Article Text

Abstract
Objective To assess polypharmacy in women and men with psoriatic arthritis (PsA).
Methods From the German BARMER health insurance database, 11 984 persons with PsA and disease-modifying antirheumatic drug therapy in 2021 were included and compared with sex-matched and age-matched controls without inflammatory arthritis. Medications were analysed by Anatomical Therapeutic Chemical (ATC) groups. Polypharmacy (≥5 concomitant drugs) was compared by sex, age and comorbidity using the Rheumatic Disease Comorbidity Index (RDCI) and the Elixhauser Score. The mean difference in the number of medications between persons with PsA and controls was estimated using a linear regression model.
Results Compared with controls, all ATC drug classes were significantly more frequent in persons with PsA, most commonly musculoskeletal (81% vs 30%), immunomodulatory (56% vs 2.6%), cardiovascular (62% vs 48%), alimentary tract/metabolic (57% vs 31%) and nervous system (50% vs 31%) drugs. Polypharmacy was significantly higher in PsA (49%) compared with controls (17%), more frequent in women (52%) compared with men (45%) and strongly increased with age and comorbidity. For each unit increase of the RDCI, the age-adjusted number of medications increased by 0.98 (95% CI 0.95 to 1.01) units in men and 0.93 (95% CI 0.90 to 0.96) units in women. Compared with controls, the number of medications in PsA (mean 4.9 (SD 2.8)) was 2.4 (95%CI 2.34; 2.43) units higher in women and 2.3 (95% CI 2.21 to 2.35) units higher in men.
Conclusions Polypharmacy is common in PsA and is composed of PsA-specific medication as well as frequent medications for comorbidities, equally affecting women and men.
- Psoriatic Arthritis
- Arthritis, Psoriatic
- Health services research
- Antirheumatic Agents
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Patients with psoriatic arthritis (PsA) have a high burden of comorbidity. Little data exist regarding polypharmacy.
WHAT THIS STUDY ADDS
Polypharmacy affects almost half of all women and men with PsA and exceeds the amount in individuals without inflammatory arthritis.
Polypharmacy is composed of PsA-specific, pain-related and comorbidity-related medication.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Polypharmacy needs to be addressed in PsA to avoid sequelae.
It should be investigated whether the use of analgesics, glucocorticoids and further comedication could be reduced by more frequent biological disease-modifying antirheumatic drug therapy.
Introduction
For the therapy of psoriatic arthritis (PsA), a rising number of disease-modifying antirheumatic drugs (DMARDs) are available today. They are used in monotherapy or in combination with non-steroidal anti-inflammatory drugs (NSAIDs) and/or conventional synthetic (cs)DMARDs. In addition to the antirheumatic drugs, medications are often prescribed to treat concomitant diseases, to prevent certain conditions such as osteoporosis and to manage pain.1 Patients with PsA are at high risk of developing comorbidities, in particular metabolic syndrome,2 implying a significant impact on medication use. PsA therapy and comorbidity almost inevitably lead to the issue of polypharmacy, which itself may further challenge the management of the disease. The most commonly reported definition of polypharmacy is the numerical definition of five or more medications daily.3 Data on polypharmacy in patients with inflammatory rheumatic diseases are mainly available from patients with rheumatoid arthritis (RA). In RA, polypharmacy is common and associated with higher age, female sex, multimorbidity, disease activity, disease duration and functional impairment.4 For persons with psoriasis, European data also indicate a higher comedication burden compared with controls.5 6 There is a lack of data on polypharmacy in PsA.
In a German study, 42% of the population aged 65 years and older met the definition of polypharmacy and 20%–25% received potentially inadequate medication.7 The most commonly prescribed potentially inadequate medicines in elderly patients include cardiovascular, sedatives and sleeping agents, antiarrhythmics and antidepressants.7 These medications also relate to comorbidities that are common in PsA. For patients with PsA, German data are available for PsA-specific pharmacotherapy and for treatment persistence8 9 but not for polypharmacy. Since the majority of the comedications are prescribed by general practitioners,7 a data source containing all prescriptions is necessary to adequately analyse polypharmacy in PsA. Therefore, we used data from a large nationwide German statutory health insurance fund to assess the age-related, sex-related and comorbidity-related frequency of polypharmacy in individuals with PsA compared with controls without inflammatory arthritis.
