Article Text

Abstract
Objectives To describe power Doppler (PD) ultrasound findings in joint regions with B-mode (BM) synovitis using a standardised scanning protocol and scoring system in patients with juvenile idiopathic arthritis (JIA). Further, to examine associations between PD findings and BM synovitis, clinical arthritis, patient characteristics and disease activity.
Methods In this cross-sectional study, one experienced ultrasonographer, blinded to clinical findings, performed ultrasound examinations in 27 JIA patients with suspected clinical arthritis. The elbow, wrist, metacarpophalangeal 2–3, proximal interphalangeal 2–3, knee, ankle and metatarsophalangeal 2–3 joints were assessed bilaterally and scored semiquantitatively (grades 0–3) for BM and PD findings using a joint-specific scoring system with reference atlas. Multilevel mixed-effects ordered regression models were used to explore associations between PD findings and BM synovitis, clinical arthritis, age, sex, JIA subgroups, disease duration and 10-joint Juvenile Arthritis Disease Activity Score (JADAS10).
Results Twenty-one girls and six boys, median age (IQR) 8 years (6–12 years) were included. Overall, 971 joint regions were evaluated by ultrasound, 129 had BM synovitis and were assessed for PD. PD findings were detected in 45 joint regions (34.9%), most frequently in the parapatellar recess of the knee (24.4%). Increasing PD grades were associated with higher BM grades (OR=5.0,p<0.001) and with clinical arthritis (OR=7.4,p<0.001) but not with age, sex, JIA subgroups, disease duration or JADAS10.
Conclusion Increasing severity of PD findings were significantly associated with BM synovitis and with clinical arthritis. This suggests that PD signals detected using a standardised ultrasound examination and scoring system can reflect active disease in JIA patients.
- Arthritis, Juvenile
- Synovitis
- Ultrasonography
- Synovial fluid
- Inflammation
Data availability statement
Data are available on reasonable request. Quantified ultrasound data may be available on reasonable request, but patients’ data are not publicly available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Ultrasound is a valuable tool in the evaluation of synovitis in patients with juvenile idiopathic arthritis (JIA), but the interpretation of Doppler signals in children is challenging due to physiological vascularisation that can be misinterpreted as pathological findings.
WHAT THIS STUDY ADDS
Power Doppler (PD) findings in multiple joint regions with B-mode (BM) synovitis in patients with JIA were described using a standardised scanning approach and scoring system. Increasing PD grades were significantly associated with higher BM grades and with the presence of clinical arthritis.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Doppler signal assessment using a standardised ultrasound examination and a joint-specific scoring system can establish a feasible and more accurate interpretation of disease activity in patients with JIA.
Introduction
Ultrasound is a well-tolerated, non-invasive and easily accessible imaging technique that is well suited for use in children. However, the interpretation of ultrasonographic images in children can be challenging due to the unique features of the growing skeleton.1–3 The interpretation of Doppler signals in children is especially challenging because of physiological vascularisation during growth. Doppler signals in healthy children can be detected in fat pads, epiphysis, physis and in intracartilaginous regions of small bones.4–6 It is important that physiological vascularisation on ultrasound in children is not misinterpreted as pathological vascularisation and a sign of synovitis.
Few data exist on the evaluation of Doppler findings in patients with juvenile idiopathic arthritis (JIA). The studies conducted have used different scanning approaches, definitions for abnormal Doppler signals and scoring systems.7–11 In addition, previous studies have mostly used ultrasound definitions developed for adults with rheumatoid arthritis (RA), which may not be suitable for use in children.7–11
The Outcome Measures in Rheumatology (OMERACT) ultrasound group has made preliminary ultrasound definitions for synovitis in children, including B-mode (BM) and Doppler findings.12 Only Doppler signals detected within synovial hypertrophy are considered pathologic.12 The fact that Doppler signals need to be intrasynovial and not just intraarticular is an important differentiation from the definition in adults.13
A standardised ultrasound examination and scoring system for Doppler signals are needed to clarify the role of Doppler findings in monitoring disease activity and treatment effects in patients with JIA. A scanning protocol and an ultrasonographic joint-specific semiquantitative scoring system for BM synovitis and power Doppler (PD) activity with reference atlas for patients with JIA have recently been developed and have shown moderate to excellent reliability.14
As ultrasound is increasingly being used in the evaluation of synovitis in children and has become an important tool in the management of patients with JIA,15 16 it is essential to understand the significance of Doppler findings in these patients. A description of abnormal Doppler signals and an evaluation of whether these findings reflect active disease are needed.
