Article Text

Abstract
Introduction Early diagnosis of systemic sclerosis (SSc) is important to start therapeutic interventions timely. Important risk factors for progression to SSc are the SSc-specific autoantibodies, of whom anti-centromere antibodies (ACA) and anti-topoisomerase I antibodies (ATA) are the most frequent. ATA is associated with a severe disease course. A more detailed characterisation of the ATA-response in SSc might increase insights in preclinical disease stages and improve prognostication. To address this we identified all patients with suspected very early ATA-positive SSc, defined as all patients who are ATA-positive not fulfilling American College of Rheumatology (ACR)/European Alliance of Associations for Rheumatology (EULAR) 2013 criteria, in the Leiden Combined Care in Systemic Sclerosis (CCISS)-cohort and found very low numbers.
Methods This triggered us to search the literature on the ATA prevalence in patients with suspected very early SSc and contribution of the SSc-specific autoantibodies to progression from suspected very early to definite SSc. To increase insights on the ATA-response in suspected very early SSc, we then evaluated the association between the ATA-response and time between onset of Raynaud’s phenomenon (RP) and first non-RP symptom, as a proxy for progressing to definite SSc, in all patients with ATA-positive SSc from the Leiden CCISS-cohort.
Results In short, included studies show that prevalence of ATA is much lower in suspected very early SSc than in populations fulfilling ACR/EULAR 2013 criteria. After 1–15 years of follow-up, only 52% of the patients with suspected very early SSc progress to definite SSc. ATA-IgG levels tend to be higher in patients with ATA-positive SSc with more rapid disease progression.
Conclusion Although a role of ATA in disease progression is suggested, more studies on the ATA response in suspected very early SSc are warranted.
- Autoantibodies
- Scleroderma, Systemic
- Autoimmunity
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Systemic sclerosis (SSc) specific autoantibodies are important risk factors for progression from suspected very early SSc to definite SSc.
More insight into the characterisation and prevalence of the SSc-specific autoantibodies during the development of SSc is necessary to improve disease prognostication.
WHAT THIS STUDY ADDS
Prevalence of anti-topoisomerase I antibodies (ATA) is much lower in suspected very early SSc than in populations fulfilling American College of Rheumatology/European Alliance of Associations for Rheumatology28 2013 criteria.
ATA-IgG levels tend to be higher in patients with ATA-positive SSc with less time between onset of Raynaud’s phenomenon and first non-Raynaud’s phenomenon symptom, as proxy for disease progression.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Although a role of ATA in disease progression is suggested, more detailed studies on the characterisation of ATA and underlying B-cell responses in suspected very early SSc are needed.
The low ATA prevalence among patients with suspected very early SSc suggests swift disease progression in ATA-positive SSc and consequently a different approach to identify this subgroup before development of irreversible organ damage.
Introduction
Systemic sclerosis (SSc) is a rheumatic autoimmune disease with a pathogenesis involving a triad of autoimmunity, vasculopathy and fibrosis.1 Early diagnosis of SSc is crucial to start therapeutic interventions before development or progression of organ damage. In 2013, the American College of Rheumatology (ACR)/European Alliance of Associations for Rheumatology (EULAR) criteria for SSc were published showing an increased sensitivity to classify patents with SSc early in the disease course.2 In addition, criteria for suspected very early SSc were developed consisting of Raynaud’s phenomenon (RP), SSc-specific autoantibodies, puffy fingers and abnormal nailfold capillaroscopy.3 4 Patients classified as suspected very early SSc do not fulfil ACR/EULAR 2013 criteria for SSc. The progression from suspected very early SSc to ACR/EULAR 2013 criteria is usually defined by the development of a first non-RP symptom.
Anti-topoisomerase I antibodies (ATA) and anti-centromere antibodies (ACA) are the most prevalent SSc-specific antinuclear autoantibodies,5 and are used for disease and risk stratification.6 7 In patients with suspected very early SSc, presence of SSc-specific autoantibodies are important predictors for the development of definite SSc8 9. However, so far little is known on the contribution of the SSc-specific autoantibodies to the underlying processes involved in disease progression and whether this is different between ATA and ACA. Given the importance of the SSc-specific autoantibodies for progression to SSc, more detailed characterisation of the autoantibody responses in preclinical disease stages might increase insights in disease development and contribute to improved disease prognostication. In this paper we show the different steps and analyses we undertook to evaluate the ATA characteristics during progression from suspected to definite SSc.
