS-P scores (p<0.001), with no correlation among scores in the FM-P group (online supplemental figure S3).

{kind=link}
{kind=link}
{kind=link}
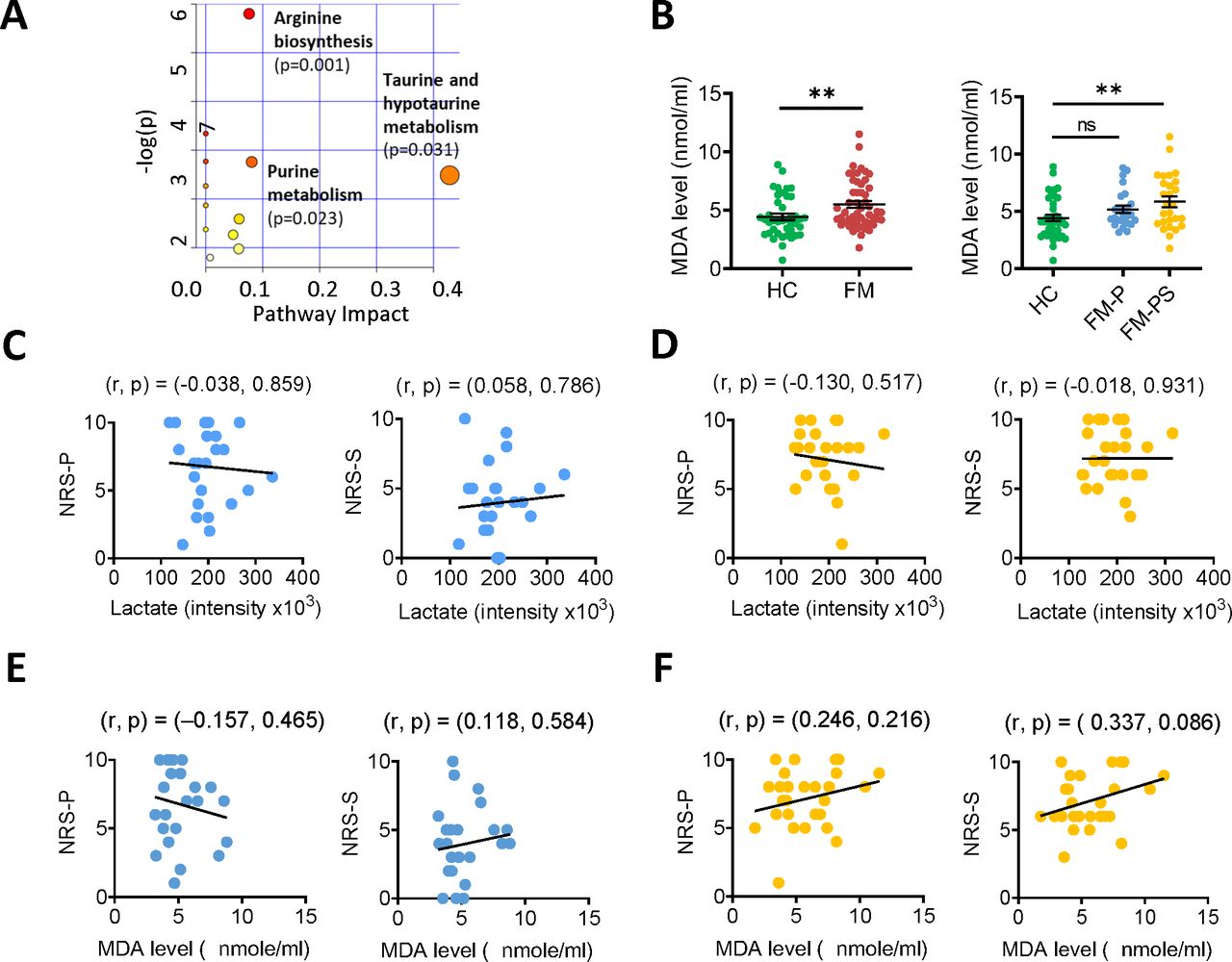
Metabolic pathway analysis and oxidative stress status in patients with FM. (A) Summary of pathway analysis visualised by bubble plots. For biologically meaningful pathways selected by pathway analysis and the involved metabolites, please refer to online supplemental figure S6. (B) Plasma malondialdehyde (MDA) level assayed by the thiobarbituric acid reactive substance method in patients with FM versus HCs. Left, comparison between FM and HC groups (unpaired t-test). Right, comparison among FM-P, FM-PS and HC groups (one-way analysis of variance). (C, D) Correlation analysis of plasma expression of lactate with NRS-P (left) and NRS-S (right) in FM-P (C) and FM-PS (D) (Spearman’s correlation test). (E, F) Correlation analysis of plasma MDA levels with NRS-P (left) and NRS-S (right) in FM-P (E) and FM-PS (F) (Spearman’s correlation test). **p<0.01, ***p<0.001 compared with HCs. FM, fibromyalgia; FM-P, fibromyalgia with pain dominant symptoms; FM-PS, fibromyalgia with mixed pain and soreness symptoms; HCs, healthy controls; NRS-P, Numerical Rating Scale for Pain; NRS-S, Numerical Rating Scale for Soreness.
For patients with FM-P, high pain intensity was positively correlated with high levels of fatigue, insomnia, allodynia and overall domain 3 scores (online supplemental table S8). Similarly, high pain intensity was positively correlated with high overall FIQR scores in FM-PS. Notably, in both groups, patients with high soreness severity tended to manifest restless conditions (intolerance of sitting for 45 min).
