Article Text

Abstract
Objective To study the effect of methotrexate (MTX) therapy on new-onset uveitis in patients with biological-naïve juvenile idiopathic arthritis (JIA).
Methods In this matched case–control study, we compared MTX exposure between cases with JIA-associated chronic uveitis (JIA-U) and patients with JIA and without JIA-U at the time of matching (controls). Data were collected from electronic health records of the University Medical Centre Utrecht, the Netherlands. Cases with JIA-U were matched 1:1 to JIA control patients based on JIA diagnosis date, age at JIA diagnosis, JIA subtype, antinuclear antibodies status and disease duration. The effect of MTX on JIA-U onset was analysed using a multivariable time-varying Cox regression analysis.
Results Ninety-two patients with JIA were included and characteristics were similar between cases with JIA-U (n=46) and controls (n=46). Both ever-use of MTX and exposure years were lower in cases with JIA-U than in controls. Cases with JIA-U significantly more often discontinued MTX treatment (p=0.03) and out of those who did, 50% afterwards developed uveitis within 1 year. On adjusted analysis, MTX was associated with a significantly reduced new-onset uveitis rate (HR: 0.35; 95% CI: 0.17 to 0.75). No different effect was observed between a low (<10 mg/m2/week) and standard MTX dose (≥10 mg/m2/week).
Conclusion This study demonstrates an independent protective effect of MTX on new-onset uveitis in patients with biological-naïve JIA. Clinicians might consider early initiation of MTX in patients at high uveitis risk. We advocate more frequent ophthalmologic screening in the first 6–12 months after MTX discontinuation.
- Arthritis, Juvenile
- Methotrexate
- Epidemiology
- Autoimmune Diseases
Data availability statement
Data are available upon reasonable request. All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
The current literature reports contradicting evidence about a possible preventive effect of methotrexate (MTX) on juvenile idiopathic arthritis (JIA)-associated uveitis (JIA-U) onset.
No study has yet demonstrated an independent preventive effect of MTX therapy on JIA-U in patients with biological-naïve JIA.
WHAT THIS STUDY ADDS
In this study, MTX was associated with a reduced JIA-U onset rate in patients with biological naïve JIA on adjusted and time-varying analysis.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Clinicians might consider early treatment with MTX in patients at high risk of developing JIA-U.
Clinicians should always consider more frequent ophthalmologic screening after MTX discontinuation.
Introduction
Juvenile idiopathic arthritis (JIA) is the most common chronic inflammatory rheumatic condition of childhood with a global prevalence ranging from 3.8 to 400 cases per 100 000 population.1 Uveitis is a common extra-articular manifestation of JIA, with a predicted risk of up to 40% in antinuclear antibodies (ANA) positive patients with JIA with early onset of oligoarthritis.2 The chronic form of uveitis is characterised by asymptomatic inflammation of the uveal layer of the eye. Therefore, tailored ophthalmologic screening of patients with JIA is essential to early detect chronic uveitis and commence treatment before the development of vision-disabling complications such as cataracts, glaucoma, band keratopathy and macular oedema.3 4
Although the conventional synthetic disease-modifying antirheumatic drug (DMARD) methotrexate (MTX) is commonly used in the treatment of JIA-associated chronic uveitis (JIA-U),5 little is known about its possible preventive effect on developing new-onset JIA-U. Two observational studies reported significantly less uveitis development in patients with JIA who had ever received MTX compared with patients who had not received MTX.6 7 In contrast, no preventive effect of MTX on the number of uveitis events was observed in an additional exploratory analysis of a randomised controlled trial (RCT) in patients with oligoarticular JIA treated with intra-articular steroids.8
The primary aim of this study was to investigate the effect of MTX therapy on the development of new-onset chronic uveitis in children with JIA not treated with biological DMARDs. Secondary aims were to study the influence of different MTX doses and discontinuation of MTX therapy.
Methods
Study design and patients
Whereas a cohort study is concerned with frequency of disease in exposed and non-exposed individuals, a case–control study is concerned with the frequency and amount of exposure in subjects with a specific disease (cases) and people without the disease (controls).9 In this matched case–control study, clinical, demographic, laboratory and drug therapy data were collected from electronic health records of patients with JIA-U from a previously reported dataset10 11 and patients with JIA who did not develop uveitis at the time of matching from a distinct cohort.12 All patients were treated at the University Medical Centre Utrecht (UMCU), the Netherlands, a tertiary referral centre. Patients with JIA-U were treated at the UMCU department of ophthalmology and a diagnosis of JIA-U was made by an ophthalmologist specialised in paediatric uveitis. Control patients with JIA were treated at the UMCU department of paediatric immunology and rheumatology, located within the Wilhelmina Children’s Hospital. A diagnosis of JIA was made by a paediatric rheumatologist according to International League of Associations for Rheumatology criteria.13 Exclusion criteria for this study were a JIA diagnosis before the year 2000, enthesitis-related arthritis (ERA), systemic arthritis, rheumatoid factor (RF) positive polyarthritis, a diagnosis of uveitis prior to or simultaneously with JIA onset, no records of regular ophthalmologic screening and the use of biological DMARD therapy. Only patients with a JIA diagnosis from 2000 onwards were included since MTX was not commonly used in the UMCU prior to this year. Patients with ERA were excluded since these commonly present with acute instead of chronic uveitis.3 4 Systemic arthritis and RF positive patients with polyarthritis were excluded due to their minimal risk of developing JIA-U.2 14 Data were arrested on 19 November 2021.
