Article Text

Abstract
Background/purpose The manifestations of uveitis are well established in axial spondyloarthritis (ax-SpA), but not in psoriatic arthritis (PsA). We aimed to assess, in a large unselected series of PsA: (A) the frequency and clinical features of uveitis; (B) its association with PsA activity, the impact of disease and functional disability, and (C) its relationship with the biological treatment. In addition, a literature review was performed.
Methods Retrospective longitudinal study of PsA patients from a single referral hospital. PsA was classified according to the CASPAR criteria, and uveitis was diagnosed by experienced ophthalmologists.
Results We studied 406 patients with PsA (46.3±12.3 years). Uveitis was observed in 20 (4.9%). Uveitis was acute in all cases, anterior (80%), unilateral (80%) and recurrent (50%). Patients with uveitis had a higher prevalence of HLA-B27 (45% vs 7.5%, p<0.0001), sacroiliitis on MRI (25% vs 8.3% p=0.027), ocular surface pathology (10% vs 0.8%, p=0.021), and median PsA impact of Disease Score (5.9 (2.1–6.8) vs 1.25 (0.0–3.0), p=0.001) and Bath Ankylosing Spondylitis Functional Index (4 (1.6–5) vs 1.0 (0.0–3.5), p=0.01) than patients without uveitis.
The exposure adjusted incidence rate (episodes/100 patients-year) of uveitis before versus after biological treatment decreased with anti-TNFα monoclonal antibodies (56.3 vs 9.4) and increased with etanercept (ETN) (6.03 vs 24.2) and secukinumab (SECU) (0 vs 50) (including only one patient treated in the last two cases).
Conclusion The prevalence of uveitis in patients with PsA was about 5%. The pattern was similar to that observed in ax-SpA. Uveitis was associated with a worse quality of life and greater functional disability. The uveitis exposure adjusted incidence rate decreased with anti-TNFα monoclonal antibodies and increased with ETN and SECU.
- Psoriatic Arthritis
- Spondylitis, Ankylosing
- Biological Therapy
Data availability statement
No data are available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Several studies have analysed the frequency of uveitis in spondylarthritis (SpA) and its relationship with biological therapy. However, studies specifically focused on psoriatic arthritis (PsA) and uveitis are scarce, and the frequency as well as the relationship with biological therapy is not well established.
WHAT THIS STUDY ADDS
This study provides real-world clinical data on the epidemiology and clinical features of PsA-related uveitis, and its relationship with biological therapy.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
We can recognise the clinical characteristics of uveitis in PsA as well as the appropiate biological therapy for treatment.
Introduction
Ocular involvement is a typical extraarticular manifestation of spondylarthritis (SpA), including psoriatic arthritis (PsA).1–4 Uveitis is the most common ocular complication of SpA and may be a potentially sight-threatening complication.1 2 In addition, SpA-related uveitis has been described as a poor prognostic marker since it is associated with increased disease activity.4
Data on epidemiology, clinical pattern and therapeutic scheme of PsA-related uveitis widely differ across studies. Thus, the prevalence of uveitis in PsA ranges from 7% to 18%,3 5–8 lower than 20%–40% described in ankylosing spondylitis (AS).3 Uveitis in PsA is predominantly anterior although it can also have posterior involvement, bilateral, and with an insidious onset and chronic course,9 10 while it is usually anterior, unilateral and with a sudden onset and relapsing course in patients with AS.3 4
Several studies have analysed the relationship between uveitis and psoriasis1 11–13 as well as AS.14–17 However, studies specifically focused on the clinical features of PsA-related uveitis are scarce and based on small or selected series of patients.5–9 On the other hand, in most of them, the relationship of uveitis with PsA activity, quality of life, functional capacity measured with standardised tools and biological therapy has not been reported.
Treatment of uveitis in PsA patients initially relies on topical corticosteroids, and more rarely by systemic route, or periocular injections.18 However, in case of recurrences or persistent inflammation, different conventional and/or biological immunosuppressive drugs have been implemented.18 The most widely used biological disease-modifying antirheumatic drugs (bDMARDs) are TNFα inhibitors (TNFi)19 such as etanercept (ETN), infliximab (IFX), adalimumab (ADA), golimumab (GLM) and certolizumab pegol (CZP).20 In addition, most biological therapies used in PsA including TNFi, ustekinumab, secukinumab (SECU) and ixekizumab have also been associated with paradoxical uveitis.21
Taking all these considerations into account, we aimed to evaluate, in a large unselected series of patients with PsA (A) the epidemiology and clinical features of PsA-related uveitis; (B) the association of uveitis with PsA activity, quality of life and functional disability and (B) the relationship of uveitis with the bDMARDs used. In addition, a literature review was also performed.