The objectives of this study were, first, to describe PD ultrasound findings in joint regions with BM synovitis using a standardised scanning protocol and a joint-specific scoring system for synovitis with reference atlas for patients with JIA. Second, to explore whether PD grades were associated with BM grades and with the presence of clinical arthritis. Further, to examine associations between PD grades and age, sex, JIA subgroups, disease duration and measures of disease activity.
Methods
In this cross-sectional study, 27 patients with JIA, classified according to the International League of Associations for Rheumatology (ILAR),17 who had suspected clinical arthritis, that is, an assumed flare that required treatment adjustment, were consecutively recruited from the inpatient and outpatient clinic at the Department of Rheumatology at Oslo University Hospital, Norway between September 2020 and May 2022.
Clinical and laboratory assessment
The patient’s age, sex, JIA subgroup, disease duration and medications used were registered at the study visit. Clinical 71 joint evaluation18 was performed by experienced rheumatologists who were blinded to ultrasound findings. Clinical arthritis was defined as the presence of joint swelling, or of joint tenderness and limited range of motion.19 Disease activity was assessed using the 10-joint Juvenile Arthritis Disease Activity Score (JADAS10), (range 0–40) with the new cutoffs for disease activity states in JIA.18 20 The JADAS10 includes the following four measures; the number of joints with clinical arthritis (the count of joints with clinical arthritis up to a maximum of ten joints, any joint count higher than 10 gives 10 points in the score), physician global assessment (PhGA) of disease activity (0–10 cm Visual Analogue Scale (VAS) where 0=no activity and 10=maximum activity), parent/patient global assessment (PGA) of the patients well-being (0–10 cm VAS where 0=very well, 10=very poor) and the normalised erythrocyte sedimentation rate (0–10).18 20
Ultrasound examination
All patients underwent an ultrasound examination within 2 days after the clinical assessment. The ultrasound examinations were performed by the same rheumatologist (NKS) with extensive ultrasound experience. Inter-reader and intra-reader reliability evaluation have been reported in a previous study.14 The ultrasonographer was blinded to clinical findings, but the patient’s age was known. The same ultrasound machine, a GE Logiq S8 machine with linear probe (6–15 MHz) and hockey stick (8-18MHz), with standardised settings for BM and PD (pulse repetition frequency 0.6 kHz, frequency 7.7 MHz and low wall filter) was used in all examinations. PD was chosen instead of colour