Determinants and outcome
For each patient, the following data were collected: gender, date of JIA diagnosis, JIA subtype, JIA disease duration, the number of joints with active inflammation at JIA diagnosis, ANA status, human leucocyte antigen (HLA)-B27 status, erythrocyte sedimentation rate (ESR) at JIA diagnosis, use of non-steroidal anti-inflammatory drugs, intra-articular corticosteroids, systemic corticosteroids, MTX and other conventional synthetic DMARDs, MTX dose (mg/m2/week), MTX start and stop dates and date of uveitis diagnosis. For this study, disease duration was defined as the time from JIA diagnosis to uveitis diagnosis for cases with JIA-U, and time from JIA diagnosis to last visit or start of biological therapy for controls with JIA. Later data were censored. For the number of active joints, a maximum time difference of 6 months from JIA diagnosis was allowed. For ANA positivity, only one positive test at a titre of ≥1:40 was required since in multiple occasions this was the only titration that was recorded. For ESR, a maximum time difference of 3 months from JIA diagnosis was allowed. Patients were only considered to have used MTX if they had received at least 4 weeks of consecutive MTX therapy. If body surface area for calculation of MTX doses was not available, average values from the Dutch national growth curves were used.15 We classified MTX doses <10 mg/m2/week as low-dose MTX and doses ≥10 mg/m2/week as standard dose MTX.16
Matching
Cases with JIA-U were matched 1:1 to controls with JIA without replacement based on date of JIA diagnosis (to counteract the influence of treatment strategies changing over time) and the following known risk factors for JIA-U: age at JIA diagnosis, JIA subtype, ANA status and JIA disease duration.3 4 In order to identify similar patients based on all of the before mentioned variables, matching was based on the nearest Mahalanobis distance17 and no calliper (ie, maximal acceptable distance) was used. By doing so, cases with JIA-U were matched to control patients with JIA from similar time periods with similar clinical characteristics and disease duration, who had not developed JIA-U at the time of matching. In case, a case with JIA-U was similar to a control patient with JIA with longer disease duration, data from the control patient after a disease duration equal to that of the case with JIA-U were disregarded. In this way, a patient with JIA who developed JIA-U could act as a control patient as long as he or she developed JIA-U after a disease duration equal to that of a matched case with JIA-U. We only included unique patients, which means that a patient could not act as both a case and a control in our study.
Statistical analysis
Characteristics of cases with JIA-U and controls with JIA were presented as frequency and valid percentage for categorical variables and median and IQR for numerical variables. Variables were compared between the two groups using the Mann-Whitney U test, χ2 or Fisher’s exact test. A p value of <0.05 was considered statistically significant for all analyses. The adjusted effect of (different doses of) MTX therapy on new-onset uveitis was examined using a multivariable Cox regression analysis for which MTX therapy was entered as a time-varying variable. This type of analysis is commonly used to prevent immortal time bias which occurs if exposure time is misclassified in groups with non-constant exposure over time.18 In order to remove potential bias due to the matched case–control study design,19 the analysis was adjusted for the matching factors age at JIA diagnosis, JIA subtype and ANA status. Linearity of the numerical age at JIA diagnosis variable was checked by plotting it against the Martingale residuals. Associations were reported as adjusted HRs with 95% CIs. Analyses were performed with IBM SPSS Statistics V.26.0.0.1 and the survival and survminer packages for R V.4.0.3.20 We adhered to the Strengthening The Reporting of Observational Studies in Epidemiology checklist for case–control studies (online supplemental file 1).21
Supplemental material
Results
Patient characteristics
Out of 160 cases with JIA-U, 46 were eligible for matched analysis. Most cases were excluded because of a JIA diagnosis before the year 2000 or (a history of) uveitis at JIA diagnosis (figure 1). The majority of included cases with JIA-U and matched control patients with JIA were girls with ANA positive oligoarthritis, characteristics did not differ significantly between cases and controls (table 1). In addition, JIA diagnosis dates of cases (median 2 January 2010; range 1 February 2000 to 14 November 2018) and controls (median 12 April 2011; range 21 February 2002 to 20 November 2018) were from a roughly similar time period.