The challenge in finding patients with suspected very early SSc with ATA
For ACA, we recently studied 138 patients with suspected very early SSc and 487 patients with definite SSc with ACA and showed that ACA-IgG and ACA-IgM levels were significantly higher in patients with definite SSc.10 In the patients with suspected very early SSc, progression to definite SSc was associated with higher ACA-IgG levels at baseline.10 We set out to identify whether this observation also holds for ATA-positivity, but could only identify 4 patients with suspected very early ATA positive SSc in the 1077 patients referred to the Leiden Combined Care in Systemic Sclerosis (CCISS) cohort. The most recent study of the very early diagnosis of SSc (VEDOSS) project, a European multicentre study in suspected very early SSc, evaluated progression to SSc in 553 patients with suspected very early SSc.9 Strikingly, although 32% of the patients with suspected very early SSc in this study were ACA-positive (=164), only 7% were ATA-positive (n=39). Intriguingly, the prevalence of ATA is much higher among patients with definite SSc: for example, 24% of the patients with SSc in the Leiden CCISS cohort is ATA-positive11 and 39% in the European Scleroderma Trials and Research (EUSTAR) cohort.12 These observations triggered us to perform a literature search to review the prevalence of ATA in patients with suspected very early SSc and on the contribution of the SSc-specific autoantibodies to progression from suspected very early to definite SSc.
Part 1: literature study
Methods
The research question for the scoping literature review was ‘What is the contribution of the SSc-specific autoantibodies and their underlying B cell response to the progression of suspected very early SSc to definite SSc?’. We searched PubMed with the following terms: ‘very early SSc’, ‘VEDOSS’, ‘suspected’, ‘isolated RP’, ‘progression’ and ‘SSc’. All identified articles were assessed for relevant content by the corresponding author. Initial rejection for further evaluation was based on the information in the abstract; next, secondary rejection was based on the content of the full article. All other studies were included if they were original research in English, included greater than five patients and reported on prevalence of SSc-specific autoantibodies in suspected very early SSc, clinical characteristics of suspected very early SSc and/or the progression of isolated RP/suspected very early SSc to definite SSc.
Results
We included the following studies: (1) six studies reporting on the prognostic value of SSc-specific autoantibodies for progression of RP or suspected very early SSc to definite SSc,8 9 13–17 (2) six studies describing clinical characteristics of patients with suspected very early SSc18–23 and (3) two studies investigating SSc-specific autoantibody responses in detail and their association with progression of RP or suspected very early SSc to definite SSc.10 24
The ATA prevalence reported in the studies on suspected very early SSc and VEDOSS ranges from 0.2% to 24% (tables 1 and 2). The lowest prevalence of ATA was reported in the studies that recruited patients based on RP. In studies also including patients with organ involvement, ATA prevalence was higher (tables 1 and 2). Progression from RP to definite SSc occurred in 0% to 21% of the patients, and progression from suspected very early SSc to definite SSc in 8% to 52% of the patients. Moinzadeh et al reported that patients with isolated RP with anti-RNA-polymerase III had 1.7 (SD: 6.4) years between RP and SSc onset, with ATA 3.6 (SD: 6.4) years and with ACA 10.8 (SD: 12.5) years.16 In the other studies, no specific progression rates for the different autoantibody subgroups were reported. All studies except for the study of Trapiella-Martínez et al found that the presence of SSc-specific autoantibodies increased the risk for progression from RP or suspected very early SSc to definite SSc.15 In the study of Trapiella-Martínez et al, patients who progressed from suspected very early SSc to definite SSc were ATA-positive more often than patients who did not progress (19% vs 8%).15 Intriguingly, some studies describing clinical characteristics of patients with suspected very early SSc showed substantial prevalence of possible organ involvement, such as oesophageal symptoms, digital ulcers, puffy fingers in their populations, by which they might have fulfilled ACR/EULAR 2013 SSc criteria (table 2).