Doppler because the ultrasonographer had most experience with PD. The ultrasound examinations were done in 18 joint regions bilaterally according to an image acquisition protocol for patients with JIA including the anterior elbow, posterior elbow, radiocarpal, midcarpal, metacarpophalangeal (MCP)2 and MCP3 (dorsal), proximal interphalangeal (PIP)2 and PIP3 (dorsal and volar), knee (suprapatellar and lateral parapatellar recess), tibiotalar, talonavicular, anterior subtalar, posterior subtalar, metatarsophalangeal (MTP)2 and MTP3 (dorsal) joints.14 Synovitis detection on ultrasound was defined according to the preliminary ultrasound definitions for synovitis in children.12 The ultrasound findings were scored at the time of acquisition according to a joint-specific semiquantitative scoring system for BM synovitis and PD activity with reference atlas for patients with JIA ranging from grade 0 (normal) to grade 3 (severe) for each joint region.14 PD activity was scored accordingly: grade 0: no Doppler signal. Grade 1: 1–3 signals within the area of synovial hypertrophy only. Grade 2: >3 signals or confluent signals present in <50% of the area of synovial hypertrophy. Grade 3: confluent signals present in >50% of the area of synovial hypertrophy.21 The synovial abnormalities threshold for BM and PD findings was chosen to be grade ≥1. PD findings were only scored within synovial hypertrophy in joint regions with BM synovitis (grade≥1). The EULAR recommendations checklist for reporting of ultrasound studies in rheumatic and musculoskeletal diseases was used.22
Statistical analysis
Baseline patient characteristics were expressed as the number (%) or median (IQR). Further analyses were performed on a joint level. This included the 18 joint regions that were examined with ultrasound (anterior elbow, posterior elbow, radiocarpal, midcarpal, MCP2-3 (dorsal), PIP2-3 (dorsal and volar), knee (suprapatellar and lateral parapatellar recess), tibiotalar, talonavicular, anterior subtalar, posterior subtalar and MTP2-3 (dorsal)). Only joint regions with BM synovitis (grade≥1) were included in the analyses. The proportion of PD findings (grades 0–3) in joint regions with BM synovitis and in joint regions with clinical arthritis was described. Joint regions within the same clinically assessed joint (elbow anterior/posterior, knee suprapatellar/lateral parapatellar recess, subtalar anterior/posterior, PIP dorsal/volar) were attributed to the same clinical finding. To account for within-patient effect (random intercept), we used multilevel mixed-effects ordered logistic regression analyses. Cross-sectional associations between PD grades and BM grades and clinical arthritis were examined with adjustment for