Characteristics of matched cases with JIA-U and control patients with JIA

Flowchart of included patients. Patients were matched on date of JIA diagnosis, age at JIA diagnosis, JIA subtype, ANA status and JIA disease duration. ANA, antinuclear antibodies; JIA, juvenile idiopathic arthritis; JIA-U, juvenile idiopathic arthritis-associated uveitis; UMCU, University Medical Centre Utrecht.
MTX therapy and uveitis onset
Drug history was not significantly different between cases with JIA-U and control patients with JIA, although ever use of MTX was lower in the cases (50.0% vs 65.2%, respectively) (table 2). Furthermore the median number of exposure years was also lower in the cases than in the controls (0.1 years vs 0.5 years, respectively). Out of all cases, only 20% (n=9) developed JIA-U while on MTX therapy. Of these nine patients, seven (78%) had used MTX for less than 6 months. Also, two (22%) received low-dose MTX therapy. Furthermore, cases with JIA-U had significantly more often discontinued MTX therapy than control patients with JIA (69.6% vs 40.0%; p=0.03). Fifty per cent of those patients with JIA-U who discontinued MTX therapy and did not restart (n=14) developed uveitis within 1 year after discontinuation (figure 2).
Drug history at censor date of matched cases with JIA-U and control patients with JIA
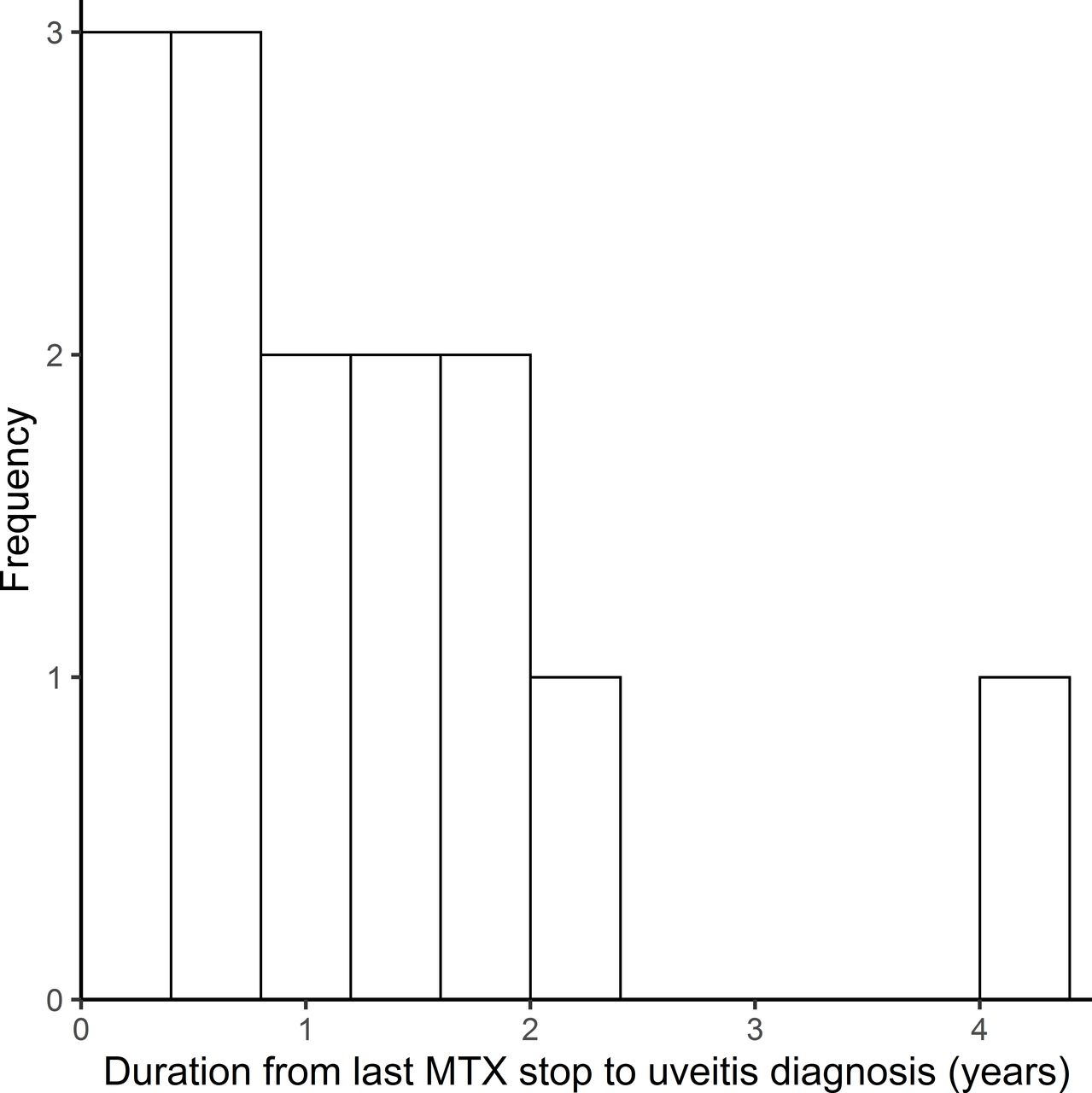
Distribution of time from last MTX stop to uveitis diagnosis. The figure includes patients with juvenile idiopathic arthritis-associated uveitis who discontinued MTX and did not restart before uveitis development (n=14). MTX, methotrexate.