Methods
Data source
We used BARMER cross-sectional claims data for the complete year of 2021. The BARMER statutory health insurance fund is one of the largest health insurance companies in Germany and covers around 8.8 million people, corresponding to 12% of all inhabitants with a statutory health insurance. Around 73 million people (90%) of the German population are members of a statutory health insurance. Germany has universal healthcare with a multipayer system. It is possible to change between statutory health insurance funds every 18 months. There are differences between German statutory health insurances with respect to morbidity,10 thus, representativeness for the total German population is limited. The validity of PsA diagnoses has not been investigated in these data. For RA, 81% of the persons with two German modification of the International Statistical Classification of Diseases (ICD-10-GM) codes of M05 or M06 in a large survey confirmed the diagnosis and 7.2% had another inflammatory rheumatic disorder, predominately PsA.11
Inclusion criteria
Persons aged ≥18 years who were continuously insured in 2021 and had either an outpatient diagnosis in at least two quarters of 2021 or one inpatient diagnosis of psoriasis (L40) and PsA (M07.0–3+L40.5) according to the ICD-10-GM, plus at least one prescription for DMARD therapy (Anatomical Therapeutic Chemical (ATC) codes see online supplemental table 1) in 2021, were included. This algorithm to identify patients with PsA in claims data was validated by Lee et al.12 Psoriasis (L40) was selected as inclusion criterion to increase the specificity of the PsA diagnosis in distinction to other overlapping rheumatic diseases, especially RA. DMARD-therapy was also required to increase specificity, accepting loss of sensitivity. A 100% coverage of all persons with PsA was not a priority for this analysis. Diagnoses of Crohn’s disease (K50), ulcerative colitis (K51) and ankylosing spondylitis (M45) were identified as concomitant conditions and were not excluded due to overlapping manifestations. Diagnoses of RA (M05, M06) were also identified but not excluded as especially the M06 code (‘other polyarthritis’) is often also documented in PsA.
Supplemental material
According to the updated GRAPPA treatment recommendation for PsA,13 we considered the following DMARD therapies: csDMARDs, namely methotrexate (MTX), sulfasalazine, leflunomide, ciclosporin A, the tumour necrosis factor inhibitors etanercept, adalimumab, golimumab, certolizumab and infliximab, the CTLA4-immunoglobulin fusion protein abatacept, the interleukin inhibitors (IL-12/23i: ustekinumab, IL-17i: secukinumab, ixekizumab, IL-23i: guselkumab), the phosphodiesterase inhibitor apremilast and the januskinase inhibitors tofacitinib and upadacitinib (ATC codes, see online supplemental table 1).
A control group matched by sex and age 1:10 was randomly selected in the population without any diagnoses of RA, PsA or axial spondyloarthritis in the complete year 2021 as defined in the inclusion criteria.
Comedication and comorbidity
We identified all drugs by ATC codes within the claims data, prescribed at least once in 2021, and assigned them to ATC groups as proposed by the Classification System of the WHO Collaborating Center for Drug Statistics Methodology.14 The defined daily doses (DDDs) dispensed are reported, providing information on the assumed average maintenance dose per day for a drug used for its main indication. Applying DDDs allows to make international comparisons.15
Comorbidities were identified by ICD-10-GM codes and are reported according to the Rheumatic Disease Comorbidity Index (RDCI),16 which has been used for PsA patients.17 18 The RDCI includes the following conditions: lung disease, myocardial infarction, other cardiovascular disease, stroke, hypertension, fracture (of hip, leg or spine), diabetes mellitus, depression, cancer, ulcus and other stomach problems. The included ICD-10-GM codes are reported in online supplemental table 1. In addition to the RDCI, we looked for the presence of renal failure, hypothyroidism, osteoporosis, osteoarthritis, obesity, liver disease, dementia and gout. We also used the ICD-10-GM codes to calculated the Elixhauser comorbidity Score19 for comparison with controls. It can also be used to compare results with other administrative data analyses. All ICD-10-GM and ATC codes are reported in online supplemental table S1). Specialist care was identified by physician specialist numbers (rheumatology 31, dermatology 21) and specific billing codes for rheumatology.
