Article Text

Abstract
Objectives We studied patterns of joint inflammation in juvenile idiopathic arthritis (JIA) to assess whether joint activity recurs locally in the same joints.
Methods Joints of 91 patients of the BeSt for Kids study, a treat-to-target trial for children with recent-onset oligoarticular, rheumatoid factor-negative polyarticular and psoriatic JIA, were clinically assessed during 2 years (10 study visits). The association between joint inflammation at baseline and later inflammation in the same joint was assessed using a multilevel mixed-effects logistic regression model at joint level. With a Poisson model, the association between baseline joint inflammation and the number of study visits at which the same joint was recurrently inflamed was tested.
Results Of the 6097 joints studied, 15% (897) was clinically inflamed at baseline. In 42% (377/897) of those joints, inflammation recurred during follow-up. Joint inflammation at baseline was statistically significantly associated with joint inflammation during follow-up in the same joint (OR 3.9, 95% CI 3.5 to 4.4) and specifically with the number of episodes of recurrent joint inflammation (IRR 1.6, 95% CI 1.2 to 2.1).
Conclusion In JIA, joint inflammation has the tendency to recur multiple times in joints that are clinically inflamed at disease onset. This indicates that local factors might play a role in the processes contributing to the occurrence of JIA flares.
- Juvenile Idiopathic Arthritis
- Synovitis
- Inflammation
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Juvenile idiopathic arthritis (JIA) often has a relapsing/remitting disease course. Previous assessment of large joint pairs suggested a tendency for local recurrence of joint inflammation.
WHAT THIS STUDY ADDS
We showed that in children with JIA, clinical joint inflammation is more likely to recur in initially affected joints, indicating the presence of local factors influencing the susceptibility for recurrence of inflammation of a joint.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
These results emphasise the need for further research of local factors in arthritic joints as potential treatment targets and imply that prevention of recurrence of arthritis demands more intensive (local or systemic) treatment.
Introduction
Juvenile idiopathic arthritis (JIA) describes a cluster of arthritides in children that persist for more than 6 weeks with an unknown origin.1 Treatment may be local, for instance with intra-articular glucocorticoids, or systemic, with disease-modifying antirheumatic drugs (DMARD).
Currently, guidelines recommend to start treatment of oligoarthritic JIA with intraarticular glucocorticoids (with or without non-steroid anti-inflammatory drugs).2 However, local relapses occur in up to 20% of joints within 3 months postinjection.3 When systemic antirheumatic treatments are also used, minimal disease activity has been reported in 55% of patients with oligoarthritis after 2 years.4 For children with polyarthritis systemic treatment, aimed at minimal or no disease activity, may be sufficient. The use of intraarticular glucocorticoids in these patients is debated.5
Despite treatment, joint inflammation may persist or recur. Adjustment of treatment strategies or even development of new treatments may depend on identification of persistent systemic inflammatory processes or local factors at joint level. It was previously suggested that such local factors are present in JIA. For example, local presence of tumor necrosis factor α and interleukin 6 may promote chronic inflammation by hindering suppression of inflammation by regulatory T-cells in the joint.6 Furthermore, the composition of synovial fluid was found to be predictive for severity of the disease course of oligoarticular JIA.7
To investigate whether joint inflammation recurs locally or at random locations over time in JIA, we performed a post hoc subanalysis at joint level in the BeSt for Kids study, where systemic treatment adjustments were aimed at achieving inactive disease. We also describe local joint activity in relation to joint damage.
Methods
Patients
We used data from the BeSt for Kids study, a multicenter randomised, single blind treat-to-remission strategy study in 92 DMARD-naive patients with non-systemic JIA (oligoarticular, rheumatoid factor (RF)-negative polyarticular and psoriatic JIA) and a symptom duration <18 months. Treatment arms were (1) initial treatment with methotrexate or sulfasalazine, followed, in case of insufficient response, by dose increase and, subsequently, etanercept, (2) initial treatment with methotrexate in combination with prednisolone bridging, if necessary followed by DMARD dose increase and subsequently etanercept and (3) initial combination treatment with etanercept and methotrexate, if necessary followed by the treatment choice of the treating physician. Follow-up was 2 years. The treatment target was an ACRPedi50 response at 3 months and inactive disease (modified Wallace 2004 definition4) at 6 months and further. Treatment was tapered after inactive disease was achieved (for at least 3 months in oligoarticular and 6 months in polyarticular JIA). Clinical assessments were done at baseline, 6 weeks and every 3 months until end of follow-up. The BeSt for Kids study has been described in more detail previously.4 8
Patient and public involvement
Patients nor public were involved in the design, execution or analysis of the original study, nor in the current subanalysis.