joint regions and side (left and right). We also performed analysis with further adjustment for age and sex to examine if the associations were altered. Associations between PD grades and age, sex, JIA subgroups, disease duration and measures of disease activity (JADAS10) were also explored. P values <0.05 were regarded as statistically significant. For missing PhGA, PGA and biochemical values, the JADAS10 was not estimated. One joint region (anterior elbow) was not assessed by ultrasound because of band-aid in the elbow, but for joint regions assessed by ultrasound there were no missing values for BM grades, PD grades or findings of clinical arthritis. Statistical analyses were performed using STATA V.17.
Patient and public involvement
Patients did not actively participate in the planning of this study. However, the participants and the Norwegian Rheumatism Association have communicated that this is of interest to the patient community, especially due to the difference in the use and interpretation of ultrasound in children. Study results will be disseminated to patients and the public through the patient organisation’s website and newsletter.
Results
Table 1 shows demographic and clinical characteristics of the 27 patients. A total of 971 joint regions were evaluated by ultrasound. Of these, 129 joint regions had BM synovitis and were included in further analyses (flowchart of joint region assessment in online supplemental figure 1).
Supplemental material
Demographic and clinical characteristics of the 27 patients with JIA
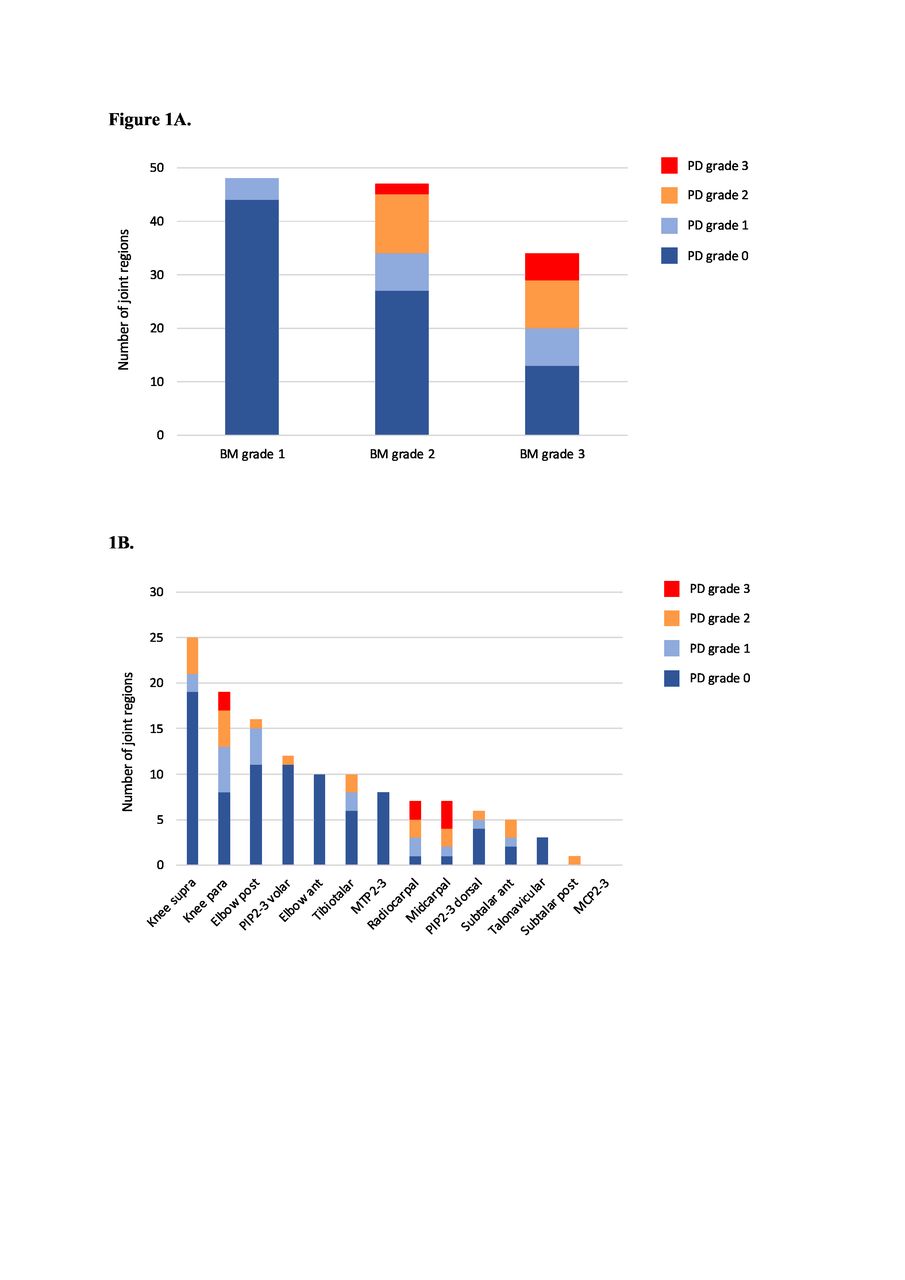
Abnormal PD signals were present in 45 of 129 joint regions with BM synovitis (34.9%), of which 18, 20 and 7 joint regions had PD grades 1, 2 and 3, respectively. Of the 129 joint regions with BM synovitis, 84 of 129 joint regions (65.1%) did not have PD findings (PD grade=0). PD grade 1 was found in 4 of 48 (8.3%), 7 of 47 (14.9%) and 7 of 34 (20.6%) joint regions with BM grades 1, 2 and 3, respectively. PD grades 2 and 3 were only present in joint regions with BM grades 2 and 3(figure 1A). Increasing PD grades were associated with higher BM grades (OR 5.0, 95% CI 2.7 to 9.1, p<0.001). Additional adjustment for age and sex did not alter the results (data not shown).

(A). Power Doppler (PD) ultrasound findings (grades 0–3) in 129 joint regions with B-mode (BM) synovitis (grades 1–3) in patients with juvenile idiopathic arthritis (JIA). (B). Distribution of PD ultrasound findings (grades 0–3) in 129 joint regions with BM synovitis in patients with JIA. ant, anterior; MCP, metacarpophalangeal; MTP, metatarsophalangeal; para, parapatellar recess; PIP, proximal interphalangeal; Post, posterior; supra, suprapatellar recess.
