Article Text

Abstract
Background To examine radiographic axial damage of the sacroiliac joints and spine in patients with psoriatic arthritis (PsA) and spondyloarthritis (SpA) in private and academic Belgian practices.
Methods Patients with PsA with clinical diagnosis of PsA and fulfilling the Classification Criteria for Psoriatic Arthritis from the prospective Belgian Epidemiological Psoriatic Arthritis Study and patients with SpA fulfilling the Assessment of SpondyloArthritis international Society classification criteria for SpA originate from the Ghent and BelGian Inflammatory Arthritis and spoNdylitis cohorTs were included in this study. Baseline pelvic and spinal radiographs were analysed by two calibrated readers. Blinded for the origin of the cohort or clinical data readers assessed the modified Stoke Ankylosing Spondylitis Spine Score (mSASSS) and modified New York criteria on spinal and pelvic radiographs, respectively. Data were compared between both patient groups.
Results Of the 525 patients included (312 PsA and 213 SpA), most patients showed normal spinal radiographs: 87.5% of the patients with PsA and 92.0% of the patients with SpA. Patients with SpA with spinal damage show higher mSASSS than the patients with PsA (p<0.05). In patients with PsA, cervical spine is more often affected; 24/33 patients (72.7%) compared with lumbar spine 11/33 (33.3%). While in patients with SpA, syndesmophyte location was more evenly distributed; cervical 9/14 (64.3%) and lumbar 10/14 (71.4%).
Conclusion Minimal radiographic spinal damage was observed in Belgian patients with PsA or SpA. Patients with SpA tend to have higher mSASSS values and more syndesmophytes compared with PsA. Syndesmophytes were more often located in the cervical spine of patients with PsA, while the location was equally distributed in axSpA.
- Psoriatic Arthritis
- Spondyloarthritis
- Arthritis
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Psoriatic arthritis (PsA) and spondyloarthritis (SpA) share a number of clinical features; nevertheless there is an ongoing discussion about whether they belong to the same entity or are different phenotypes of the same disease.
WHAT THIS STUDY ADDS
In both patients with PsA as well as SpA, the incidence rate of radiographic spinal damage was low, nevertheless severe spinal damage, mainly syndesmophytes more damage was observed in patients with SpA.
Site distribution of syndesmophytes was equal in axial SpA while patients with PsA show more cervical syndesmophytes.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
These results shed light on the continuing discussion on the alleged difference in axial damage between patients diagnosed with PsA or SpA.
Introduction
Psoriatic arthritis (PsA) and spondyloarthritis (SpA) share similar genetic backgrounds (eg, MHC class I association), pathomechanism (eg, mechanoinflammation) and clinical presentation (eg, enthesitis).1 Both PsA and SpA can manifest in the spine. No clear consensus exists on defining axial involvement in PsA and therefore its prevalence varies greatly depending on which criteria are applied.2 While axial SpA (axSpA) classification criteria are clear and homogeneously applied, classification of axial PsA is multi-interpretable by lack of specific criteria. Axial PsA has been described as patients with PsA with inflammatory back pain (IBP). About half of all patients with PsA present with IBP at diagnosis or develop IBP, yet few show axial radiographic progression.3–6 Axial involvement in PsA has also been described as patients with unilateral or bilateral sacroiliitis using modified New York criteria (mNY). Often these studies are not focused on spine involvement and potentially do not cover the full spectrum of axial PsA.7–10 Equivalents of axial involvement might be modified Stoke Ankylosing Spondylitis Spine Score (mSASSS) ≥2, the presence of (any) syndesmophytes or various other definitions. Previous radiographic studies addressing axial involvement in PsA revealed pathological changes that are somewhat different from SpA such as parasyndesmophytes, asymmetrical sacroiliitis and predominant involvement of cervical spine.3 Also, facet joints seem to be less frequently involved in PsA.11
Considering that the differences, and similarities, between axial damage in patients with PsA and SpA require a better understanding, we examined radiographic axial damage of the sacroiliac joints (SIJs) and spine in patients with PsA and SpA from prospective multicentre cohort studies in private and academic rheumatology practices in Belgium.