Statistical analysis
We provide all results stratified by sex and age. The extent of comorbidity, drug prescriptions and polypharmacy were compared with controls. To define polypharmacy, we identified the month with the highest number of medications in 2021 for each person. For this analysis, only prescriptions with DDDs >30 were considered to exclude short-time medication from the total medication estimates. We also used the DDDs to estimate the proportion of PsA-specific medication out of the total medication. The mean number of medications is reported by sex and age groups, and by RDCI and Elixhauser Scores. Polypharmacy was defined by five or more drugs in any month of 2021.3
As there was frequent overlap between PsA and RA diagnoses, a sensitivity analysis was performed excluding persons with an additional RA diagnosis. In order to reflect a possible bias due to the selected inclusion criteria, the frequency of polypharmacy was also calculated for the group with PsA diagnosis but without any DMARD prescription in 2021 and for the group with PsA diagnosis when including persons without psoriasis.
We used a linear regression model with age as a covariate to estimate the mean difference in number of medications between the PsA and control groups. We fitted separate models for women and men. The number of medications was modelled as n(meds)=age+age×control+control.
The research paper was written in accordance with the REporting of studies Conducted using Observational Routinely collected Data guideline.20
Patient and public involvement
Within the framework of the TARISMA (Targeted Risk Management in Musculoskeletal Diseases)research project, three patient research partners have accompanied our research from application to implementation (see the Acknowledgement section).
Results
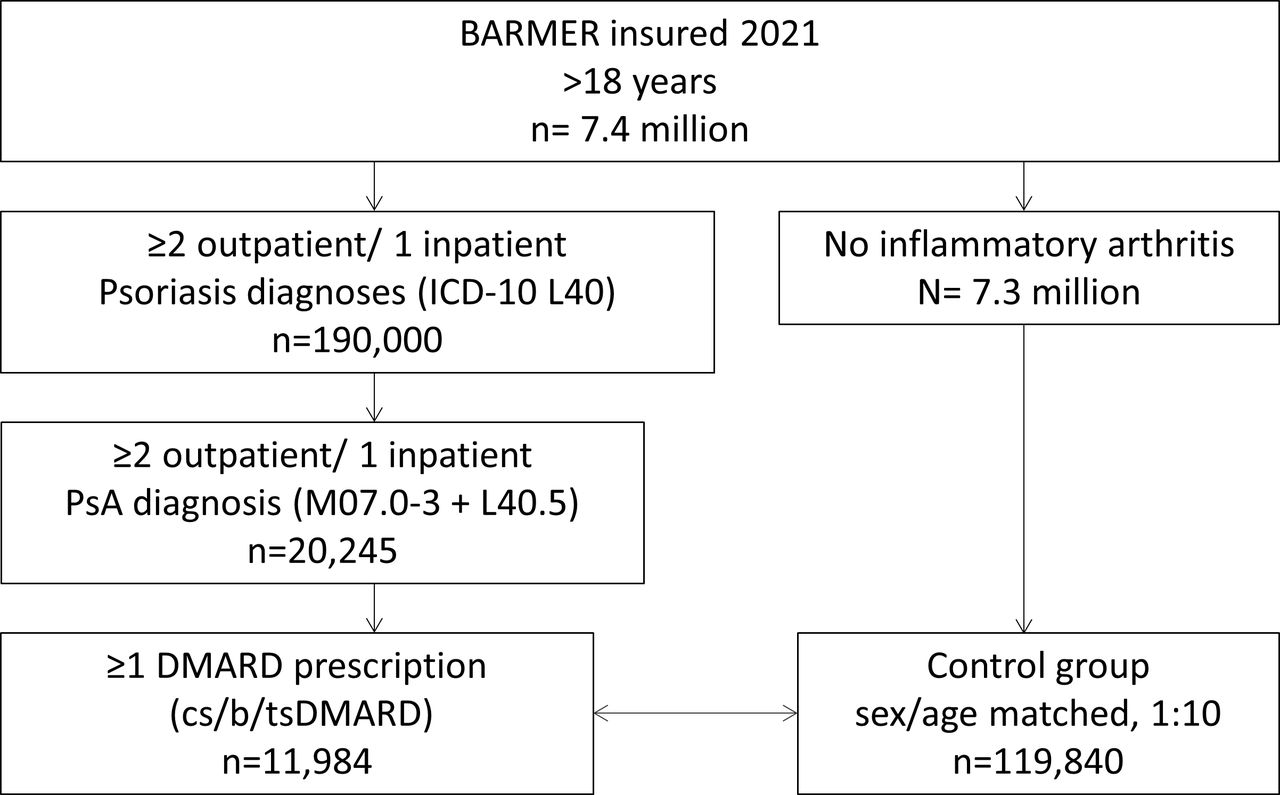
From all adult persons insured in 2021 (n=7.4 million), 190 000 (2.6%) had a diagnosis of psoriasis (L40). Of those, 20 245 (11%) also had a PsA diagnosis (L40.5+M07.0–3), and 11 984 of those received any DMARD therapy. A total of 119 840 persons without diagnoses of inflammatory arthritis were included as controls (figure 1).

Flow chart. DMARD, disease-modifying antirheumatic drug; ICD-10, nternational Classification of Diseases 10th Revision.
Characteristics