Converted
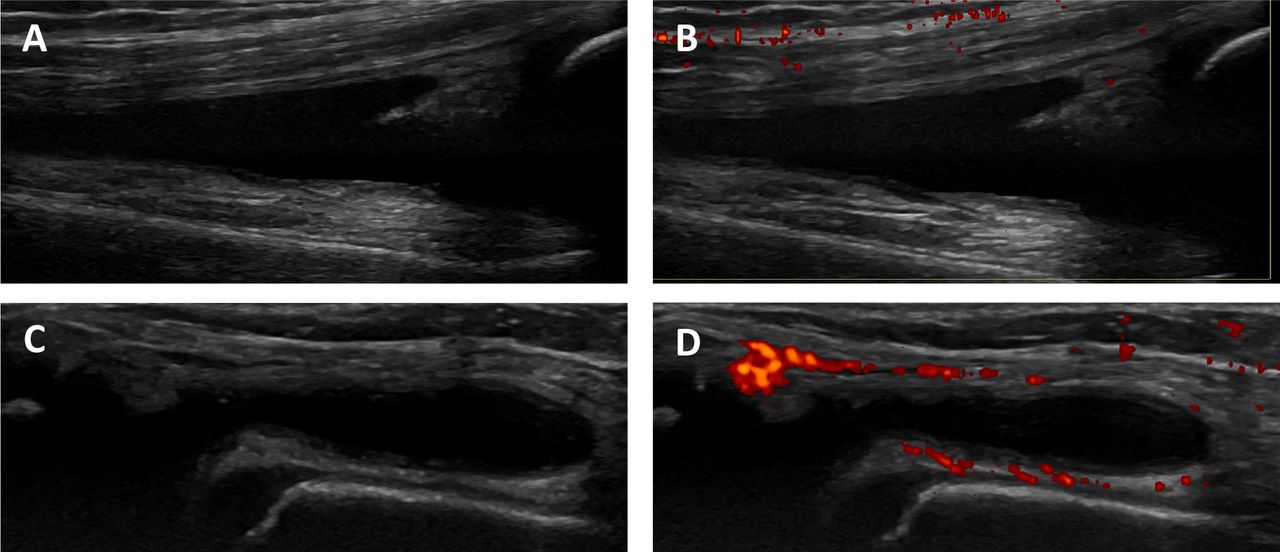
The lateral parapatellar recess of the knee was the joint region with most PD findings (11 of 45 joint regions (24.4%)), followed by the radiocarpal (6 of 45 joint regions (13.3%)), the midcarpal (6 of 45 joint regions (13.3%)) and the suprapatellar recess of the knee (6 of 45 joint regions (13.3%)). The joint region with most findings of BM synovitis without abnormal PD signals was the suprapatellar recess of the knee (19 of 84 joint regions (22.6%)). Synovitis based on BM findings without PD findings and synovitis based on BM and PD findings are illustrated in figure 2. There were no BM or PD findings in the MCP2 or MCP3 joints. Distribution of PD findings (grades 0–3) in the 129 joint regions with BM synovitis are illustrated in figure 1B.

{kind=link}
{kind=link}
Illustration of variations in power Doppler (PD) ultrasound findings in two joint regions of the knee in a 10-year-old with juvenile idiopathic arthritis (JIA). Longitudinal dorsal scan of the knee joint (suprapatellar recess) showing B-mode (BM) synovitis (A), and BM synovitis without abnormal PD signals (grade 0) (B). Longitudinal dorsal scan of the knee joint (lateral parapatellar recess) showing BM synovitis (C), and BM synovitis with abnormal PD signals (grade 3) (D).
Of joint regions with PD grades 1, 2 and 3, clinical arthritis was present in 13 of 18 (72.2%), 17 of 20 (85.0%) and 7 of 7 (100.0%), respectively. Of joint regions considered as clinical arthritis, 37 of 78 joint regions (47.4%) had PD findings. The lateral parapatellar recess of the knee had the highest frequency of PD findings (10 of 37 (27.0%)), followed by the radiocarpal (6 of 37 (16.2%)), the midcarpal (6 of 37 (16.2%)) and the suprapatellar recess of the knee (6 of 37 (16.2%)) in joints with clinical arthritis. Increasing PD grades were significantly associated with the presence of clinical arthritis (OR 7.4, 95% CI 2.6 to 21.0, p<0.001). Additional adjustment for age and sex did not alter the results (data not shown).
Abnormal PD signals were present in all age groups. Joint regions with PD findings were seen in 9 of 27 (33.3%), 11 of 35 (31.4%), 14 of 27 (51.9%) and 11 of 40 (27.5%) in the age groups 2–4, 5–8, 9–12 and 13–18 years, respectively. Boys had PD findings in 13 of 32 joint regions (40.6%) whereas girls had PD findings in 32 of 97 joint regions (33.0%). Oligoarthritis was the JIA subgroup that had most PD findings (29 of 73 joint regions (39.7%)), followed by polyarthritis rheumatoid factor (RF) positive (10 of 33 joint regions (30.3%), polyarthritis RF negative (5 of 17 joint regions (29.4%) and psoriatic arthritis (1 of 6 joint regions (16.7%)). Joint regions with PD findings were seen in 1 of 6 (16,7%), 27 of 68 (39.7%) and 9 of 33 (27.3 %) in the minimal, moderate and high disease activity groups, respectively. Cross-sectional associations were not found between PD findings and age, sex, JIA subgroups, disease duration or JADAS10.