Methods
Study design and data collection
Data on patients with PsA originate from the Belgian Epidemiological Psoriatic Arthritis Study (BEPAS) cohort. This national multicentre prospective non-interventional epidemiological trial included patients with clinical PsA diagnosis and fulfilling the Classification Criteria for Psoriatic Arthritis enrolled from 17 academic, non-academic and private practice centres across Belgium.12 In 312 patients, clinical information and spinal radiographs were available at inclusion and in 307 patients, pelvic radiographs were included.
Patients with SpA originate from the ongoing observational Ghent and BelGian Inflammatory Arthritis and spoNdylitis cohorTs ((Be-)GIANT).13 14 An imaging data subset was used, containing 213 patients with a clinical SpA diagnosis fulfilling the Assessment of SpondyloArthritis international Society (ASAS) classification criteria for axial (n=176, 82.6%) or peripheral (n=37, 17.4%) SpA, and without skin psoriasis. All 213 patients with SpA had available spinal radiographs and in 2/213 patients SIJ radiographs were missing.
Radiographic imaging assessment
Pelvic radiographs were scored according to the mNY criteria.15 Briefly, with this method SIJs are assessed on anteroposterior view plain radiographs. Radiographic changes of each SIJs are graded on a 0–4 scale. The mNY criteria are fulfilled in case of a bilateral grade 2 or unilateral grade 3 or 4 score (mNY+).
The spinal radiographs were assessed using mSASSS, assessing cervical and lumbar spinal segments for erosions, sclerosis, squaring or (bridging) syndesmophytes. The total score per patient ranges from 0 to 72.16 Lesions were only scored when they met the description of syndesmophytes. Ambiguous lesions like syndesmophytes due to Diffuse Idiopathic Skeletal Hyperostosis were not scored.17 18
Two central readers (AI, MdH) performed two training sets and one calibration round, conducted separately for SIJs and spine resulting in substantial agreement (kappa >0.70). After calibration, the centralised imaging assessment used in the current study started. Readers were blinded for origin of cohort, clinical data and other obtained images (radiographs of the hands/feet). In 1% of the reads, disagreement on the presence of syndesmophytes occurred. These cases were discussed and reader consensus was reached. All data presented are based on concordant reader scores.
Statistical analysis
Demographic, clinical and radiographic data were analysed using descriptive statistics. Continuous data were presented as mean±SD (normally distributed) or median, minimum, maximum and IQR (not normally distributed). Shapiro-Wilk test was used to determine normality. As radiographic data are usually not normally distributed but show a very skewed distribution, it was described in both mean±SD as well as median, minimum, maximum and IQR, adhering to recommended literature.19 Continuous variables were analysed by Student’s t-test or Mann-Whitney U test where appropriate. Statistical analysis was performed using STATA V.17 statistical software.
Results
In total, 525 patients were included in this study; 312 patients with PsA and 213 patients with SpA. Sex is equally distributed but patients with PsA are older, have less frequently a positive Human Leucocyte Antigen B27 (HLA-B27) (136 lacked HLA-typing), less often show IBP, good response to non-steroidal anti-inflammatory drugs or elevated erythrocyte sedimentation rate/C reactive protein compared with patients with SpA. Back pain was reported in 207 patients with PsA (table 1).
Demographic and clinical data of patients with PsA and SpA in private and academic Belgian practices
Thirty-three patients with PsA showed spinal damage (≥2 mSASSS) while 273 patients with PsA did not have any radiographic abnormalities at all (mSASSS=0). In 17 patients with SpA, spinal damage (≥2 mSASSS) was reported, all but one are patients with axSpA. Patients with SpA with spinal damage show a higher mSASSS, therefore indicating more severe spinal damage than patients with PsA (p<0.05) (table 2). Due to a few mSASSS outliers, average mSASSS was rather high compared with the median, especially in SpA with mean mSASSS of 10.3±14.91 and a median of 5 (IQR 2–13).