Joint assessment
At each study visit, joint assessments of 67 joints were performed by trained research nurses or physical therapists. A joint was considered clinically inflamed if it was scored as ‘active arthritis’.
Persistent joint inflammation was defined as active arthritis in the same joint at two or more subsequent study visits. Recurrent joint inflammation was defined as active arthritis in the same joint after a period (≥1 visits) of absence of arthritis. A period of one or more subsequent study visits at which a joint was (persistently) active was called a ‘joint inflammation episode’. In case of missing joint assessments, the joints were considered non-active.
Radiographic joint damage assessment
Joint damage was measured in wrist joints with the Poznanski score.9 Radiographs were taken in 57 (63%) participants. All available radiographs were assessed by two observers, with an intraclass correlation coefficient of 0.999.10 A negative Poznanski Z-score indicates delayed radiometacarpal bone growth, associated with loss of cartilage and joint space narrowing. A positive Z-score is associated with early ossification of carpal bones. As arbitrary cut-offs to include limited damage, we used a Z-score of <−0.25 and >0.25, respectively. As a sensitivity analysis, we used <1 and >1 as cut-offs for damage that may be more clinically relevant.
Statistical analysis
Joint-level description of inflammation
Joint activity at baseline and during follow-up was described at the level of individual joints for the three different JIA categories.
Association between baseline joint inflammation and local joint inflammation during follow-up
To investigate whether joints that are clinically inflamed have a higher risk of later inflammation, we studied the association between baseline joint activity and joint activity in the same joint during follow-up with a multilevel mixed-effects logistic regression model (model 1). Joints were clustered within patients. The model was adjusted for joint location and the time point (study visit) of the joint assessment.
To assess whether an association between baseline and later clinical joint inflammation was a specific within-joint association, a permutation test was performed.11 Scores of baseline joint activity were permuted (shuffled) within each patient after which the analysis was repeated. The permutation was repeated 1000 times. A statistically significant result (p<0.05) indicates that the association between baseline and later joint inflammation is stronger in the original model (activity compared within the same joint) than in the permutations (activity compared across random other joints), suggesting a local effect. A 95% CI for this p value is provided to describe the uncertainty of the outcome, provided only a part (1000) of all possible combinations has been tested.12
In several exploratory analyses, we assessed possible factors that might influence local joint inflammation patterns.
Since the association between baseline and later local joint inflammation might be different between JIA categories, an interaction between baseline joint activity and JIA category was added to model 1. If the interaction was statistically significant, indicating a different association between JIA categories, a stratified analysis was performed, meaning we ran the model separately for each JIA category.
For evaluation of a possible effect of treatment on the association between baseline and later local joint inflammation, an interaction between baseline joint activity and treatment group was added, with stratification in case of a statistically significant association.
The association between baseline joint inflammation and later local inflammation in the same joint might also differ between joints. Therefore, an interaction between baseline joint activity and joint location was tested. The right wrist was chosen as the reference group because it was often assessed as active in all JIA categories.
In case of analyses in which stratification was used, joints in which neither at baseline nor at follow-up arthritis was observed were excluded from the analysis.
Association between baseline joint inflammation and recurrent local joint inflammation during follow-up
To study whether joint inflammation recurs in the same joints after absence of joint inflammation, model 1 was subsequently stratified for joint activity at the previous study visit.
In addition, a Poisson model with joints clustered within patients was performed to study the association between baseline joint inflammation and the number of recurrent joint inflammation episodes, adjusted for joint location and time point. A permutation test was performed to assess the specificity of the results. Furthermore, we added an interaction term to the model between baseline joint inflammation and the JIA category and in a second modification of the model an interaction between baseline joint inflammation and treatment group, as exploratory analyses. In case of a statistically significant result, we stratified the analysis.
Association between duration of baseline joint inflammation and later joint inflammation
The effect of duration of baseline joint inflammation on occurrence of later joint inflammation was studied in joints that were active at baseline. A variation of model 1 was used, with duration of baseline joint inflammation instead of presence of baseline joint inflammation (yes/no) as a dependent variable.