A total of 63% of all persons with PsA and DMARD therapy were women and the overall mean age was 60 years. Associated autoimmune conditions were diagnosed for axial spondyloarthritis (6%), Crohn’s disease/Colitis ulcerosa (2%) and iridocyclitis (1%). A diagnosis of RA was documented in 37%, more frequently in women (41%) than in men (29%) and more common in older persons (23% in 18–30 years, 50% in >80 years) than in younger. Seropositive RA (M05) was diagnosed in 7% while 93% had unspecific M06 codes (‘other chronic polyarthritis’).
A total of 68% of persons visited a rheumatologist in 2021; subdivided into 40% who saw a rheumatologist only and the remaining 28% who visited both a rheumatologist and a dermatologist. Sixteen per cent only saw a dermatologist while another 16% did not see either specialist in 2021. Contacts with specialists were similar within sex and age groups (table 1, online supplemental table 2).
Characteristics of persons with PsA and controls
Comorbidities
Comorbidity was more frequent in PsA compared with controls (mean Elixhauser comorbidity score 3.6 vs 2.2 in controls). This applies to the characteristics of the metabolic syndrome: hypertension (57% vs 42% in controls), dyslipidaemia (32% vs 27%), obesity (22% vs 11%), diabetes (21% vs 13%) as well as to all other comorbidities except dementia, in particular osteoarthritis (35% vs 15%) and depression (28% vs 16%). Men more often had dyslipidaemia (36% vs 31%), cardiovascular disease (21% vs 14%) and gout (8% vs 2.7%) than women. In contrast, women more often had lung disease (22% vs 16%), depression (32% vs 21%), hypothyroidism (26% vs 9%), osteoporosis (18% vs 7%) and osteoarthritis (39% vs 28%) than men (table 1). Comorbidities strongly increased with age, from a mean RDCI of 0.4 for those aged 18–30 to 3.0 for those aged above 80 (online supplemental table S2). For the individual comorbidities, the sex ratio and also the age distribution were comparable in persons with PsA and controls, with a higher overall comorbidity burden in PsA (figure 2,online supplemental figure 1 for controls).

Comorbidities in women and men with psoriatic arthritis by age groups. The figures indicate the percentage of persons in the respective group who have the comorbidity diagnosis. For example, 83.9% of women aged >80 years with PsA have a diagnosis of hypertension. PsA, psoriatic arthritis.