Reader consensus scores of radiographic spinal damage in patients with PsA and SpA
Syndesmophytes are seen in 10.6% (PsA) and 6.6% (SpA). Similar to mSASSS, patients with SpA had more syndesmophytes (mean: 4.9±5.78) compared with patients with PsA (mean 2.0±1.45); p<0.05. All patients with PsA with mSASSS ≥2 also had ≥1 syndesmophyte while three patients with SpA with mSASSS ≥2 has no syndesmophytes (table 2). In figure 1, examples of patients with PsA and SpA with syndesmophytes are shown.
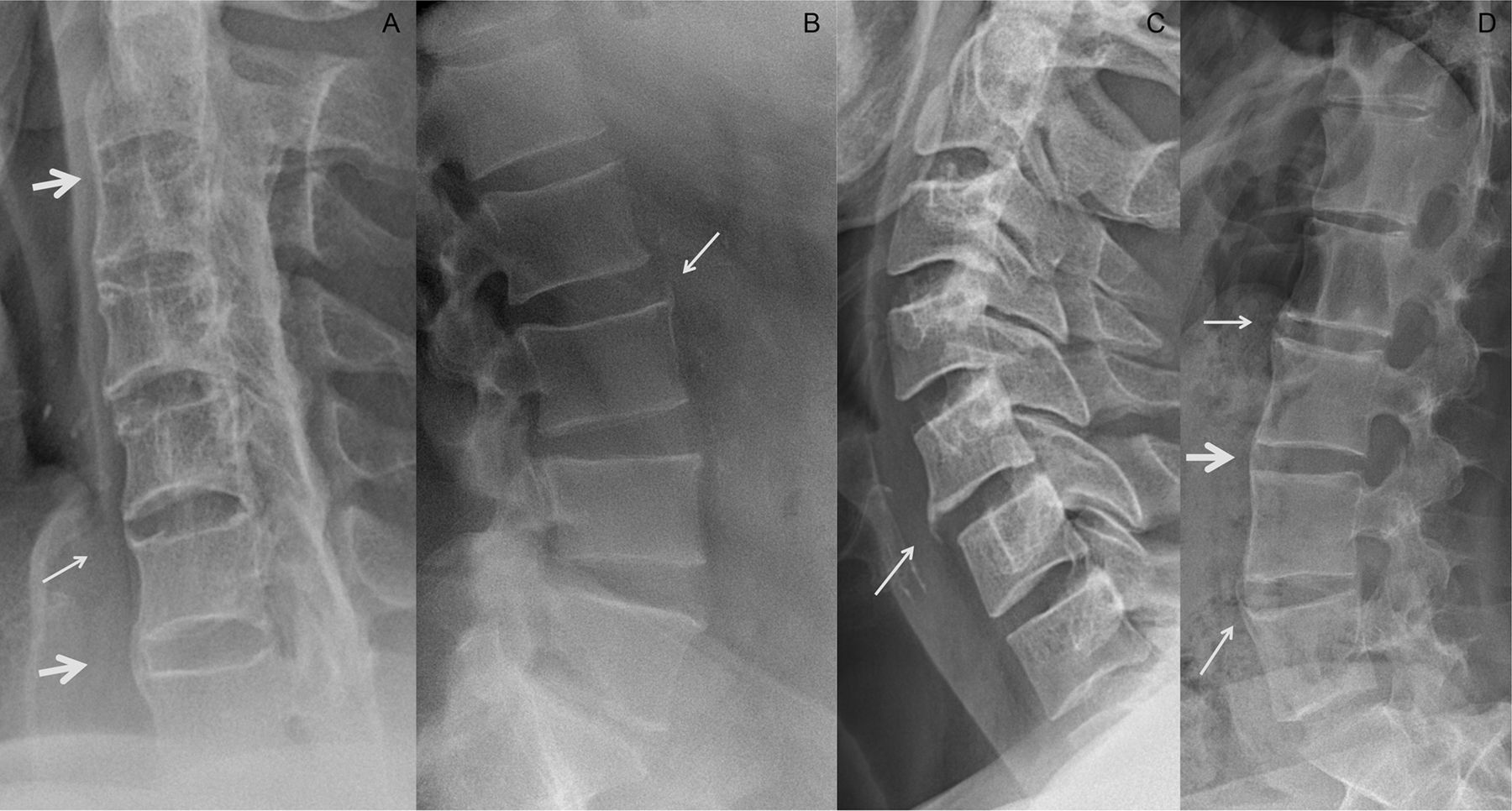
(A) Patient with psoriatic arthritis from the BEPAS cohort with cervical bridging (thick arrow) and non-bridging (thin arrow) syndesmophytes. (B) Patient with psoriatic arthritis from the BEPAS cohort with syndesmophytes (thin arrow) on upper anterior corner L3. (C) Patient diagnosed as peripheral spondyloarthritis from the (Be-)GIANT cohort with syndesmophytes (thin arrow) in C3, T12 and L1. (D) Patient with axial spondyloarthritis showing a syndesmophyte (thin arrow) on C5. (E) Patient with axial spondyloarthritis from the (Be-)GIANT cohort with several bridging (thick arrow) and non-bridging (thin arrow) syndesmophytes. (Be-)GIANT, BelGian Inflammatory Arthritis and spoNdylitis cohorTs; BEPAS, Belgian Epidemiological Psoriatic Arthritis Study.