Sensitivity analyses
To exclude the possible effect of frequency of inflammation of certain joints, we repeated model 1 in the 25% most often inflamed joints (ankles, knees, wrists, elbows, shoulders, metacarpophalangeal joints 2–3, proximal interphalangeal joints 2–3). In addition, a permutation test was performed in the most often inflamed joints to further study whether an association between baseline and later local joint inflammation was determined by higher susceptibility to inflammation of certain joints or by higher susceptibility for inflammation after previous inflammation.
To further account for the differences in the general probability of certain joints to become inflamed at all, we also performed a permutation test for model 1 in which joint scores were permuted within strata of joint pairs (left and right side) of a patient.
To account for a potential influence of mechanical stress on susceptibility for joint inflammation, we adjusted model 1 for whether a joint was weight bearing (as a proxy for mechanical stress; hips, knees, ankles, subtalar joints, midtarsal joints, metatarsophalangeal joints and interphalangeal joints of the feet were regarded as weight bearing).
Sensitivity analyses accounting for missing observations in different ways were done for all models. First, joints were regarded as non-active in case of missing assessments before end of follow-up. Second, we used an adjusted form of last observation carried forward: the last observation (activity yes/no) was only carried forward for missing values in case the observation previous to the missing time point corresponded with the observation at the time point after the missing observation.
Joint inflammation and radiographic outcomes
Presence of joint activity during follow-up was described for joints with a positive and negative Poznanski Z-score at the last available wrist radiograph. A generalised linear mixed model was used to assess the association between joint inflammation during follow-up (yes/no) in a wrist joint and its Z-score. Wrist joints were clustered within patients and the model was adjusted for the baseline Z-score.
All analyses were performed in Stata V.SE 16.1.
Results
Of the 92 patients of the BeSt for Kids study, one patient had no follow-up information available after baseline and was excluded from this analysis. Of the remaining patients, 12% (11) had oligoarticular, 79% (72) polyarticular RF-negative and 9% (8) psoriatic JIA. At baseline, the patients had a median (IQR) age of 9 (5–13) years, 66% (60) were female and the mean (SD) symptom duration was 8.5 (4.7) months. The mean (SD) JADAS 10 score at baseline was 18.0 (4.8) with median (IQR) 8 (5–12) active joints. All but two patients had 2-year follow-up joint assessment data available. During follow-up, 89 patients (98%) had inactive disease (of whom 35 were drug free) at least once, and 51 patients (56%) achieved persistent (≥6 months) remission.
Joint-level description of inflammation
