Article Text

Abstract
Methotrexate is associated with bone lesions that are rare and, although presenting with a typical localisation to the lower extremities and appearing with a characteristic radiologic morphology, largely unknown and often misdiagnosed as osteoporotic insufficiency fractures. The correct and early diagnosis, however, is key for treatment and prevention of further osteopathology. Here, we present a patient with rheumatoid arthritis who developed multiple painful insufficiency fractures in the left foot (processus anterior calcanei, tuber calcanei) and in the right lower leg and foot (anterior and dorsal calcaneus and at the cuboid and distal tibia) during therapy with methotrexate, which were all misdiagnosed as osteoporotic. The fractures occurred between 8 months and 35 months after starting methotrexate. Discontinuation of methotrexate resulted in rapid pain relief and no further fractures have occurred. This case powerfully demonstrates the importance of raising awareness of methotrexate osteopathy in order to take appropriate therapeutic measures, including and perniciously discontinuing methotrexate.
- Methotrexate
- Arthritis, Rheumatoid
- Arthritis
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
(MTX) can cause insufficiency fractures, especially in the lower limbs.
WHAT THIS STUDY ADDS
Rising the awareness for MTX associated osteopathy by demonstrating the occurence of four fractures in a single lower limb.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Joint-related complaints may be misinterpreted as rheumatic disease activity or osteoporotic osteopathy. Awareness of MTX-induced osteopathy is necessary to prevent further bone defects.
Introduction
Methotrexate (MTX) is established as first-line therapy for inflammatory rheumatic diseases such as rheumatoid arthritis1 and others. It has anti-inflammatory and immunomodulatory effects by inhibiting ribonucleotide transformylase and intracellular accumulation of adenosine.2 However, effects such as inhibition of osteoblast differentiation and prevention of osteoclast activation have also been described,3 4 which may lead to disturbances in bone homeostasis and stability. Indeed, there is an increasing number of case reports of MTX-induced osteopathy manifesting as insufficiency fractures in patients with inflammatory rheumatic diseases. However, MTX-induced osteopathy is often misdiagnosed, resulting in continued MTX therapy, which prevents healing and promotes further bone pathology. Awareness of MTX-induced osteopathy, therefore, needs to be raised.
Case report
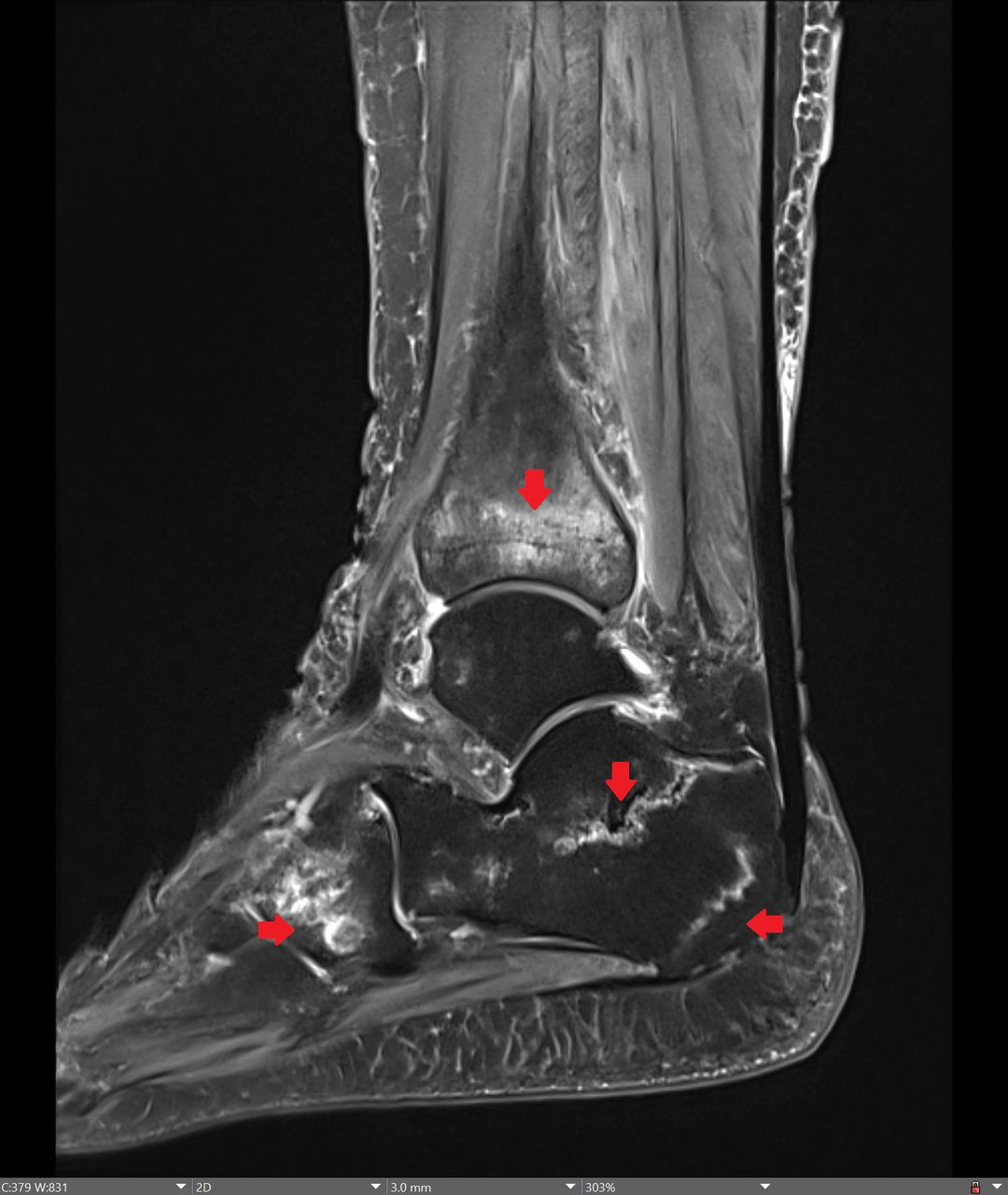
We report the case of a 73-year-old woman who presented to our clinic with three independent episodes of foot exertional pain. Seven years earlier, she had been diagnosed with rheumatoid arthritis, which was treated intermittently with prednisolone. Four years after the onset of the disease, MTX (15 mg/once weekly, s.c.) was started with very good clinical success. Simultaneously, alendronate was started to treat osteoporosis (lowest T-score from the lumbar spine, femoral neck and total <−2.8) that had caused multisegmental thoracic vertebral body sintering. Five additional thoracic vertebral body fractures occurred during the first 3 months of bisphosphonate treatment. In June 2020, 8 months after starting therapy with methotrexate, an MRI was performed due to pain in the right foot, which revealed a calcaneal fracture. It was suspected at that time that the fracture was due to osteoporosis. Alendronate was exchanged for denosumab for some weeks, followed by romosozumab (the complete timeline of the antirheumatic and antiosteoporotic therapy is presented in online supplemental figure 1). In October 2021, the T-score had increased to – 2.0, suggesting a halt of bone loss and osteoporotic therapy was modified from romosozumab to denusomab. In May 2022, left foot pain occurred, and an MRI showed two new fractures in the left calcaneus. In August 2022, the patient presented again with right foot pain, but in a hospital in France. There, only an X-ray of the foot was taken without evidence of fractures. In