Patients and methods
Patients, enrolment criteria and study design
A retrospective longitudinal study of patients diagnosed with PsA in the last 30 years who attended a single referral University Hospital from January to December 2020 was conducted. Ocular involvement was assessed in a multidisciplinary ocular inflammatory disease unit by expert rheumatologists and ophthalmologists in patients with ocular symptoms.
The diagnosis of PsA was performed by a rheumatologist, based on the recognition of the musculoskeletal inflammatory disease in the context of psoriasis. These patients were classified according to the CASPAR criteria.22 The different domains of musculoskeletal involvement such as peripheral arthritis, dactylitis, enthesitis and axial spondylitis were identified.23
The diagnosis of uveitis was made by an expert ophthalmologist based on clinical and ophthalmological examinations. Evaluation for intraocular inflammation included assessment by slit-lamp biomicroscopy and funduscopic examination. In addition, fluorescein angiography was performed to assess the presence of vasculitis, and high-definition optical coherence tomography to measure the macular thickness. Visual acuity and intraocular pressure were also determined. The Standardisation of Uveitis Nomenclature working criteria were used to assess anterior chamber inflammation (0–4+).24
Informed consent was given for all patients included in the study. Patient data are sufficiently anonymised so that they are not individually identifiable.
Data collection and clinical assessment
Clinical data and laboratory parameters were retrieved from the patients' medical records. Demographic data, cardiovascular (CV) risk factors, PsA manifestations, HLA-B27 status, uveitis features (pattern, laterality, onset and recurrence) and the presence of other extra-articular manifestations were gathered. The presence of sacroiliitis on MRI was evaluated in patients with low back inflammatory pain. Information on treatment with non-steroidal anti-inflammatory drugs (NSAIDs), glucocorticoids and DMARDs was also collected. All data were stored in a computerised database, and all data were double-checked to minimise input errors.
Uveitis was classified according to the International Uveitis Study Group into anterior if it affected the iris or ciliary body; intermediate, if the vitreous chamber was involved; posterior, if it affected the choroid or the adjacent retina and panuveitis, when the anterior ocular chamber, the vitreous cavity and the retina and/or the choroid and/or the retinal vessels were compromised.25 Laterality, onset and recurrence were also analysed. Recurrence was defined as the presence of repeated episodes separated by periods of inactivity without treatment for at least 3 months.24
PsA activity was evaluated using two clinical scores, Bath Ankylosing Disease Activity Index (BASDAI) and Disease Activity Index for Psoriatic Arthritis (DAPSA) Score.26 27 BASDAI ranges from 0 (no activity) to 10 (maximum activity).26 27 DAPSA classified activity as remission (DAPSA ≤4), low (DAPSA in 5–14), moderate (DAPSA ≥15 to 28) or high (DAPSA >28) disease activity.27 Quality of life was evaluated using the PsA impact of Disease Score (PsAID)28 and the functional capacity according to the Bath Ankylosing Spondylitis Functional Index (BASFI).26 Skin involvement was measured using the Psoriasis Area and Severity Index score (PASI).29
CV risk factors were also evaluated. Dyslipidaemia was defined if one of the following data was present: triglycerides >150 mg/dL, cholesterol >200 mg/dL, LDL-cholesterol >130 mg/dL or HDL-cholesterol <40 mg/dL in men or <50 mg/dL in women. Serum lipid measurement was performed with standard techniques. Arterial hypertension was defined as systolic blood pressure higher than 140 mm Hg and/or diastolic blood pressure higher than 90 mm Hg. Diabetes was defined as a measured HbA1c level of at least 6.5% and the use of antidiabetic agents.
The relationship between bDMARDs and the incidence of uveitis was assessed by comparing the incidence before and during the biological treatment. Incidence of uveitis was reported as exposure adjusted incidence rate (EAIR) per 100 patient-years of biological drug exposure.