Patients with PsA more often showed syndesmophytes in the cervical spine (72.7%) compared with lumbar syndesmophytes (33.3%). Syndesmophyte location was more evenly distributed in patients with SpA; cervical 64.3% and lumbar 71.4%. Percentages exceed 100%, as there were patients with syndesmophytes in both spinal segments.
Eight patients with PsA fulfilling the mNY criteria; six patients had mSASSS ≥2. In three patients, erosions were reported and all six patients showed syndesmophytes. Three patients had syndesmophytes in cervical spine and another three patients had lumbar syndesmophytes, with a cervical segment average of 3.7 syndesmophytes and a lumbar segment average of 2 syndesmophytes (figure 2).

{kind=link}
{kind=link}
Flowchart study population with spinal damage in patients (pt) with radiographic sacroiliitis according to mNY criteria. #Discordant cases are the patients in whom there was disagreement between readers on fulfilment of modified New York criteria; only one reader assessed modified New York as positive. *Consensus score means both readers agreed on fulfilment of modified New York criteria. (Be-)GIANT, Ghent and BelGian Inflammatory Arthritis and spoNdylitis cohorTs; BEPAS, Belgian Epidemiological Psoriatic Arthritis Study; mNY, modified New York; mSASSS, modified Stoke Ankylosing Spondylitis Spine Score; PsA, psoriatic arthritis; SpA, spondyloarthritis.
There were 58 patients with PsA with IBP and 207 with chronic back pain. When stratifying patients with PsA for the presence of axial involvement (IBP and chronic back pain) the trends are the same: ~11% of the patients with an mSASSS ≥2 driven by syndesmophytes, and more syndesmophytes in the cervical compared with lumbar segment (data not shown).
Similar to the spinal results, data on pelvic assessment in patients with SpA was also driven by the axSpA subgroup. From the 35 patients with SpA with dissent mNY scores, 32 patients were axSpA. Of the 20 patients with mNY+ SpA, six patients had mSASSS ≥2. There was one patient with erosions, two with squaring and three with sclerosis, all mutually exclusive. All mNY+ patients with mSASSS ≥2 had lumbar syndesmophytes and two patients also had cervical syndesmophytes with averages of 6.3 and 6 syndesmophytes, respectively.
Sensitivity analysis BEPAS cohort
In total, 461 patients were included in the entire BEPAS cohort. The mean age was 52.8±12.3 years and 43.0% were women; the average disease duration was 8.5±9.3 years and approximately 34% of the patients reported inflammatory axial pain. In one-third of the patients, radiographs were missing. Online supplemental table 1 shows the characteristics of these 149 patients. In general, patients with PsA that were excluded due to missing imaging do not differ from patients with PsA included in the current study. Only IBP is statistically significant more often seen in patients with PsA with radiographic imaging available. While patients with PsA without imaging are almost twice as often present with peripheral arthritis at baseline visit.