Prescribed drugs
All drugs prescribed in 2021 are reported by ATC groups in table 2. Compared with controls, all ATC drug classes were prescribed relevantly more often in persons with PsA. The largest amounts were attributable to the musculoskeletal (81% vs 30%) or the cardiovascular system (62% vs 48%), immunomodulating agents (56% vs 2.6%), treatments for alimentary tract and metabolism (57% vs 31%) and the nervous system (50% vs 31%). Women more often had prescriptions for antiulceratives (45% vs 36%), analgesics (43% vs 31%) and antidepressants (24% vs 14%). With higher age, the prescription of antihypertensives, diabetes medication and lipid-lowering agents increased in both women and men. Older men were more often prescribed gout medication and older women were more often prescribed thyroid medication (figure 3).
Proportion of persons with a PsA diagnosis with at least one prescription for the respective drug in 2021 in %

Prescribed drugs in women and men with psoriatic arthritis by age groups. The figures show the percentage of persons in that group with at least one prescription of the respective drug in 2021. For example, 65.7% of men with PsA aged 18–30 years had a prescription of bDMARDs in 2021. bDMARDs, iological disease-modifying antirheumatic drug; PsA, psoriatic arthritis.
Specific DMARD therapy was prescribed similarly in women and men. In total, 62% had a csDMARD, predominately MTX (55%) and 49% had a bDMARD, 67% in monotherapy. TNF inhibitors were the most frequently prescribed among the b/tsDMARDs (30%), followed by IL17 inhibitors (15%). All DMARD prescriptions are reported in table 3. While csDMARDs and analgesics, as well as opioids, were prescribed more frequently at older ages, bDMARDs were used much less frequently regardless of sex (69% in 18–30 years, 27% in >80 years.) or specialist care. Women received analgesics more often than men, while glucocorticoids were prescribed more frequently for men in the older compared with the younger age groups (figure 3). Compared with controls, women and men with PsA were prescribed opioids 2–3 times more frequently in the older age groups (online supplemental figure 2). Opioid prescriptions were comparable in individuals with PsA if a rheumatologist was involved compared with patients without rheumatology care: 7% vs 5% in 18–30 years to 28% vs 33% in >80 years. The prescription of antidepressants was twice as high in PsA compared with controls, in particular in the middle-aged groups (29% in women with PsA vs 14% in female controls aged 51–60 years) (see figure 3).