Statistical analysis
The incidence of uveitis per 100 patients-year and the proportion of patients who presented with uveitis over the follow-up period (from the time of diagnosis of PsA to the last visit) was calculated.
Categorical variables were expressed as frequencies and percentages. Continuous variables were expressed as mean±SD or median (25–75th IQR) as appropriate, and compared with the two-tailed Student’s t-test or the Mann Whitney U test. For dichotomous variables, the χ2 test or the Fisher’s exact test was used.
Data were analysed using SPSS V.20.0 for Windows (SPSS). Statistical significance was considered at p<0.05 in all the calculations.
Results
General features of the whole PsA sample
A total of 406 PsA patients (202 women/204 men) with a mean age of 46.3±12.3 years were included. The mean PsA duration was 9.9±8.2 years. The median delay from the onset of musculoskeletal symptoms to diagnosis of PsA was 1 (0–3) years. The main demographic data and disease-related features are summarised in table 1.
General features of 406 patients with psoriatic arthritis
The predominant pattern of PsA was peripheral and it was present in 236 (58.1%) patients. Mixed involvement was observed in 122 (30.1%) patients. The mean BASDAI score was 2.7±2.6, the median BASFI score was 1.2 (0–4) and 65 (16%) patients showed active disease (DAPSA>4). HLA-B27 was positive in 38 (9.4%) cases. Regarding CV risk factors dyslipidaemia was present in 201 (49.5%) cases, hypertension in 149 (36.7%) and diabetes in 47 (11.6%). Some 179 (44.1%) patients received glucocorticoids and 348 (85.7%) NSAIDs. Most of the patients were on bDMARDs, especially TNFi monoclonal antibodies (table 1).
Frequency and clinical features of uveitis
Uveitis (≥1 episode) was observed in 20 (4.9%) patients (12 women/8 men; mean age, 43.1±14.5 years) (table 1). The incidence rate of uveitis was 0.5/100 patients-year. The mean duration of PsA disease in patients with uveitis was 12.7±9.2 years.
The most common pattern of uveitis was anterior and unilateral (n=16, 80%) (table 2). Bilateral pattern was present in 4 (20%) patients. Posterior uveitis was only observed in four patients while none of them developed panuveitis. The onset was acute in all cases, and 10 (50%) patients suffered a recurrence. At the time of the study, there were no patients with uveitis who had presented with permanent vision problems.
Case series of PsA-related uveitis
Comparative study of PsA with and without uveitis: relationship of uveitis with PsA activity
The differences between the patients who developed uveitis and those who did not are shown in table 1. Regarding PsA features, patients with uveitis had a longer, although non-significant, disease duration(12.7±9.2 vs 9.8±8.2 years, p=0.129) and a higher prevalence of axial pattern (20% vs 11.4%, p=0.277). The peripheral joint pattern was predominant in both groups. There were no differences in the frequency of enthesitis and dactylitis.
On the other hand, patients who developed uveitis had a greater frequency of positive HLA-B27 (45% vs 7.5%, p<0.0001), sacroiliitis in MRI (25% vs 8.3%, p=0.027), ocular surface pathology (10% vs 0.8%, p=0.021), and higher PsAID score and BASFI index than those without uveitis (table 1).
Patients with uveitis also had a higher but not statistically significant disease activity (DAPSA>4, 30% vs 15.3%, p=0.11), skin involvement (PASI, 3.9±3.4 vs 1.9±0.4, p=0.245) and inflammatory bowel disease (10% vs 4.9%, p=0.277).
Relationship between uveitis and the biological treatment
All patients with uveitis received topical ophthalmic treatment. Treatment with oral NSAIDs, systemic glucocorticosteroids and cDMARDs was similar in patients with and without uveitis (table 1).
Flow-chart of biological agents in patients with PsA-related uveitis is shown in figure 1. bDMARDs were used in 8 (40%) patients with uveitis; 6 (30%) of them received TNFi monoclonal antibodies, 1 (5%) ETN and 1 (5%) SECU. Switching was required in 3 (15%) patients.