Supplemental material
Discussion
This study found minimal radiographic axial damage in Belgian patients with PsA and SpA. The reported spinal damage was mainly driven by syndesmophytes but not only the extent of severe lesions like syndesmophytes (spine) or ankylosis (SIJ) but any damage was uncommonly seen. Though the proportion of patients with spinal damage (strongly led by syndesmophytes) was not significantly different between the two patient groups, the degree of damage was higher in SpA compared with patients with PsA, suggesting the latter to be a disease in which pattern recognition should be considered less focused on axial disease. Not all patients with PsA had radiographs taken which is common in clinical practice but in addition also allows for the possibility that radiographic damage was either underestimated or overestimated. This bias would apply to both cohorts making the comparisons between patients with PsA and SpA groups valid.
An interesting difference is the distribution of syndesmophytes over cervical and lumbar segments. A clear distinction was seen between patients with axSpA and PsA. The syndesmophyte ratio in the cervical/lumbar spine was over 2:1 in patients with PsA, while in patients with axSpA, this was 1:1, which is in agreement with the literature.11 20 21
Especially in established SpA, facet or zygapophyseal joints are frequently affected.22 23 Therefore, an argument could be made that spinal damage assessment should include these joints. This is a limitation of all currently available validated radiographic spinal scoring methods and subsequently spinal damage could have been underestimated in this study. Limitations of this study are the absence of HLA-typing in over half of the patients from the BEPAS cohort and the lack of MRI data. MRI would be preferred over radiographs as inflammation can be detected and there is no radiation exposure. Unfortunately at the time of developing the BEPAS protocol (before 2012), HLA-B27 was not a standardised feature of interest in these types of studies and MRI was not valued as useful in daily clinical practice for patients with PsA. Currently, two global organisations, ASAS and the Group for Research and Assessment of Psoriasis and Psoriatic Arthritis, announced a joint project studying axial involvement in PsA looking at various data, including MRI.24 This future research provides the opportunity to focus on the examination of the extent and association of inflammatory and structural lesions, like fat deposition, of the axial skeleton in PsA.
The strengths of this study are the systematic reading assessments of the imaging data with good reader agreement, which was achieved after training for spinal and pelvic radiographs separately. The reported data of this study were based on reader consensus score, which makes the data more robust and the results less affected to reader assessment fluctuations.
In this multicentre cohort study of Belgian patients with PsA or SpA, we observed a low incidence of radiographic spinal damage, regardless, syndesmophyte extent exceeded in patients with SpA. Syndesmophytes were frequently located in the cervical spine in patients with PsA, while cervical and lumbar syndesmophytes were equally distributed in patients with axSpA.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by local ethical committees from the participating centres. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
Authors like to noteworthy mention Hermine Leroi from MSD Belgium.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
MdH and AI are joint first authors.
KdV and FVdB are joint senior authors.
Contributors AI assessed the images and contributed to writing the manuscript. MdH assessed the images, conducted data management and the analyses, and wrote the manuscript. KdV, RL, FVdB and MdH interpreted the data. All authors read and approved the final manuscript. KdV and FVdB are joint last authors.
Funding BEPAS has been funded by MSD Belgium. Be-GIANT has been funded by unrestricted grants from AbbVie.
Competing interests AI, A-SDC and AN have no conflict of interests. MdH has received consultancy fees and/or invitation for congresses from UCB. SS has received consultancy fees and/or invitation for congresses from Celgene, Novartis, Abbvie, Phizer and MSD. DE has received consultancy and speaker fees from Abbvie, Amgen, Eli Lilly, Galapagos, Gilead, Janssen, Merck, Novartis, Pfizer and UCB. RL has received consultancy and speaker fees, and research grants from Abbvie, Amgen (Celgene), Eli-Lilly, Galapagos, Janssen, Kabi-Fresenius, MSD, Novartis, Pfizer, Sandoz, Biosplice (Samumed) and UCB. KdV has received consultancy and speaker fees, and research grants from Amgen, Affibody, Abbvie, Eli-Lilly, KOOR UZleuven, Pfizer and UCB. FVdB has received speaker and/or consultancy fees from Abbvie, Celgene, Eli Lilly, Galapagos, Gilead, Janssen, Merck, Novartis, Pfizer and UCB.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.