Proportion of persons with a PsA diagnosis with at least one prescription for the respective DMARDs in 2021 in %
Polypharmacy
Polypharmacy was relevantly higher in persons with PsA (49%) compared with controls (17%), more frequent in women (52%) compared with men (45%) and strongly increased with age (15% in 18–30 years, 78% in >80 years) and comorbidity. In the group of PsA without DMARDs (n=8261), 38% were affected by polypharmacy. In the group of PsA without psoriasis (n=847), 49% were affected by polypharmacy.
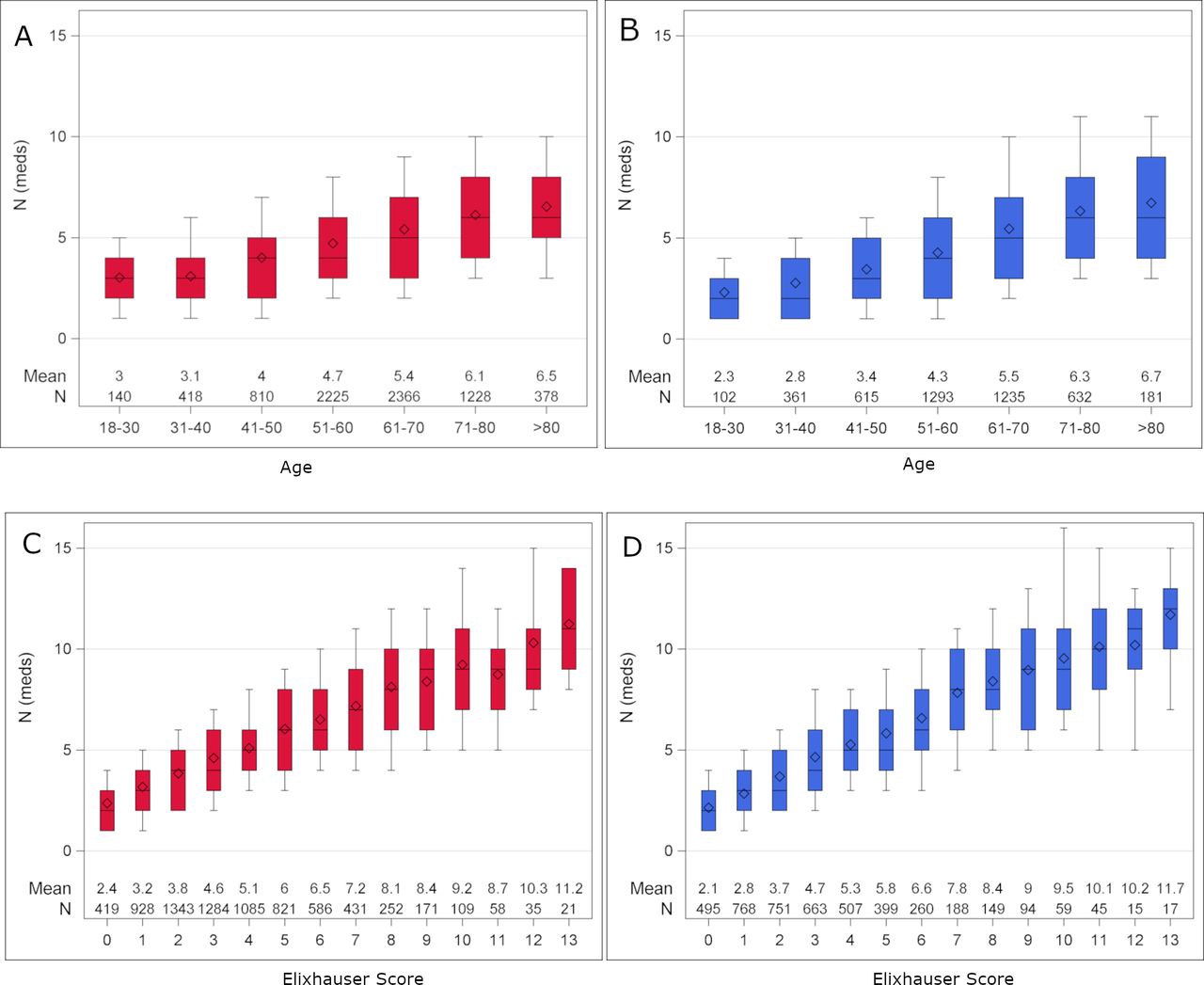
Box plots show the distribution of the number of medications according to age, sex and comorbidity (figure 4). In all age groups and comorbidity levels, the mean number of medications was higher in women and men with PsA than in controls (online supplemental figure 3). For each unit increase of the RDCI, the age-adjusted number of medications increased by 0.98 (95% CI 0.95 to 1.01) in men and 0.93 (95% CI 0.90 to 0.96) in women. For each unit increase in the Elixhauser index, the age-adjusted number of medications increased by 0.66 (95% CI 0.64 to 0.68) in men and by 0.64 (95% CI 0.62 to 0.65) in women with PsA.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Distribution of the number of medications according to age groups and Elixhauser Score. Boxplots are shown, the diamond marks the arithmetic mean. (A) Women with PsA by age groups. (B) Men with PsA by age groups. (C) Women with PsA by Elixhauser score. (D) Men with PsA by Elixhauser score. PsA, psoriatic arthritis.
The DDDs are reported in online supplemental table 3. They refer to the persons to whom the corresponding drug was prescribed in 2021. They serve as an orientation, which medications were given continuously. The mean proportion of DDDs of systemic PsA-specific medication (glucocorticoids, b/ts/csDMARDs, NSAIDs) of all DDDs was 38% (median 30%, 1. quartile 16%, 3. quartile 54%). That means that on average, PsA medication accounted for 38% of the medication in this cohort.
The mean number of drugs with prescription of >30 DDDs at the same time was 4.9 (SD2.8) in PsA compared with 2.3 (2.5) in controls. The number of medications in persons with PsA as compared with controls was 2.4 (95% CI 2.34 to 2.43) units higher in women and 2.3 (95% CI 2.21 to 2.35) units higher in men. There was no relevant age trend. In 40 years, the difference was 2.9 (95% CI 2.8 to 3.0) in women and 2.4 (95% CI 2.3 to 2.5) in men. For those aged 70 years, the difference was 2.7 (95% CI 2.7 to 2.8) in women and 2.4 (95% CI 2.2 to 2.5) in men (table 4).