Studies evaluating the association of the SSc-specific autoantibodies and the progression of RP/suspected very early SSc/VEDOSS to definite SSc
Prevalence of SSc-specific autoantibodies and clinical characteristics in patients with suspected very early SSc
In order to elucidate if the SSc-specific autoantibodies are more than active bystanders in the development of SSc, it is important to study their response more in depth. So far, we found two studies evaluating the association between levels of autoantibodies and progression to definite SSc. The first study by Lande et al evaluated anti-CXCL4 and found no differences in anti-CXCL4 levels between patients who progressed to definite SSc and patients who did not.24 The second study of our own research group (van Leeuwen et al10) evaluated ACA isotype levels. Of all patients with suspected very early SSc with follow-up (n=115), 39% progressed to definite SSc and the ACA-IgG levels at baseline were significantly associated with progression to definite SSc.10
Part 2: time between RP and first non-RP
The results of the literature review suggest that ATA positivity is associated with a more rapid progression of disease towards fulfilment of the ACR/EULAR 2013 SSc criteria, based on the strikingly low prevalence of ATA among suspected very early SSc.25 The mechanism behind this is unknown. To complement these observations, we aimed to investigate if the ATA response is associated with the (rate of) disease progression in suspected very early SSc. To tackle the problem of low numbers of patients with suspected very early SSc with ATA, we evaluated time between onset of RP and first non-RP symptom as a proxy for progressing to definite SSc, and investigated if this is associated with clinical and ATA response characteristics. We hypothesise that RP may be the first manifestation in suspected very early SSc. We assumed that a shorter time between RP and first non-RP symptoms reflects more rapid disease progression and thus (risk for) more severe disease. For this part, we took advantage of the prospective Leiden CCISS cohort.26
Methods
Patients
Patients with SSc, fulfilling the ACR/EULAR 2013 SSc criteria at cohort entry2 and positive for ATA-IgG, were included from the prospective CCISS cohort at Leiden University Medical Center until 1 January 2022.26 We used the following definitions for the included patients:
Definite SSc: fulfilling ACR/EULAR 2013 criteria.2 Early SSc refers to patients with definite SSc with a short disease duration (<2 years since first non-RP).
Suspected very early SSc: fulfilling VEDOSS criteria, but not the ACR/EULAR 2013 criteria.3 4 The VEDOSS criteria consist of RP, SSc-specific autoantibodies, puffy fingers and abnormal nailfold capillaroscopy.
All patients with SSc in the CCISS cohort undergo annual screening for organ involvement and gave informed consent.
Disease characteristics
At baseline visit, clinical data and blood samples were collected from all patients. A detailed explanation of the definitions for organ involvements are shown in the online supplemental file 1. Baseline was defined as the first visit in the CCISS cohort. Patients were categorised in three groups using the terciles of time between RP and first non-RP: (1) ≤3 months, (2) 4 to ≤24 months (3) ≥25 months.
Supplemental material
Anti-topoisomerase I assay and measurements
One hundred and one patients with ATA-positive SSc were randomly selected for ATA measurements. A detailed description of the ATA assay is described elsewhere.27
Statistical analysis
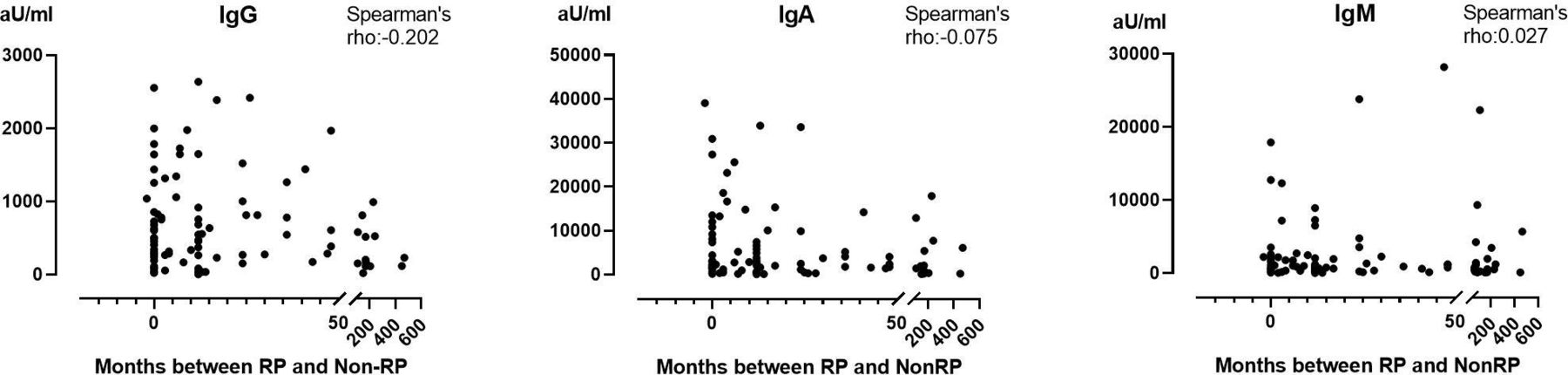
Disease characteristics at baseline were compared using independent t-tests, Kruskall-Wallis, Mann-Whitney U and χ2 tests between the three times between the patients with RP and first non-RP groups. Correlation between time between RP and first non-RP symptom and the ATA isotype levels was assessed using Spearman’s rank order correlation test. Based on figure 1, a cut-off of 1000 IE was taken and time between RP and first non-RP was compared between patients with high ATA-IgG levels (≥1000 AU/mL) and lower ATA-IgG levels (<1000 AU/mL) using Kruskal-Wallis tests. Analyses were conducted with SPSS V.25.0 (SPSS, Chicago, Illinois, USA). A p value of <0.05 was considered statistically significant.