Pharmacotherapies effectively alleviated pain symptoms in both groups (figure 1I). For soreness, the current treatment timely reduced soreness intensity (NRS-S) in FM-P within 2 weeks, but no therapeutic response was noticed in FM-PS until 4 weeks after treatment (figure 1J). Although conventional pharmacotherapies successfully reduced both soreness intensity and diffuseness in the FM-PS group 4 weeks later, NRS-S and WSI scores remained significantly higher in the FM-PS (5.59±2.72 and 8.26±4.44) than the FM-P group (2.83±2.32 and 2.54±2.41) even after 4 weeks of treatment (figure 1J). Moreover, current treatment significantly improved overall symptom severity and disease impacts for patients with FM-P but not patients with FM-PS (online supplemental table S9).
Metabolomic differentials among patients with FM with and without prominent soreness
To probe the metabolic features of FM, we used untargeted metabolomics analysis of plasma samples from participants with use of MetaboAnalyst.17 Unsupervised PCA revealed no clear separation between FM and HC groups (online supplemental figure S4A). Another score plot was constructed to explore any metabolic differences between FM cases with and without prominent non-exertional soreness but still showed no distinct separation between the FM subgroups (online supplemental figure S4B).
Next, we used fold-change analysis to compare the peak intensity expression of metabolites between FM and HC groups. Metabolites with significant dysregulation in FM versus HCs are listed in online supplemental table S10. To probe any metabolomic phenotypes in FM cases, we further compared the expression of the identified metabolites in FM-P and FM-PS groups (figure 2A,B). Except for N6-acetyl-l-lysine, the levels of upregulated metabolites were prominently higher in the FM-PS but not FM-P group than HCs (figure 2A). Also, we observed incremental expression gradients for all metabolites among HC, FM-P and FM-PS groups in that order. Likewise, for downregulated metabolites, the peak intensity was significantly lower for patients with FM-PS than HCs (figure 2B). We observed decreased expression gradients for metabolites among HC, FM-P and FM-PS groups in a similar order.