Of the 6097 joints (91 patients) studied, 897 (15%) were active at baseline. Of these 897 joints, 419 (47%) were persistently active from baseline until at least the second study visit (6 weeks after baseline). After the baseline inflammation episode, 377 joints (42%) were recurrently active (that is, after a period of absence of arthritis in that joint) during follow-up. The distribution of active joints at baseline and recurrence of activity during follow-up is illustrated in figure 1. The joint involvement pattern differed between the three included JIA categories.

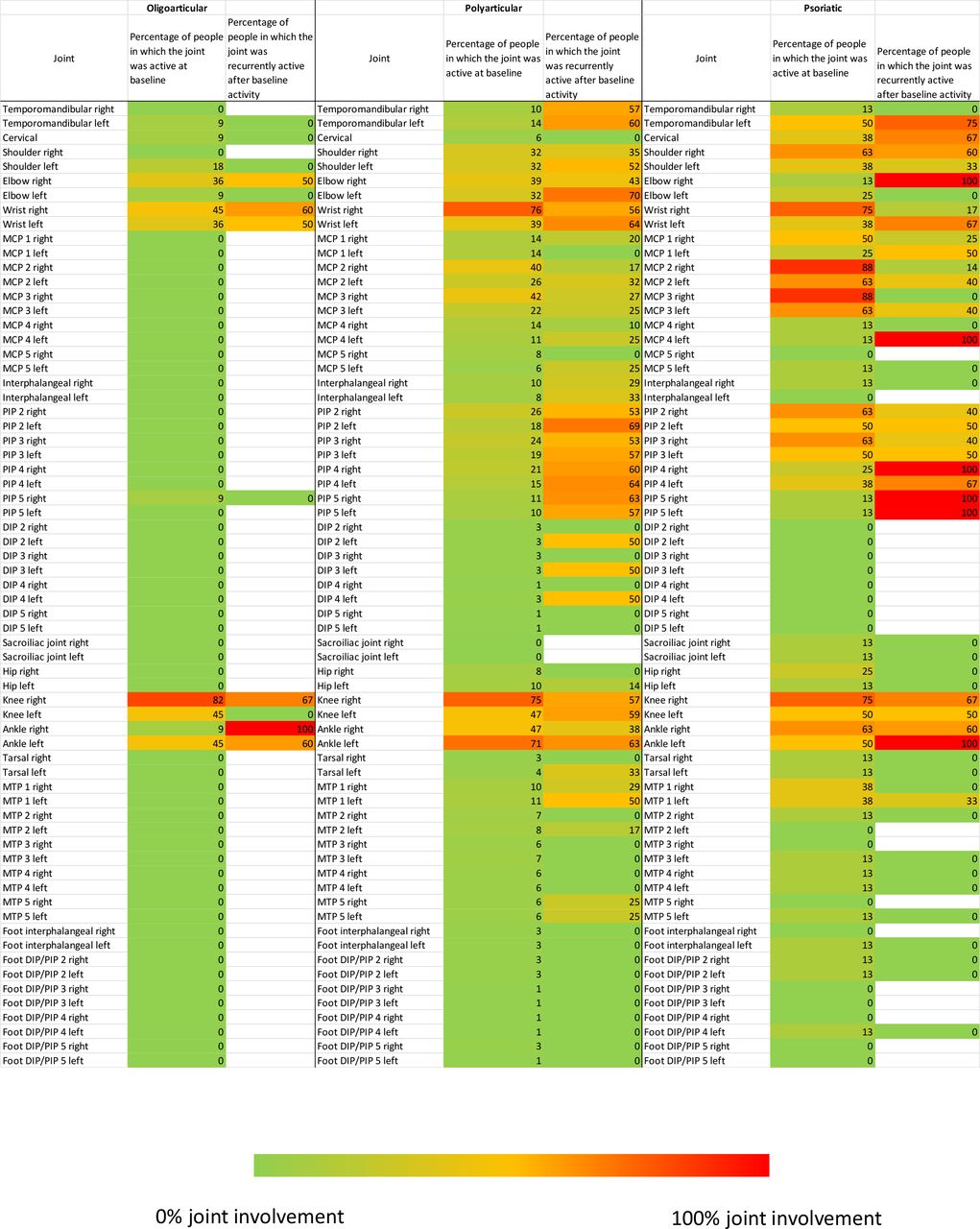{kind=link}
Joint inflammation patterns in the three JIA types (oligoarticular, n=11 ; RF-negative polyarticular, n=72, psoriatic, n=8) included in the BeSt for Kids study. MCP, metacarpophalangeal; PIP, proximal interphalangeal; DIP, distal interphalangeal; MTP, metatarsophalangeal
Of the 5200 joints that were not active at baseline, 561 (11%) became active during follow-up. In patients who had a flare of disease activity after (the first time) inactive disease was reached, 1195 (93%) of the 1280 joints that became inflamed had also been inflamed before the first period of inactive disease. Joint inflammation after the first period of drug-free inactive disease occurred in the same joint in 96% (485/507) of the joints.
Association between baseline joint inflammation and local joint inflammation during follow-up
We found a statistically significant association between baseline joint inflammation and inflammation in the same joint during follow-up with an OR of 3.9 (95% CI 3.5 to 4.3), that is, the odds of joint inflammation during follow-up were approximately four times higher in joints that were already inflamed at baseline, depending on the time point and joint location. The permutation test showed that inflammation during follow-up in a certain joint was better predicted by baseline inflammation of the same joint, than by baseline inflammation of randomly selected other joints (p<0.001, 95% CI 0 to 0.004).
Because of a statistically significant (p<0.001) interaction between baseline joint inflammation and JIA category, a stratified analysis was performed, showing a positive association between baseline and later local joint inflammation in all three categories, although to a different extent (table 1).
Association between baseline joint inflammation and joint inflammation in the same joint during follow-up within three different JIA categories
A statistically significant interaction (p=0.02) between baseline joint inflammation and the treatment strategy arm was also found. The stratified analysis showed that the association between baseline and later local joint inflammation was present in all three arms and was strongest in the arm starting with monotherapy, with a statistically significant difference between the monotherapy arm and the treatment arm starting with methotrexate with prednisolone bridging (table 2).
Association between baseline joint inflammation and joint inflammation in the same joint during follow-up within the three BeSt for Kids treatment strategy arms
The interaction between baseline joint activity and joint location was also statistically significant (p<0.001), indicating that the association between baseline and later local joint inflammation is different for different joints.