September 2022, in our hospital, an MRI showed additional insufficiency fractures in the anterior and dorsal calcaneus, cuboid and distal tibia with a ligamentous or meandering appearance (arrows in figure 1). There was no history of trauma. The diagnosis of MTX-induced osteopathy was made based on the localisation, fracture distribution and morphology, which were atypical for osteoporotic lesions, but characteristic for MTX-associated osteopathy. Retrospectively, the first fracture that occurred as early as 8 months after the initiation of MTX therapy was also considered to be MTX associated, not at last because of its typical MRI pattern (online supplemental figure 2 PLEASE exchange the text of supplementat figure 2: Heading: MRI of the right foot at the time of the occurrence of the first fracture; PLEASE NAME THE FIRST PICTURE (A); FOOTING: PLEASE REMOVE T1-weighted imaging, PLEASE ADD: Sagittal contrast enhanced T1-fat-saturated sequence. PLEASE NAME THE SECOND PICTURE (B); FOOTING: PLEASE REMOVE T2-weighted imaging, PLEASE ADD: Sagittal proton density fat-saturated sequence. Discontinuation of MTX resulted in spontaneous disappearance of the pain and halted further fractures. With respect to her rheumatoid arthritis, the patient is in complete remission under treatment with tocilizumab in the usual weekly dose of 162 mg.
Supplemental material
Supplemental material

{kind=link}
MRI of the right foot (Sagittal proton density fat-saturated sequence): insufficiency fractures at the anterior and dorsal calcaneus, cuboid and distal tibia with band-shaped or meander-shaped appearances. Arrows indicate the fracturzones
Discussion
MTX-induced osteopathy is a rare side effect of MTX. It was first described in the 1970s in children with leukaemia.5 Meanwhile, case reports of MTX osteopathy are also accumulating in patients with inflammatory rheumatic diseases.6 7 The insufficiency fractures in the context of MTX osteopathy typically occur at the lower extremity,6 as in our patient. They manifest in descending order at the distal tibia, calcaneus, proximal tibia, tarsus and metatarsus.6 The case presented here is the first case with multiple pathognomonic fractures of the lower extremity.
The differential diagnosis of MTX osteopathy includes osteoporotic insufficiency fractures, and in fact approximately 50% of the patients from the case reports also suffered from underlying osteopenia or osteoporosis.6 7 Whether patients with MTX-induced osteopathy are at increased risk for osteoporis is currently unknown as the number of cases reported do not allow such a calculation. However, typical localisation in the lower extremity and characteristic radiological morphology (eg, pathognomonic type of stress fractures with band-shaped or meander-shaped apperance along the growth plate) as illustrated in our case should raise the suspicion of MTX-associated osteopathy.
The bone-destructive effects of MTX on bone metabolism have been extensively described in vitro.3 It can be assumed that suppression of new bone formation and inhibition of osteoblast differentiation may lead to an imbalance in bone that ultimately results in insufficiency fractures. However, the exact mechanisms of MTX-induced osteopathy remain unclear.
Treatment of MTX-induced osteopathy should begin with immediate discontinuation of MTX. In case reports, rapid and complete disappearance of pain and other symptoms occurred after discontinuation of MTX.6 7 In our patient, lower limb pain also disappeared several weeks after discontinuation of MTX.
In conclusion, MTX is associated with osteopathy, although the mechanism is currently unknown. Treatment involves discontinuation of MTX, but the diagnosis is often overlooked because awareness of MTX-induced osteopathy is low and, therefore, MTX is continued. The patient presented here is a striking illustration of the typical manifestation of MTX-induced osteopathy, and the case may help to raise awareness of this rare side effect of MTX.
Ethics statements
Patient consent for publication
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors None.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.