We then used supervised sparse partial least squares discriminant analysis (sPLS-DA) to identify the discriminative metabolites for FM (online supplemental file 1). Most of the top 10 discriminative features selected by the sPLS-DA model based on loading values for component 1 were also the dysregulated metabolites recognised by the fold-change analysis, which correspondingly underpinned the selection by sPLS-DA as consistent markers. Next, we repeated sPLS-DA for FM-P, FM-PS and HC groups (online supplemental figure S5B). Similarly, the top discriminative features selected by the sPLS-DA model based on component 1 loading values were mostly the altered metabolites recognised by the fold-change analysis. Of note, the top 10 selected features identically predicted FM-PS or HC groups but not the FM-P group, which suggested metabolomic differentials predominantly existed between FM-PS and HC but not FM-P and HC groups. To visualise the potential discrepancy among the groups, we constructed a heatmap of the 11 significantly dysregulated metabolites with hierarchical clustering (figure 2C). FM-PS and HC groups had an almost opposite expression of the selected metabolites except for N6-acetyl-l-lysine, whereas the FM-P group showed intermediate expression between FM-PS and HC groups (figure 2D).
Pathway analysis was used to identify the biologically meaningful pathways relevant to FM. To identify the most biologically meaningful patterns, only metabolites with incremental changes >2 or decremental changes <0.5 were used for further analysis. The impact value calculated from topology analysis and −log(p) were used to evaluate the importance of the pathways related to FM. The threshold of impact value was set at 0.05, and pathways with statistical significance and values above the threshold were filtered out as potential pathway targets (figure 3A; online supplemental table S11). We identified three biologically significant pathways related to FM (taurine metabolism, purine metabolism and arginine biosynthesis), and five metabolites involved in the pathways (taurine, L-arginine, 2-oxoglutarate, hypoxanthine and adenosine monophosphate) (online supplemental figure S6).
Mounting evidence indicates that the pathophysiology of FM is associated with oxidative stress.18–22 Previous reports indicated higher oxidative status for FM individuals than controls, and the oxidative stress loading of FM individuals could be correlated with disease severity.20 23 In our study, two of the three identified pathways from pathway analysis are known to be associated with cellular oxidative metabolism, including purine metabolism and arginine biosynthesis. To explore whether excessive oxidative stress exists in FM, we evaluated oxidative stress by assessing plasma levels of lipid peroxidation as determined by malondialdehyde (MDA) level.20 23 The significantly higher MDA level in patients with FM than HCs suggested higher oxidative stress loading in FM individuals (p=0.009; figure 3B). Of note, MDA level was significantly higher in the FM-PS than HC group (p=0.008), with no significant difference between FM-P and HC groups (p=0.229; figure 3B), which suggests excessive oxidative stress with FM-PS but not FM-P. To probe the FM soreness mechanism and make a comparison with exercise-related soreness, we used correlation analyses of plasma lactate expression and soreness intensity between groups, but no correlation was noticed (figure 3C,D). Given that patients with FM-PS had prominent soreness symptoms with simultaneously higher oxidative stress, we next explored the correlation between soreness intensity and MDA level in FM subgroups (figure 3E,F). We identified a correlative trend, although statistically non-significant, in FM-PS versus FM-P groups, which suggest that oxidative stress or other oxidised metabolites might modulate the non-exertional soreness phenotype in FM.
Discussion
Our investigations revealed that morbid soreness symptoms were prevalent in FM. As compared with exercise-related soreness, several characteristics of the non-exertional soreness in FM were identified in terms of clinical manifestations, distribution and metabolomic features6 24 (table 2). Additionally, phenotypes, therapeutic responses and metabotypes distinctly differed between patients with FM with different severity of soreness symptoms (online supplemental table S12). Of note, the morbid soreness phenotypes in FM did not involve lactate accumulation but might be associated with excessive oxidative stress.
A comparison between non-exertional and exertional soreness
Muscle soreness results in intolerance to daily activity and thus hinders individuals from daily activities or rehabilitation.6 In research of soreness, post-exercise soreness is mostly investigated, including acute post-exercise soreness and DOMS.6 The morbid soreness in FM shows several similarities as post-exercise conditions. First, both conditions show significant correlations of soreness and pain intensity.2 25 Moreover, post-exercise soreness limits range of motion and results in stiffness.26–28 Similarly, soreness intensity and stiffness severity were positively correlated in FM.