Anti-topoisomerase I antibody (ATA) IgG, IgA and IgM levels in 101 patients with ATA-IgG+SSc at baseline. Spearman’s correlation for IgG: −0.202 (p=0.041); for IgA, −0.075 (not significant) and IgM, 0.027 (not significant). RP, Raynaud’s phenomenon; SSc, systemic sclerosis.
Results
Clinical characteristics
In total, 169 patients were ATA-IgG-positive. Of the 708 patients with definite SSc fulfilling ACR/EULAR 2013 SSc criteria, 163 (23%) were ATA-positive. Of the 115 suspected very early patients, 4 (3%) were ATA-positive. Given the low number of ATA-positive suspected very early SSc, we focused on the 163 patients with SSc for evaluation of clinical characteristics and antibody response. However, in 2/163 patients with ATA-positive SSc, dates of RP or first non-RP symptom was unknown and these patients were therefore excluded. For this part, we thus included 161 patients with ATA-positive SSc. Of these included patients, 55 (34%) had a time between RP and the first non-RP symptom of ≤3 months, 54 (34%) between 4 and ≤24 months and 52 (32%) between ≥25 months.
At baseline visit, patients with ≤3 months between RP and first non-RP were men more often compared with patients with 4 to ≤24 months and ≥25 months (47% vs 26% vs 31%, respectively, p=0.035), had a higher skin score (9 (5; 17) vs 5 (2; 14) vs 4 (2; 7), respectively, p=0.002) and had diffuse cutaneous SSc more often (53% vs 52% vs 23%, respectively, p=0.004; (table 3)).
Baseline characteristics of patients with included anti-topoisomerase I antibodies positive SSc categorised in groups based on time between RP and non-RP
The prevalence of interstitial lung disease (ILD) on high-resolution CT (HRCT) at baseline visit was similar between all groups (64% vs 63% vs 64%, p=0.690), whereas the proportion of patients with ILD on HRCT and an abnormal pulmonary function test was higher in the group of ≤3 months and 4 to ≤24 months compared with ≥25 months (31% vs 28% vs 15%, respectively, p=0.158; Table 3).
Skin tightening was the first non-RP symptom most frequently reported, namely in 78 (48%) patients with ATA-positive SSc, followed by sclerodactyly/puffy fingers in 28 (17%). In the patients with ≤3 months between RP and first-non RP, sclerodactyly/puffy fingers was more frequently reported (12 (28%)) compared with patients with 4 to ≤24 months (5 (9%)) and ≥25 months (9 (20%); Table 3).
ATA-IgG, ATA-IgM and ATA-IgA levels
Serum samples obtained at baseline (inclusion in the cohort) were analysed in 101/161 patients with ATA-positive SSc. Presence of ATA-IgA and ATA-IgM was similar between the three groups (table 4). A clear decrease in ATA-IgG levels was seen between the groups categorised on time between RP and first non-RP symptoms (p=0.361; figure 2/table 4). ATA-IgG levels correlated weakly with the time between RP and first non-RP (Spearman’s rho: −0.202, p=0.041; Figure 1), but ATA-IgM and ATA-IgA levels did not. In patients with ATA-IgG levels ≥1000 AU/mL median time to develop a first non-RP symptom was 7 months (range 0–24) as compared with 12 months in patients with ATA-IgG levels <1000 AU/mL (range: 1–65; p=0.089).