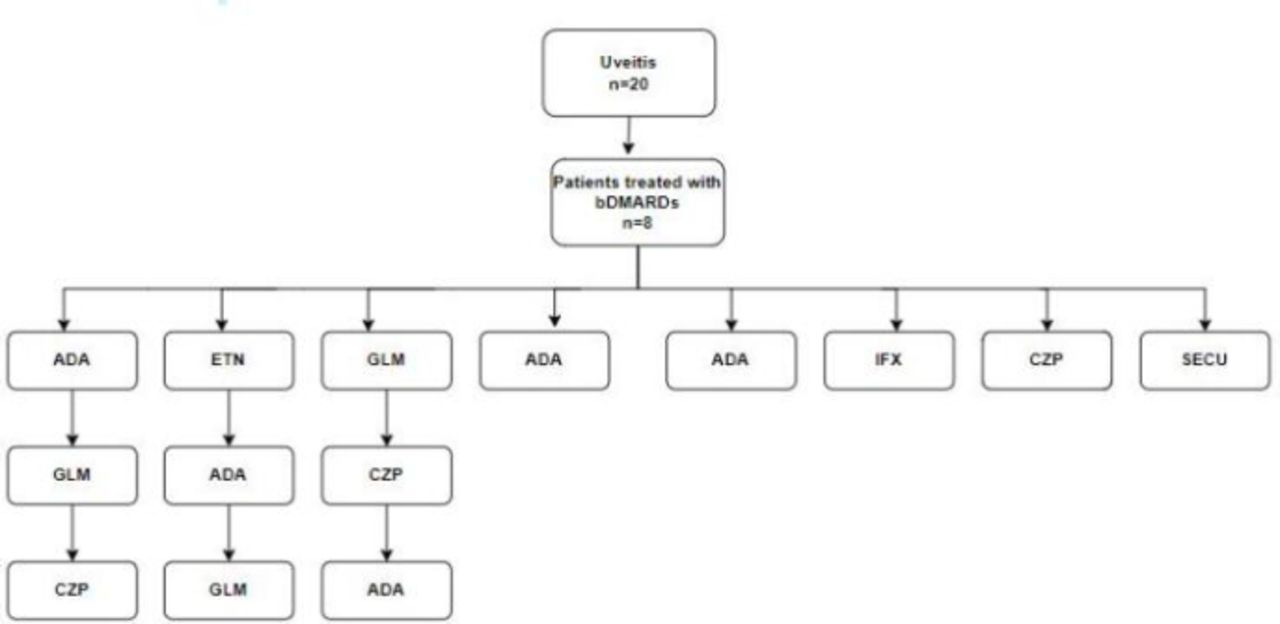
Biological and target immunosuppressive drugs in patients with PsA-related uveitis. ADA, adalimumab; bDMARDs, biological disease-modifying antirheumatic drugs; CZP, certolizumab pegol; ETN, etanercept; GLM, golimumab; IFX, infliximab; PsA, psoriatic arthritis; SECU, secukinumab.
The difference between patients with and without uveitis who received bDMARDs was not statistically significant (8 (40%) vs 129 (33.4%) (table 1). TNFi monoclonal antibodies were the most used bDMARDs in both groups.