Discussion
This is the first study to investigate associations between PD grades and BM grades and the presence of clinical arthritis in multiple joint regions using a standardised scanning protocol and a joint-specific scoring system for synovitis with reference atlas for patients with JIA. On joint level, increasing PD grades were strongly associated with higher BM grades. We also demonstrated a clear association between increasing PD grades and the presence of clinical arthritis. This suggests that the scoring system corresponds well with the severity of synovitis.
The preliminary ultrasound definitions for synovitis in children emphasise that synovitis can include BM findings alone, but not PD findings alone.12 In our study, we found many joint regions with BM synovitis without abnormal PD signals. This could represent residual findings of previous active arthritis,23 or that our patients had a low-grade severity arthritis. It could also indicate that BM synovitis alone without PD findings is more common in patients with JIA, or that synovial effusion without synovial hypertrophy is a prominent feature in joints with active arthritis since Doppler signals must be detected within synovial hypertrophy to be considered as a sign of synovitis.
 In joint regions that had PD findings, most had findings of clinical arthritis. The knee, radiocarpal and midcarpal joints had the highest frequency of PD findings in joints with clinical arthritis. The wrist joint is difficult to evaluate clinically and has been identified as an indicator of poor outcome and a vulnerable site of structural damage.24 25 Ultrasound can be an important and helpful tool in the evaluation of this joint as ultrasound has been shown to be more sensitive than clinical examination in the evaluation of joint inflammation in peripheral joints.26 Our findings might suggest that the presence of abnormal PD signals is a sign of disease severity, but longitudinal studies are needed to examine this further.
In joint regions that had PD findings, most had findings of clinical arthritis. The knee, radiocarpal and midcarpal joints had the highest frequency of PD findings in joints with clinical arthritis. The wrist joint is difficult to evaluate clinically and has been identified as an indicator of poor outcome and a vulnerable site of structural damage.24 25 Ultrasound can be an important and helpful tool in the evaluation of this joint as ultrasound has been shown to be more sensitive than clinical examination in the evaluation of joint inflammation in peripheral joints.26 Our findings might suggest that the presence of abnormal PD signals is a sign of disease severity, but longitudinal studies are needed to examine this further.
We found that increasing PD signals were associated with the presence of clinical arthritis, but not with the composite disease activity score JADAS10. This could be because clinical joint examination and ultrasound evaluate the precise site of inflammation, while the JADAS measures the disease activity more widely and may also be affected by confounding factors. Other studies have reported poor correlation between ultrasound findings and JADAS.7 In this study, we explored associations on joint level, if we had investigated on patient level with ultrasound sum scores, we might have obtained other results. This could be addressed in a future study.
We found a high number of PD findings in the lateral parapatellar recess of the knee joint. The highest number of BM synovitis without PD findings was found in the suprapatellar recess of the knee joint. This may be because the parapatellar recess is more superficial than the suprapatellar recess and therefore easier to detect Doppler signals there. This supports the added value of scanning both the suprapatellar and the parapatellar recess when evaluating the knee joint with ultrasound in children, as has also been suggested by others.21
We did not find BM synovitis, and therefore, no abnormal PD signals, in the MCP joints. This was unexpected since these joints are superficial and PD findings are then often easier to interpret, in addition, the MCP2 joint is often affected in patients with JIA.6 27 28 This could be a random finding in our sample, but the small size of the joint, few vessels and slow blood flow velocity could have made it difficult to evaluate. However, we did find synovitis in the PIP joints which are even smaller. The PIP joints were assessed from both the dorsal and volar views. The MCP joints were only evaluated from the dorsal view. In adults with RA, a dorsal approach is recommended over the volar approach to evaluate finger joints with ultrasound.29 To our knowledge, this has not been investigated in children, and the use of only the dorsal or both the dorsal and the volar approaches are inconsistent.12 27 28 30 In a clinical setting it can be difficult to evaluate several joints from more views because young children are often impatient. Larger studies to evaluate the different views to include for each joint are needed.