ATA characteristics of patients with included ATA-positive SSc categorised in groups based on time between RP and non-RP

{kind=link}
{kind=link}
Baseline anti-topoisomerase I antibody (ATA) IgG, IgA and IgM levels in 101 patients with ATA-IgG+SSc, categorised in groups based on time between RP and first non-RP symptom. Patients are categorised in three groups based on the terciles of the time between RP and first non-RP symptom: (1) ≤3 months (n=55), (2) 4 to ≤24 months (n=54) and (3) ≥25 months (n=52). The ATA-IgG, ATA-IgA and ATA-IgM levels were not statistically significant difference between the groups. RP, Raynaud’s phenomenon; SSc, systemic sclerosis.
Discussion
Our literature search shows that the progression rate of suspected very early SSc to definite SSc varies between 8% and 52%. Among patients with suspected very early SSc the lowest prevalence of ATA is observed in patients recruited based on RP and highest in patients with suspected very early SSc with organ involvement. In addition, in patients with definite SSc from the Leiden CCISS cohort, ATA-IgG levels were higher in patients with shorter duration between first RP and first non-RP symptom. We observed that patients with ATA-IgG-positive SSc with a shorter time between RP and non-RP had severe skin involvement more often, but other disease complications were comparable between groups.
Suspected very early SSc: characteristics, role of SSc-specific autoantibodies and terminology
The relevance of SSc-specific autoantibodies, including ATA, as predictors for development of SSc has been confirmed by multiple studies.8 9 The ACR/EULAR SSc criteria in 2013 have led to the identification of more patients with ATA-positive SSc with a less severe disease course,28 which is an important step towards early recognition of the disease. Like in the VEDOSS study,9 also in the Leiden CCISS cohort the prevalence of ATA among patients with the very early SSc was lower than expected based on the distribution in definite SSc. From the literature review it becomes apparent that the prevalence of ATA in patients with suspected very early SSc ranges from 0.2% to 24%, which is a rather wide range. As the majority of studies have been performed in Europe, it is not likely that ethnicity plays a role. Also, the percentage of men in the studies was generally the same and ranged from 8% to 11%. Therefore, we think that the definitions of suspected very early SSc used in the included studies explain the observed difference, because the percentage of ATA positivity is lowest in studies that only include RP and highest in studies that also include patients with organ involvement. Indeed this might again underline that in ATA-positive disease, progression to full blown disease is swift, decreasing the chance of an ATA-positive patient to be captured in the RP only phase.
The terminology of the classification of the different stages in SSc is complex and might interfere with uniform patient stratification. First, patients with all signs or symptoms of the VEDOSS criteria already fulfil the 2013 ACR/EULAR SSc classification criteria. This can be confusing and blur clinical association studies to improve phenotyping in SSc. Second, the current terminology VEDOSS (very early diagnosis of SSc) could be questioned as well. As shown in table 1, of all patients fulfilling these criteria up to 50% will eventually progress to a diagnosis. Therefore, ‘clinical suspicion’ is perhaps more appropriate to classify these patients.
To proceed in this field we propose to perhaps take advantage of the development in other autoimmune diseases like rheumatoid arthritis (RA). In RA, the concept of clinically suspect arthralgia has been developed to facilitate clinical studies in preclinical stages.29 In contrast to RA, where this is mainly based on clinical features, in patients with RP, presence of autoantibodies and abnormal nailfold capillaries, next to puffy fingers, are main risk factors.9 19 This indicates that additional investigations are needed to identify patients at risk. To increase insights in the development of SSc, it is thus necessary to identify patients in preclinical stages, that is, persons who do not have a diagnosis yet. As the presence of autoantibodies is a profound risk factor, we propose to make this distinction based on the presence of RP and anti-nuclear antibody (ANA) positivity/SSc-specific autoantibody.
Time between RP and non-RP
To deal with the low number of patients with suspected very early ATA-positive SSc, we took time between RP and first non-RP symptom as a proxy for progression to SSc. Of course, these are not one-to-one applicable but could provide a direction. We observed an association with time between RP and first non-RP symptom and higher ATA-IgG, but not for ATA-IgM or ATA-IgA. This is in line with research in ACA-positive SSc, which shows that progression from suspected very early ACA-positive SSc to definite SSc was associated with higher ACA-IgG levels at baseline.10 While we confirmed the previous observed association between ATA-IgG level and lung progression,15 we did not see an association between ATA-IgM and time between first RP and first non-RP.27 The reason for a lack of association between ATA-IgM and time between RP and non-RP in our cohort might be the fact that we studied patients who already progressed to definite SSc. While the previous study evaluated disease progression yes/no 1 year after sample collection,27 the current study evaluated association between presence of ATA-IgM and the time between RP and first non-RP, which was preceding sample collection.