Association between baseline joint inflammation and recurrent local joint inflammation during follow-up
Baseline joint inflammation was not only associated with local joint inflammation during follow-up in general (persistent+recurrent inflammation) but also for recurrent joint inflammation in particular: stratification for inflammation in the joint at the previous study visit showed an OR of 2.6 (95% CI 2.3 to 3.1) for joints without inflammation at the previous study visit (recurrent inflammation) and an OR of 1.4 (95% CI 1.1 to 1.7) for joints with inflammation at the previous study visit (persistent inflammation).
Baseline inflammation in a joint was also associated with the number of joint inflammation episodes in that joint during follow-up (IRR 1.6, 95% CI 1.3 to 2.1), and specificity of this finding was confirmed by the permutation test (p<0.001, 95% CI 0 to 0.004). No statistically significant interactions between baseline joint inflammation and JIA category or treatment group were found for this analysis.
Association between duration of baseline joint inflammation and later joint inflammation
We found no statistically significant association between the duration of inflammation that was present at baseline and later joint inflammation in the same joint (OR 1.00 per week, 95% CI 0.98 to 1.00).
Sensitivity analyses
The association between baseline and later local joint inflammation in joints that were most often active (in other words, more susceptible for inflammation in general) was similar to the association in the main model (OR 3.3, 95% CI 2.9 to 3.8). The result of the permutation test (p<0.001, 95% CI 0 to 0.004) indicated that this association is local rather than general.
Permutation within joint pairs yielded the same results as the original permutation test, indicating that baseline joint inflammation of the contralateral joint was not as predictive for later inflammation as baseline inflammation of the joint itself.
Adjustment of model 1 for whether a joint was weight bearing or not yielded the same results as the unadjusted model.
Until end of follow-up, 3% of the observations (1673/60 970) was missing. The results of the sensitivity analyses accounting for missing assessments in two different ways were similar to the results of the original models (online supplemental data 1).
Supplemental material
Joint inflammation and radiographic outcomes
For the assessment of radiographic joint damage, Z-scores measured between year 1 and 2 were available for 94 wrist joints. Baseline assessment was available in 65 of these joints. The median (IQR) Z-score in the 94 joints was −0.16 (−0.64 to 0.53). The percentage of joints that was ever active until the last radiographic assessment with an abnormal Z-score was comparable to the percentage of ever-active joints with a normal Z-score (table 3). With +/−1 as Z-score cut-offs only 22% of the joints were regarded as abnormal and the percentage of ever-active joints with an abnormal Z-score was somewhat lower than the percentage in joints with normal Z-scores (table 3). We found no statistically significant association between joint inflammation of a wrist joint and its Z-score (β 0.17, 95% CI −0.06 to 0.41).
Wrist joint activity during follow-up and radiographic assessment
Discussion
In 91 children with non-systemic JIA that were treated to target for up to 2 years, we showed that clinical joint inflammation tends to recur in the same joint. Local joint inflammation at baseline was associated with occurrence of joint inflammation in that same joint during follow-up as well as with the number of times that joint was recurrently inflamed. In 42% of the joints that were inflamed at baseline, joint inflammation recurred. Joint inflammation during follow-up was more strongly associated with baseline joint inflammation of that same joint than of other joints. These results indicate that in patients with JIA, besides systemic inflammatory effects, the occurrence of joint inflammation over time might be partly determined by local factors that are affected by previous inflammation.
A tendency for recurrence of joint inflammation was also observed in rheumatoid arthritis.13 Furthermore, in an observational study, in adult patients with persistent JIA disease activity laterality of joint inflammation was often preserved if unilateral joint inflammation reoccurred after the patient achieved inactive disease, and it was reported that the majority of joint regions that became inflamed during a flare after the disease was inactive had been inflamed before.14 Likewise, the type of joint involvement pattern in children with JIA has been shown to be often maintained over time.15 In contrast to patients with rheumatoid arthritis, where presence of inflammation in a joint has been linked to radiographic joint damage,16 17 we did not find an association between inflammation in a wrist joint and the Poznanski score for radiographic wrist damage in this JIA population. This might be interpreted as a success of treat-to-target therapy, resulting in very little damage, but the observation period of 2 years might also have been too short to detect an association between inflammation and damage.