A clear definition of abnormal Doppler signals and a scoring system for Doppler findings is important to discriminate between physiological and pathological vascularisation in children.1 12 Magni-Manzoni et al evaluated patients with JIA in remission and found that patients with PD findings had less flares than patients without PD findings.31 However, most of the PD signals were found in the youngest patients and were scored as a grade 1 and may have represented normal vascularisation. In a study evaluating physiological Doppler signals in healthy children, most Doppler signals were detected in the age group 2–12 years.5 We were concerned that physiological Doppler signals in the youngest age groups could affect our interpretation of abnormal PD signals. However, when performing the ultrasound examinations this was not an issue. This could be because the ultrasonographer only considered Doppler signals within synovial hypertrophy as pathologic in accordance with the preliminary definitions for synovitis in children,12 and because a standardised scanning approach and scoring system with reference atlas were used during the examinations.14 In this study, most PD findings were seen in the age group 9–12 years old, but no significant association between PD findings and age was found.
There are some limitations in this study. First, the study was cross-sectional. Consequently, we cannot say anything about the longitudinal associations between PD findings and measures of disease activity, but this was outside the scope of this study. Second, we did not include healthy controls to investigate BM and PD findings in healthy children. It can, therefore, be difficult to conclude with what is a normal finding. However, the purpose of this study was to describe PD findings in joint regions with BM synovitis on ultrasound in patients with JIA, and since Doppler signals must be within synovial hypertrophy to be considered as a sign of synovitis, joint regions without BM synovitis were excluded. Another limitation is that only one rheumatologist performed the ultrasound examinations. The ultrasonographer in this study has shown moderate to excellent inter-reader reliability in a previous ultrasound study.14 In addition, it is challenging and not feasible to perform several ultrasound examinations in children. Another limitation of this study is the limited number of patients. This might explain why we did not detect pathological ultrasound findings in the MCP2-3 joints, and that there were few findings in some joints. Since the patients in this study were consecutively included from our inpatient and outpatient clinic, we believe that our sample is representative of patients with JIA seen in clinical practice. However, larger studies are needed to explore all joints that can be affected in JIA. Finally, we did not use other modalities like dynamic contrast-enhanced MRI to compare our findings. This should be addressed in a future study.
The strengths of this study include the use of the same ultrasound machine in all assessments, that the ultrasonographer was blinded to clinical findings, and that multiple joint regions were evaluated in a live-exercise. In addition, the image acquisition protocol and the joint-specific scoring system for synovitis with reference atlas ensured a standardised examination and scoring in all patients.
In conclusion, we found that increasing PD grades were significantly associated with higher BM grades and with the presence of clinical arthritis, suggesting that PD signals detected using a standardised ultrasound examination and scoring system can reflect active disease in patients with JIA. However, further studies are needed to understand more about the clinical implications of Doppler findings in these patients.
Data availability statement
Data are available on reasonable request. Quantified ultrasound data may be available on reasonable request, but patients’ data are not publicly available.
Ethics statements
Patient consent for publication
Ethics approval
The study was approved by the Norwegian Regional Committee for Medical and Health Ethics (REK 2018/805) and done in accordance with the Declaration of Helsinki. Signed informed consent was obtained by patients and/or parents.
Acknowledgments
The authors thank all the patients and their families who contributed to this study. The support from the Norwegian Rheumatism Association and the Simon Fougner Hartmann’s Family Foundation is gratefully acknowledged by the authors.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors NKS designed the study, made substantial contribution to acquisition, analyses and interpretation of data, and writing the manuscript. PB and VL designed the study and made substantial contributions to acquisition and interpretation of data and writing the manuscript. BF, A-BA and EK participated in the study design and made substantial contributions to acquisition of data and writing the manuscript. All authors read and revised the article critically and approved the final manuscript. PB is the guarantor of the study.
Funding This study was funded by the DAM foundation.
Competing interests A-BA reports personal fees from Abbvie, personal fees from Eli Lilly, personal fees from Novartis and personal fees from Pfizer.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.