The difference in number of medications (standard deviation) of persons with a PsA diagnosis and controls stratified by age: results from separate linear models
Sensitivity analysis
The PsA cohort without additional M05/M06 (RA) ICD-10-GM diagnosis (n=7612) had less women (59% vs 63%), was slightly younger (mean age 59 years vs 60 years) and had slightly less comorbidities (mean RDCI 1.7 vs 1.9, mean Elixhauser 3.1 vs 3.6) compared with the total PsA cohort (table 1). Polypharmacy was slightly less often present in the PsA cohort without RA diagnosis (45% vs 49%). Prescriptions by ATC groups were comparable in both cohorts (table 2). This also applies to the prescription of glucocorticoids (31% in the PsA cohort without RA codes). DMARD therapy was equally distributed with minor deviations, for example, MTX 55% vs 54%, bDMARDs 49% vs 50%, TNF inhibitors 30% vs 29% (table 3). The differences to the control group regarding the proportion of specific comorbidities, comedication and the number of medications in relation to age, sex and comorbidity were equally distributed (data not shown). The mean number of drugs with prescription of >30 DDDs at the same time was 4.6 (SD2.7) in the PsA cohort without RA codes.
Discussion
This study investigated the extent of polypharmacy in women and men with PsA, taking age and comorbidities into account. The results show that polypharmacy is significantly more common in persons with PsA than in individuals without diagnosis of an inflammatory arthritis. PsA-specific medication contributes to polypharmacy, as does the higher amount of medication attributable to the increased burden of comorbidities in PsA.
In Germany, around 20% of persons with psoriasis are diagnosed with PsA after rheumatological examination.21 22 The proportion of 11% with PsA diagnosis among persons with psoriasis that we found in the claims data fits well to these numbers as undiagnosed PsA may be present in a number of cases which was not considered in this study. According to the Berlin Ageing Study, 24% of the predominantly healthy participants (with a mean age of 69 years) are affected by polypharmacy which was defined as the concomitant use of at least five drugs.23 Taking into account the age of the cohort, the proportion of polypharmacy is very comparable to that in our control group, strengthening the clear difference to individuals with PsA.
For PsA, little data are available regarding polypharmacy. At the EULAR Congress 2022, a Turkish study reported 84% of PsA patients (n=73) with polypharmacy 6 months after treatment onset.24 For psoriasis, comprehensive data are available from Sweden, showing that individuals with psoriasis also had an increased risk of having dispensed drug prescription for almost all ATC groups studied with higher mean numbers of different drugs (mean 7.7–9.5, depending on psoriasis severity, psoriasis medication excluded) compared with controls (mean 5.1).5 A relationship between polypharmacy and poorer treatment response as well as more serious adverse events25 and hospitalisations26 have been shown in RA. Thus, there is a need to address polypharmacy to improve clinical outcomes in PsA as well. The FORTA (Fit fOR The Aged) List for German speaking countries addresses both overtreatment and undertreatment, irrespective of disease.27 It can be used to manage polypharmacy for the individual patient, especially in the elderly.
What could the rheumatologist contribute? Our data show that PsA medications account for almost 40% of prescribed drugs. While DMARD therapy is essential to prevent subsequent damage, systemic glucocorticoids should be avoided in PsA and analgesics may be dispensable if PsA is well controlled. According to current treatment recommendations, there is no rationale to use systemic glucocorticoids in PsA.1 However, in our analysis, these were prescribed to 35% of all persons with PsA. Our results also show substantially more frequent prescriptions of analgesics including opioids in individuals with PsA compared with controls. Better control of PsA disease activity could help to reduce the number of medications needed.