However, several divergences exist as well (table 2). Unlike in DOMS, the symptoms of FM do not involve tissue inflammation or mechanical insults.2 8 29 Also, post-exercise soreness is a transient physiological response to exercise, whereas FM is a chronic pain condition resulting from aberrant central sensitization.2 5 8 Additionally, we found no spatial correlation of pain and soreness symptoms in the affected regions of FM (figure 1C), which is quite different from the concordant manifestations of pain and soreness in the post-exercise conditions.6 29 In this sense, the investigations of non-exertional soreness in FM might provide a unique approach to probe the soreness nosography that previous DOMS research have not provided.2 4 29 30
Lactate accumulation in muscles is commonly thought to be associated with acute soreness after exercise.29 31 However, our investigation did not suggest upregulated lactate expression in FM individuals as compared with HCs. On the contrary, lactate expression was even lower in FM individuals with prominent soreness symptoms (FM-PS). Thus, the morbid soreness in FM may not involve lactate production, and the soreness mechanisms might differ from those in exercise conditions. Of note, oxidative status was significantly increased in patients with FM-PS (figure 3B). In this context, the soreness symptoms in FM may not result from lactate accumulation but might involve other factors related to oxidative stress, such as oxidised products of lipids (eg, lysophosphatidylcholine) or proteins (eg, protein carbonyls).32 33 Notably, for exertional soreness, antioxidants have been proposed to treat post-exercise soreness by reducing free radical generation during exercise.24 34 However, a recent systematic review did not strongly support the therapeutic efficacy on exertional soreness.35 Because of the excessive oxidative stress in FM and its correlation with soreness, antioxidants might be of potential therapeutic use to relieve the non-exertional soreness of FM, especially considering that current treatment cannot ameliorate soreness symptoms effectively in FM.
Patients with higher soreness intensity had more difficulty sitting still for 45 min (online supplemental tables S2 and S8). The restless conditions are reminiscent of the core feature of restless leg syndrome (RLS), another common comorbidity of FM.36 37 Up to one-third of patients with FM have reported comorbid RLS symptoms. Coincidentally, soreness sensation is also a prevalent descriptor of RLS discomfort (40.4%).38 So far, the clinical or pathophysiological associations among non-exertional soreness, RLS and FM remains undetermined. Future study is necessary to investigate the prevalence and clinicoetiologic correlates of these two disorders with focus on soreness manifestations.
FM is considered a heterogenous condition.8 We found distinct phenotypic differences between FM-P and FM-PS in terms of clinical presentation, therapeutic responses, metabolomic expression and oxidative stress status (online supplemental table S12). We found significant positive correlations between pain and soreness symptoms in FM-PS, with no similar findings for FM-P (online supplemental figure S3A,B). Additionally, the impact of pain symptoms on the FM comorbidities was evident in FM-P but not FM-PS (online supplemental table S8). Moreover, we found remarkable differences in therapeutic responses in pain and soreness symptoms between the two groups (figure 1I,J). Despite improvements of pain scores in both groups, current treatment improved overall symptom severity and disease impacts (FIQR domain 2) for patients with FM-P but not patients with FM-PS (online supplemental table S9). Such a discrepancy of outcome might result from the unsatisfactory relief of soreness symptoms in FM-PS. For pain control, conventional treatment improved pain scores in both groups and no significant difference of pain scores existed between two groups after 4 weeks of treatment. For soreness control, although pharmacotherapies reduced soreness severity in the FM-PS group with statistical significance, their NRS-S scores remained significantly higher than those in the FM-P group. Compared with the mild soreness symptoms in the FM-P group (NRS-S=2.83±2.32), patients with FM-PS still reported moderate soreness intensity (NRS-S=5.59±2.72) after treatment (figure 1J). Accordingly, soreness reduction might be a key factor in improving the disease severity for patients with FM-PS. So far, the therapeutic approaches for morbid soreness in FM remain lacking. In physical conditions, non-steroidal anti-inflammatory drugs relieve exercise-induced soreness2 29; however, their therapeutic effects for the morbid soreness of FM remain unknown. Further studies are needed to identify candidate therapies and develop appropriate therapeutic strategies, especially for patients with prominent soreness complaints.