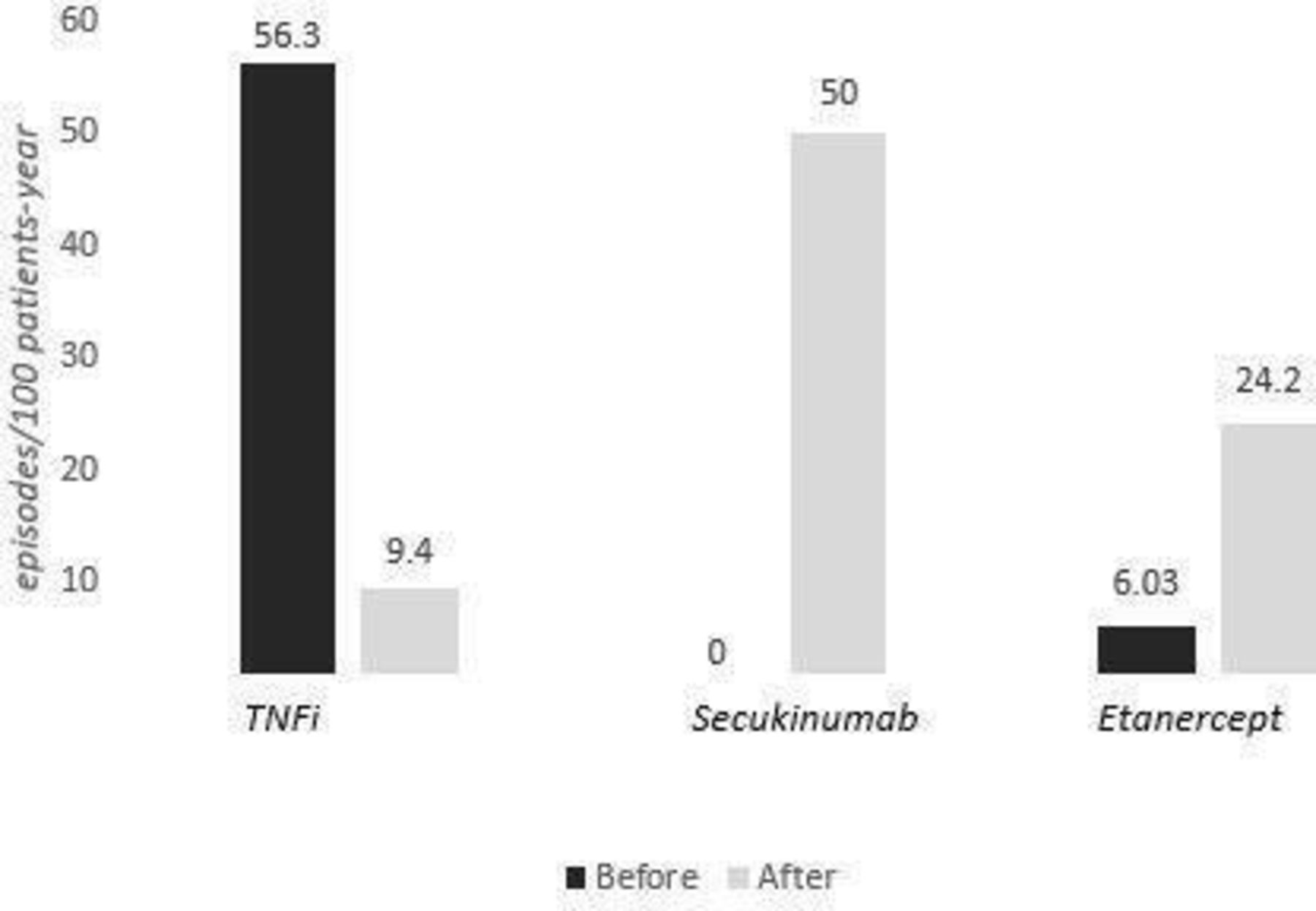
Figure 2 shows EAIR of uveitis before and after biological therapy. The EAIR of uveitis before treatment with TNFi monoclonal antibodies and ETN was 56.3 and 6.03 episodes/100 patients-year, respectively. Patients who were treated with SECU had no previous episodes of uveitis (figure 2). Once the treatment was established, the EAIR of uveitis in patients on TNFi monoclonal antibodies was 9.4 episodes/100 patients-year while in those treated with ETN and SECU was 24.2 and 50 episodes/100 patients-year, respectively.

{kind=link}
{kind=link}
Uveitis exposure adjusted incidence rate before and after biological therapy.
Discussion
Uveitis is the most common extra-articular manifestation of SpA and presents different patterns depending on the subtype of the disease.2 3 30 31 Acute anterior uveitis has also been reported to be closely related to SpA, especially AS.3 4 9 31–34 However, the ratio and characteristics of PsA-related uveitis are poorly understood with scarce studies based on small series of patients,5–9 summarised in table 2.
In this study, we present a large series of unselected patients with PsA. Uveitis was observed in 4.9% of cases, a figure lower than that reported in the literature.5–9 The lower proportion of uveitis in our study probably relies on a large number of patients, an unselected population and the use of the CASPAR classification criteria. In addition, the mean duration of PsA disease was almost 10 years in our series, whereas these data have not been specified in the most previous studies. A systematic review of the literature by Zeboulon et al35 reports that the prevalence of uveitis in PsA was 25.1%, a higher number than that reported in this study. These differences are probably because this is a study with limitations, such as the possible selection bias noted by the authors given the nature of the study, in that some patients may have been included in several studies resulting in overlap in the reported data. Although, the interpretation of the prevalence has to take into account that the mean duration of the disease was longer than in our study.