In our study, joint inflammation recurrence in JIA was investigated at a joint level while considering the dependency of joints within each patient and the overall chance of the joint becoming inflamed. Another strength is the use of clinical trial data: joints were regularly assessed, and the examinations were performed by a limited number of trained staff, limiting heterogeneity of assessments. Moreover, few data were missing (3/92 dropouts and 3% missing data points within follow-up). In case of missing data, sensitivity analyses were performed, confirming the results of the main analysis.
Limitations include the absence of long-term follow-up data and the fact that we only studied the association between baseline and later joint inflammation. Therefore, we cannot make a statement about recurrence of joint inflammation that debuted later in the disease course. We can also not infer the absence or presence of clinical joint inflammation between two study visits, although this probably did not affect the results considerably because of the frequent (3 monthly) study visits. Additionally, only clinical joint assessment was performed, so persistent subclinical joint inflammation in periods of apparent absence of arthritis cannot be ruled out
The fact that we found a tendency for local recurrence in JIA indicates that there are local aspects influencing joint inflammation, which are not yet all elucidated. One could argue that, from the beginning of the disease, certain specific joints could be more susceptible to inflammation than others. This resonates with the clinical distinction between types of arthritis with different joint inflammation patterns. Mechanical stress has been associated with joint inflammation.18 However, it is not likely to (fully) explain the recurrence of inflammation, since adjustment for weight bearing did not change our results. Another hypothesis for local recurrence of inflammation is ‘tissue priming’: in rodent arthritis models, it has been shown that a joint can become more prone to inflammation as a consequence of previous inflammation, although in these models, the effect of systemic inflammatory triggers was not tested.19 Synovial fibroblasts that acquire a more pathogenic phenotype after inflammatory priming are found to play an important role in the process of tissue priming.19 Another finding is that synovial resident memory T cells can remain in the joint during remission after previous inflammation.20 21 These T cells may further accumulate each time a joint is inflamed.22
We found a stronger association between baseline and later local inflammation in JIA patients with polyarticular arthritis than with psoriatic arthritis. Although the number of patients with psoriatic JIA was relatively low in our cohort and the analysis was of exploratory nature, this might indicate that local effects are less strong in psoriatic JIA. Since the current classification of JIA is partly based on clinical features, it would be interesting to assess whether the association between baseline and later inflammation differs between categories that are based more on pathophysiological differences. We also found that the association between baseline and later inflammation differed between the treatment arms. The association was strongest for the arm in which the patients started with monotherapy. No differences were found when assessing the number of joint inflammation episodes after baseline. Since in the latter analysis only recurrence, and not persistence, of joint inflammation is assessed, it is possible that the difference between treatment arms is mainly caused by the duration of joint inflammation from baseline, which might have been a consequence of a slower treatment effect in arm 1 and, therefore, more persistence of joint inflammation. However, this hypothesis is based on exploratory analyses. Also, the clinical outcomes at patient level were not statistically significantly different between the three treatment arms.8
If local factors play a role in chronicity of local inflammation, in addition to systemic treatment, local treatment may help to prevent recurrence of joint inflammation. However, previous research suggests that effects of current intra-articular treatment such as glucocorticoid injections and synovectomy are only temporary.14 23
In conclusion, we found that in JIA, joints that are previously inflamed are more likely to be inflamed during 2-year follow-up, indicating a local effect that increases the susceptibility of a joint to future inflammation. Although the distribution of joint involvement varied between the included JIA categories, the association between baseline and later local joint inflammation was present in oligoarticular, polyarticular as well as psoriatic JIA. Joint inflammation had the tendency to recur multiple times in the same joint after a period of absence of local inflammation. Therefore, there might be a need for even more intensive treatment of (local) JIA disease activity to prevent recurrent joint inflammation. Moreover, these local effects might be a target for new therapies.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Medisch Ethische Toetsingscommissie Leiden (p.09.034).Written Informed consent was obtained from patients above 12 years of age and parents of all participating patients before taking part.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors Concept and design: SLH, PCEH-M, CFA and SAB. Acquisition of data: PCEH-M, JMvdB, DS-M, LWAvS-S, MAJvR, YK-K, RtC and DMCB. Analysis and interpretation: SLH, CFA and SAB. Drafting the manuscript: SLH, CFA and SAB. Revising the manuscript critically: all authors. Guarantors: SLH, SAB and CFA.
Funding The original BeSt for Kids study received financial support from Pfizer. The authors, not the sponsors, were responsible for the study design, the collection, analyses and interpretation of all data, the writing of this article and the decision to publish.
Competing interests The original BeSt for Kids study received financial support from Pfizer.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.