Medication for comorbidities make up the largest portion in our analysis of polypharmacy. A well-controlled PsA helps to reduce secondary conditions such as depression, cardiovascular disease, osteoporosis or osteoarthritis, all of which occurred more frequently in PsA than in controls. Cardiometabolic diseases are associated with the extent and severity of PsA and they can influence treatment outcomes.28 As is the case with psoriasis,29 pharmacologically treated depression is more common in individuals with PsA compared with controls. It is noticeable that the proportion of persons with PsA on bDMARD therapy decreases sharply with age. With regard to drug interactions and the risk of infections, effective bDMARD monotherapy could be preferable to conventional therapy with csDMARDs, NSAIDs, analgesics or systemic glucocorticoids.
Women and men with PsA did not differ considerably with regard to polypharmacy. Women were slightly more likely to have five or more medications and had a slightly higher mean number of medications (the contraceptive pill and oestrogen replacement were included). Several concomitant diseases are represented differently in women and men, which is also reflected in the frequency of the corresponding medication group. Overall, however, polypharmacy was present regardless of sex.
Limitations and strengths
There was large overlap of PsA and (seronegative) RA diagnoses. Without a clinical validation, PsA cannot be fully differentiated from RA since both diseases are largely treated with the same drugs. M06 codes are often used as unspecific code for suspected arthritis, and in many cases the code remains in the data after a specific diagnosis has been made.11 Minor differences in the results of the sensitivity analysis indicate that we presumably also included some RA cases but the results do not differ relevantly with regard to the amount of polypharmacy. Comorbidities are captured by billing codes and not by clinical assessments. With regard to obesity, under-reporting is to be assumed since obesity does not necessarily need to be recorded as a billing diagnosis.Our data do not contain over-the-counter (OTC) medications. We had surveyed people diagnosed with RA in a prior study and found that 31%–58% took additional OTC medications, depending on pain intensity.30 Thus, the evaluation of prescription-only medicines does not fully reflect the proportion of polypharmacy leading to an underestimation of the proportion of persons with polypharmacy. In a German nursing home study, 74% of the residents received at least one OTC drug as scheduled medication.31
With almost 12 000 individuals, our data cover a broad nationwide DMARD-treated population with a PsA diagnosis. Strengths of the claims data include the possibility to identify sex-matched and age-matched controls with standardised recording of comorbidities by the Elixhauser Score. The biggest advantage of our data source is the complete coverage for all prescribed medicine.
In summary, polypharmacy is a major burden for people with PsA, resulting from both PsA therapy and medication for comorbidities. The majority of older persons with PsA are affected by polypharmacy, this applies equally to women and men. In the elderly, more frequent therapy with bDMARDs should be considered, which may result in reduced use of analgesics, opioids and other secondarily induced comedications.
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information.
Ethics statements
Patient consent for publication
Ethics approval
The study was approved by the ethics committee of the Charité-Universitätsmedizin Berlin (EA2/233/22).
Acknowledgments
The authors thank the BARMER for providing access to data via their data warehouse for this study. We thank the research partners Peter Böhm, Andrea-Dagmar Quiring and Julius Wiegand in the TARISMA project for dedicating their time to add the patient view to this project.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @callhoffj
KA and ACR contributed equally.
Contributors JC is responsible for the overall content as guarantor. KA, ACR and JC conceived the idea for the article. UM and JC were involved in data acquisition. KA, ACR, AS and JC designed the study, planned analyses and interpreted the results. JC extracted the data and performed the analyses. KA wrote the first draft of the manuscript. All authors critically reviewed the manuscript and agreed with the submission. JC had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Funding The study was supported by the Federal Ministry of Education and Research within the network TARISMA [01EC1902A].
Competing interests A.R. received speaker fees from lectures for BMS, Novartis, Pfizer, and Roche, all unrelated to this manuscript. J.C. received speaker fees from Janssen-Cilag GmbH. A.S. received speaker fees from lectures for AbbVie, Celltrion, MSD, Roche, BMS, Lilly and Pfizer, all unrelated to this manuscript. K.A. has no conflicts of interest. U.M. is an employee of the BARMER. There were no financial and personal relationships with other people or organizations that could inappropriately influence (bias) this work.
Patient and public involvement statement Within the framework of the TARISMA research project, three patient research partners have accompanied our research from application to implementation
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.