Regarding the clinical pattern, PsA-related uveitis should present insidiously, have a chronic course and should be bilateral, usually with anterior involvement, especially in patients with axial involvement.1 3 9 10 Our study revealed that the pattern of uveitis in PsA patients is similar to that observed in SpA, usually with an acute onset and an anterior and unilateral involvement. Although the predominance, in this case, has been unilateral, the presence of a bilateral pattern remains important, contrary to what has been classically reported in AS. Noteworthy, recurrence was described in half of our patients, while no data on relapses had been previously reported across series, although Durrani and Foster, in a case–control study of 36 patients with uveitis and psoriasis without joint involvement, suggested that psoriatic uveitis is usually recurrent.13
On the other hand, we found PsA-related uveitis to be associated with positive HLA-B27, sacroiliitis in MRI, ocular surface pathology, and worse PsAID and BASFI scores. The relationship between SpA and HLA-B27 is well described. Its prevalence ranged from 74 to 89% in patients with AS and non-radiographic axial SpA,36 37 while in the PsA subgroup it is described in up to 40%–50% of cases.38 In our series, the prevalence of HLA-B27 in PsA patients was 9.4%, lower than previously reported, probably because most of the reviewed studies related to PsA and uveitis did not analyse the variable HLA-B27 in all patients who developed uveitis. The most common ocular manifestation associated with HLA-B27 has been unilateral acute anterior uveitis.39 40
In our series, 60% of patients with uveitis presented peripheral joint involvement while the percentage of mixed and axial patterns were similar (20%). By contrast, Queiro et al6, found that the predominant joint pattern in PsA-related uveitis was axial or mixed (77%), while Paiva et al9 reported a similar peripheral/axial involvement in their series.
We have also found a significantly higher frequency of sacroiliitis in MRI in PsA patients with uveitis, as well a worse quality of life measured by PsAID, and greater functional disability assessed by the BASFI score.
It is known that factors such as male sex, HLA-B27 positivity, late-onset psoriasis, pustular form and the presence of dactylitis are related to the development and severity of uveitis in patients with psoriasis.10 Niccoli et al, in 242 patients with early PsA, observed 22 (9%) cases of iridocyclitis and 11 (50%) with dactylitis.41 However, in our series, we did not find differences in the frequency of dactylitis between patients who developed uveitis and those who did not.
The potential association with ocular surface complications and uveitis has been a matter of debate. Thus, Lambert et al described the ocular surface manifestations in PsA patients, but they did not relate it to the presence of uveitis.5 However, Abbouda et al found that dry eye was the main complication of the anterior chamber involvement, especially in patients with psoriasis due to dysfunction or obstruction of the meibonium glands or the lacrimal duct secondary to increased cell turnover.8 Our patients with PsA-related uveitis had a greater prevalence of ocular surface manifestations (10% vs 0.8%, p 0.021). By contrast, we did not find an association between uveitis and other extra-articular manifestations such as inflammatory bowel disease.
Furthermore, there is evidence that patients with PsA have an increased CV risk compared with the general population.42 Ferraz-Amaro et al have found a relationship between the presence of CV risk factors and increased inflammatory activity in a cross-sectional study of patients with PsA.43 Although our results have suggested that uveitis is associated with higher inflammatory burden (reflected by a higher prevalence of sacroiliitis) we have not found a significant association between CV risk factors and uveitis.
Regarding treatment, ADA was the most widely used TNFi monoclonal antibody. In our series, two patients were treated with CZP and another two with GLM. There is evidence that both CZP and GLM represent a useful therapeutic option in SpA-related uveitis, even in patients refractory to other anti-TNFα agents.44 45 Therefore, according to the 2019 EULAR update recommendations for the management of PsA, the biological drug of choice in patients with uveitis should be a TNFi monoclonal antibody.46 Similarly, the updated recommendations of the Psoriasis and Psoriatic Arthritis Research and Evaluation Group47 on the treatment of PsA and its comorbidities also recommend anti-TNFα agents (except ETN due to its lower efficacy compared with the other agents and the risk of paradoxical uveitis) as the biological treatment of choice in patients with PsA and uveitis.