We identified metabolomic differences between FM-P and FM-PS. The fold change analyses (figure 1A,B), sPLS-DA (online supplemental figure S5B) and metabolomic heatmap (figure 2C,D) findings all suggest a more distinct metabolomic expression in FM-PS than FM-P versus HCs. Along with the findings of clinical manifestations, the evaluation of soreness in FM provides an easy approach to identify FM phenotypes, thereby benefiting patient classification and better therapeutic strategies.
In addition to lactate, several metabolites are dysregulated in FM. Among the five metabolites identified by the pathway analysis, hypoxanthine, L-arginine and 2-oxoglutarate participate in oxidative stress generation and were downregulated concordantly. All three substances can function as source materials to produce endogenous oxidative and nitrosative stress. Hypoxanthine is the breakdown product of purine metabolism and functions as a material for a conversion that produces superoxide (O2—·) and hydrogen peroxide in the presence of xanthine oxidase.39 40 Also, L-arginine is converted by nitic oxide synthase into citrulline and nitric oxide, which induces nitrative and oxidative stress.32 41 Furthermore, ROS can be generated from 2-oxoglutarate via 2-oxoglutarate dehydrogenase catalyzation in the Krebs cycle.42–44 From these perspectives, the decreased levels of these metabolites might be associated with material consumption for ROS generation, which suggests increased oxidative stress in organisms. This assumption was further validated by the elevated plasma MDA level in FM, as numerous studies have previously reported.19 20 32 Of note, the expression of altered metabolites and MDA level was significantly increased in FM-PS, which implies that the oxidative status might participate in modulating the soreness phenotype in FM. Further research is needed to clarify the potential relationship and underlying mechanisms.
Despite its undetermined aetiology, FM is believed to be associated with aberrant central amplification of nociceptive signalling. Although the investigation of central mechanisms is beyond the scope of this work, our study pointed out a potential link between morbid soreness and central sensitisation based on our metabolomic findings and previous translational research.22 Our prior study found that certain oxidised lipids (eg, lysophosphatidylcholine) can cause chronic hyperalgesic changes in mice by activating acid-sensing ion channel 3 after psychological stress exposure. Thus, the oxidised metabolites likely function as a nociceptive ligand and subsequently trigger central sensitisation to cause FM symptoms. Of note, the current investigation also revealed excessive oxidative stress and lipid oxidisation in FM individuals, especially in FM-PS. Additionally, it identified a correlative trend between MDA levels and soreness severity. Therefore, the morbid soreness of FM might relate to oxidative stress and involve a similar process of central sensitisation as the development of pain.
Recent research has shown the evidence of increased muscle pressure and altered microcirculation in patients with FM.45 It is likely that microcirculation insufficiency secondary to intramuscular pressure could lead to ischaemic changes and oxidative stress. This condition might cause tissue acidosis, thus contributing to generation of subsequent soreness, especially in consideration of the hypoxic metabolite expression in the FM-PS cases and its correlation with soreness.3 The concept of sngception has been recently proposed to describe this distinct sensory modality of acid-related soreness.3 From this perspective, the microcirculation caused by muscle compression might involve the development of soreness phenotype. Also, the situation could be more severe in FM cases with prominent soreness. In this sense, attempts at improving oxygenation of muscle and looking at markers of oxidative metabolism might be helpful in understanding and treating FM. Additionally, one can also assume that antioxidants can be used as a therapeutic method for soreness discomfort. Currently, numerous types of antioxidants have been tried in treating post-exercise soreness as well as FM discomfort.35 46 47 Among these, vitamins C, E and co-enzyme Q10 might be the most investigated agents. Despite some positive findings in the literature, the benefits of antioxidants on FM symptoms remains to be further validated.