Currently, testing for the different isotypes of ATA in serum is not part of the routine clinical diagnostic workup and also not commonly available as standardised test in diagnostic laboratories. Recent research shows that the presence of autoreactive IgM is associated with disease progression in both ACA and ATA-positive SSc.10 27 IgM has the shortest serum half-life (7 days) compared with IgG and IgA and can therefore be considered a proxy for the recent and/or continuous stimulation of the adaptive immune response. The observed association between the presence of ATA-IgM with SSc disease progression in the near future27 points to a close association between (activation of) the ATA B-cell response and disease progression and suggests that ATA-expressing B cells may contribute to disease progression. Antibodies of the IgA isotype are generally associated with immune responses at mucosal surfaces. It is intriguing to speculate how these might associate with antigen expression in the pulmonary and/or gastrointestinal environment. We hypothesise that more insight into the evolution of the different ATA isotypes will increase insights in how autoreactive B cells contribute to disease progression in SSc. As the observations described are still experimental in nature, however, testing different ATA isotypes in serum cannot yet be advocated for routine clinical care. Nonetheless, we consider that testing for the presence of ATA-IgM might be of additive value to guide treatment decisions in SSc in the future.
Identifying patients with suspected very early SSc with ATA remains challenging, and we were thus not able to prospectively evaluate the association between ATA levels and progression from very early SSc to definite SSc. The observation that higher ATA-IgG is associated with shorter time between first RP and first non-RP might indicate a pathogenic role of the ATA B-cell response in the pathophysiology of SSc, a research topic which has intrigued researchers for many years. Recently, Senécal et al30 updated criteria, originally proposed by Naparstek and Plotz,31 for the definition of pathogenic autoantibodies in SSc. They concluded that ATA has the most evidence in favour of a possible pathogenic role compared with the other SSc-specific autoantibodies as ATA had evidence for all criteria except for the seventh criterion.30 The seventh criterion states that the autoantibody should be found along with a plausible target antigen at the site of the tissue damage. This is difficult to demonstrate in a chronic disease, and underlines the importance to identify ATA-positive individuals before progression to definite SSc to enable evaluation in early stages without chronic organ damage.
Regarding the second aim of this paper, we found that patients with a shorter disease duration were men and had skin involvement more often, which is in line with previous research16 32 and clinical experience. Interestingly, the prevalence of ILD on HRCT in the three patient groups based on time between RP and non-RP in this study was similar, but a trend towards a lower prevalence of clinically meaningful ILD in the group with the longest time between RP and non-RP was observed. This is an intriguing observation which we do not yet fully comprehend. As ILD is currently the most prominent cause of death in patients with SSc,33 this warrants further research.
Limitations of this study include the small number of patients and the possible recall bias of the onset of RP and non-RP by patients. Duration since first Raynaud is evaluated at baseline in all patients following a standardised intake questionnaire. The same method is applied to all patients and therefore it is unlikely that recall bias is different between the three groups. For this reason, we conclude that the observed association between ATA-IgG and more rapid progression is likely valid. Another limitation is that we do not know whether ATA have been present before onset of RP; as a consequence the interval between expression of ATA and development of first SSc-related symptom is not known. On the other hand, the fact that the proportion of clinically meaningful ILD is comparable between the three groups indicates that—if existing—the incident ATA-positive cases are equally distributed among the groups. However, our results do indicate a possible pathogenic role of ATA and warrant further multicentre research on the progression of patients with very early ATA to definite SSc.
To conclude, prevalence of ATA is much lower in suspected very early SSc than in populations fulfilling ACR/EULAR 2013 criteria. ATA-IgG levels tend to be higher in patients with ATA-positive SSc with more rapid disease progression. Although a role of ATA in disease progression is hereby suggested more detailed studies in preclinical SSc are warranted. To achieve sufficient power joint effort between expert clinics to identify persons with RP and ATA is necessary.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by METC-LDD (REU 043/SH/sh and CME no. B16.037). Participants gave informed consent to participate in the study before taking part.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors Concept and design: SIEL and JDV-B. Acquisition of data: SIEL and BAW. Analysis and interpretation: SIEL, SN, CMF, REMT, CFA, TWJH, HUS and JDV-B. Drafting the manuscript: SIEL and JDV-B. Revising the manuscript critically: All authors. All authors read and approved the final manuscript. SIEL and JDV-B accept full responsibility for the work and/or the conduct of the study, had access to the data, and controlled the decision to publish.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.