A decrease in the EAIR of uveitis was observed with anti-TNFα monoclonal antibodies, while a higher EAIR was observed with other biological therapies such as ETN and SECU (figure 2). The EAIR of uveitis before treatment with TNFi monoclonal antibodies and ETN was 56.3 and 6.03 episodes/100 patients-year, respectively. Patients treated with SECU had no previous episodes of uveitis. Once the treatment was established, the EAIR of uveitis in patients on anti-TNFα monoclonal antibodies was 9.4 episodes/100 patients-year compared with 24.2 and 50 episodes/100 patients-year in those treated with ETN and SECU respectively. It should be noted that only one case treated with ETN and another with SECU is presented, which is an important limitation in this statement.
This finding is consistent with other series published in the literature. Thus, in the Swedish National Patient Registry, which included 1365 patients with AS treated with TNFi, a decrease in the incidence of uveitis was observed in those on TNFi monoclonal antibodies (ADA and IFX) while an increase was noted in those treated with ETN.48 In this sense, Wendling and Prati observed cases of paradoxical uveitis in patients with inflammatory rheumatic diseases, including SpA, rheumatoid arthritis and juvenile idiopathic arthritis, treated with ETN.21 49 Likewise, Lim et al50 concluded in a study of patients with AS and uveitis who were treated with iTNF that ETN is associated with a higher number of cases of uveitis than IFX or ADA. Regarding SECU, there are discordant data. Deodhar et al assessed the incidence of uveitis in patients with AS treated with SECU and found no increased risk, although the study was limited by the abscense of a control group.51 Nevertheless, Roche et al found a higher incidence of anterior uveitis in axial SpA patients treated with SECU compared with those on TNFi or placebo.52 Finally, a clinical practice study observed that SECU and ETN were associated with a higher incidence of anterior uveitis than ADA and IFX.53
In conclusion, in our study, uveitis related to PsA occurs less frequently than in SpA, but with a similar pattern of anterior and unilateral involvement, as well as an acute and often recurrent course of the disease. The presence of uveitis is associated with axial activity, impaired quality of life and increased functional disability. Therefore, uveitis may be a poor prognostic marker in PsA patients and could influence the choice of the therapeutic scheme. In this regard, we found a decrease in EAIR with TNFi monoclonal antibodies but, although the number of cases of uveitis was small, it seems not to occur with ETN or SECU.
Data availability statement
No data are available.
Ethics statements
Patient consent for publication
References
Footnotes
Contributors We submit for editorial process for publication this article 'Uveitis in psoriatic arthritis: study of 406 patients in a single university centre and literature review' and declare:*The article is unpublished.*Each one of the people who appear in it as author or author has directly contributed to the intellectual content of the work, approves the contents of the manuscript that is submitted to the editorial process and gives their consent for their name to appear in the authorship of the same.*That this article has not been previously published, is not in the review process in another journal, nor does it appear in another paper accepted for publication by another publisher.
Guarantor: Ricardo Blanco
*Ana de Vicente-Delmás, Lara Sánchez-Bilbao, and Vanesa Calvo-Río shared first authorship.†Dr R Blanco and Prof. José Luis Hernández shared senior authorship.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests Dr. MA González-Gay received grants/research support from Abbvie, MSD, and Roche, and had consultation fees/participation in company-sponsored speaker's bureau from Pfizer, Celgene, Novartis, Roche, Sanofi, and Lilly. Dr. R Blanco received grants/research support from Abbvie, MSD, and Roche, and had consultation fees/participation in company-sponsored speaker's bureau from Abbvie, Pfizer, Roche, BMS, Janssen, Lilly, and MSD. Dr. JL Hernández received grants/research support from Amgen and had participation in company-sponsored speaker's bureau from Amgen, and MSD. Vanesa Calvo-Río received grants/research supports from AbbVie, Lilly, MSD and UCB Pharma. Natalia Palmou-Fontana received grants/research supports from Novartis, GSK, Amgen and Sanofi. No financial disclosures declared: Ana de Vicente-Delmás, Lara Sánchez-Bilbao, David Martínez-López, Alba Herrero- Morant, Iñigo González-Mazón, Nuria Barroso-García and Eva Galíndez-Agirregoikoa.
Provenance and peer review Not commissioned; externally peer reviewed.