At present, the data of FM soreness investigations remain limited in the literature. This phenomenon might result from the fact that soreness sensation accompanying myalgia can be overwhelmed by co-existing pain perception, thus making the impact of soreness less concerned. Our previous study has dedicated to establishing the soreness assessments in FM with self-report NRS-S.13 In the literature, a qualitative analysis of FM documented the soreness manifestations individually and compared the intensity of pain and soreness.48 Additionally, a few quantitative studies have mentioned the features of soreness phenotypic changes under medical intervention; patients with FM were likely to experience significantly higher soreness severity after trigger point drug injection and prone to sustaining soreness discomforts after fitness test.49 50 However, the information of soreness nosography in FM remains substantially insufficient, so we conducted the current study to this end.
In this study, the classification of phenotypes drastically relied on the self-assessment of soreness symptoms. Similar to pain, soreness is a subjective sensation, and its assessment could be influenced by individual differences, such as symptom definition, familiarity of assessment and even situational factors. Therapeutic intervention is another important influencing factor for symptom rating. Although perceptual differences might exist among individuals, the appraisal and interpretation of soreness symptoms should be identical within individuals. Our previous study investigated the assessments of FM soreness with self-report questionnaire and showed good test–retest reliability of soreness rating in patients with FM with a follow-up manner,13 implying that the self-rating manner was a reliable approach of assessing soreness. Additionally, in this study, we only recruited newly diagnosed patients with FM into analysis to avoid pharmacotherapeutic interference in the observations. In this setting, our observations may provide a valuable window to investigate the original FM phenotypes and thus help with better understanding its nosography.
This study has several limitations. First, the sample size might not adequately represent the general population. Also, combining pharmacotherapies of imipramine and pregabalin with individual adjustment were used to relieve symptoms. Ideally, monotherapy would be better for evaluation of therapeutic effects; however, this therapeutic approach is intrinsically limited by its analgesic efficacy or dose-limiting side effects, or both. Additionally, the need for individual drug adjustment would be an intrinsic limitation in the study. Moreover, the observational timeframe of therapeutic responses might be too short for appropriate assessments. Further studies with a monotherapy design and longer follow-up are needed for better evaluation of therapeutic responses and prognosis. Nevertheless, this study provides evidence for FM heterogeneity between cases with and without prominent soreness manifestations in terms of clinical phenotypes and metabotypes. In comparison with exercise-induced soreness, the morbid soreness in FM does not involve lactate accumulation but tends to associate with excessive oxidative stress. Assessments of morbid soreness in FM could provide a valid strategy to easily recognise disease phenotypes of FM, thereby benefitting clinical practice and therapeutic approaches.
Data availability statement
Data are available upon reasonable request. Raw and analysed data will be shared upon written request to the corresponding author from any qualified investigator.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by the institutional review board of Kaohsiung Medical University Hospital (KMUH), Taiwan (KMUHIRB-(I)-20170012). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We thank the Metabolomics Core Laboratory at the Center of Genomic Medicine of National Taiwan University and National Pingtung University of Science and Technology for their assistance in performing metabolomics experiments.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors C-HH, C-LL and C-CC designed research. C-HH and C-CC processed funding acquisition. C-HH, K-WL and Y-OF contributed to patient recruitment. C-HH, D-SH, M-HT and P-SW contributed to methodology and data for metabolomics analysis. C-YH, C-LL and C-HL contributed to critical revision of manuscript. F-WL contributed to statistical methods. C-CC is the guarantor of the study.
Funding This work was supported by intramural funding from the Ministry of Science and Technology (Taiwan) and Kaohsiung Medical University Hospital (MOST 109-2628-B-037-008, MOST 110-2628-B-037-016, NPUST-KMU-110-P009, KMUH109-9R71 and KMUH110-0R64 to C-HH; MOST 110-2321-B-001-010 and MOST 111-2321-B-001-009 to C-CC).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.