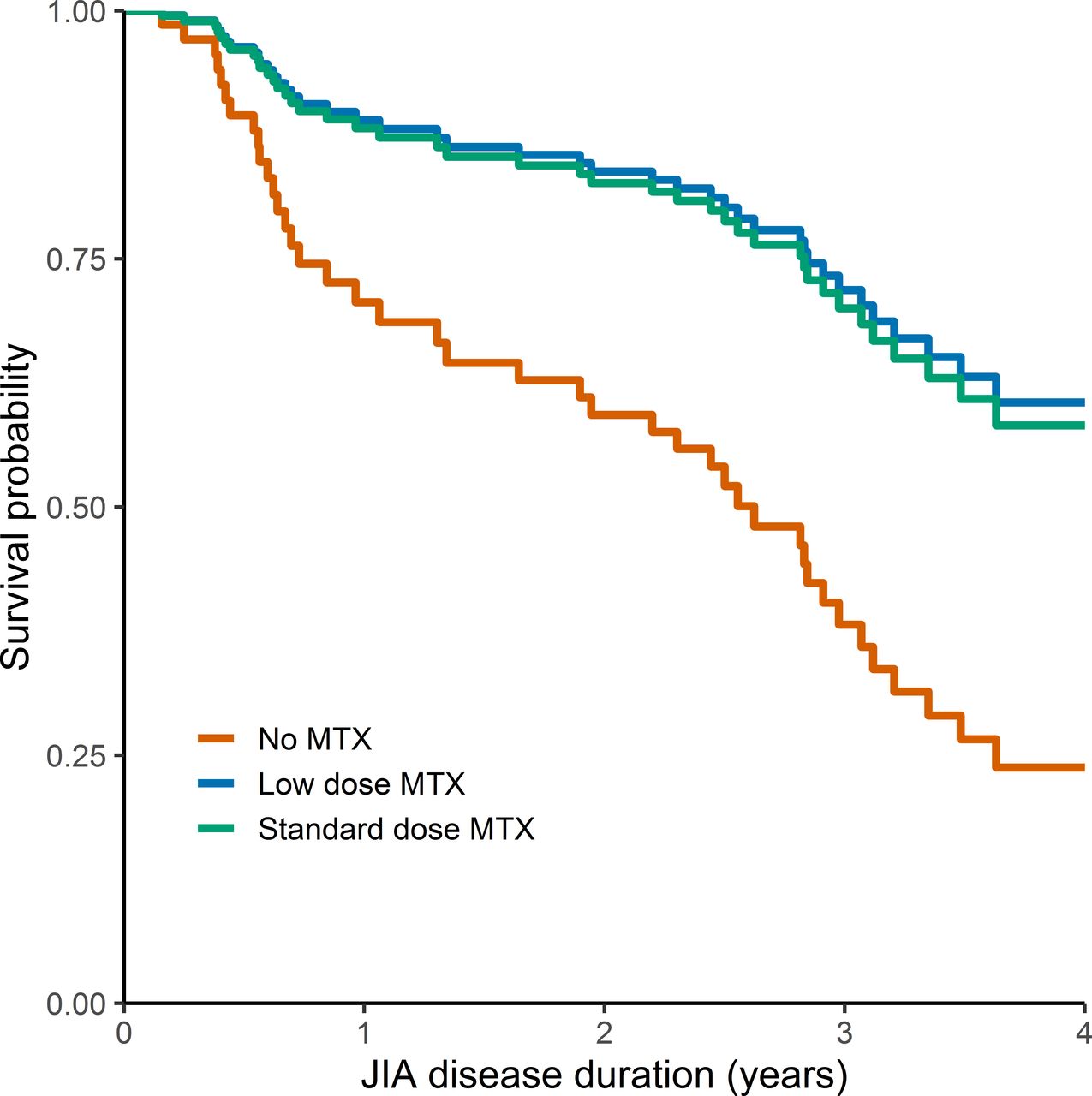
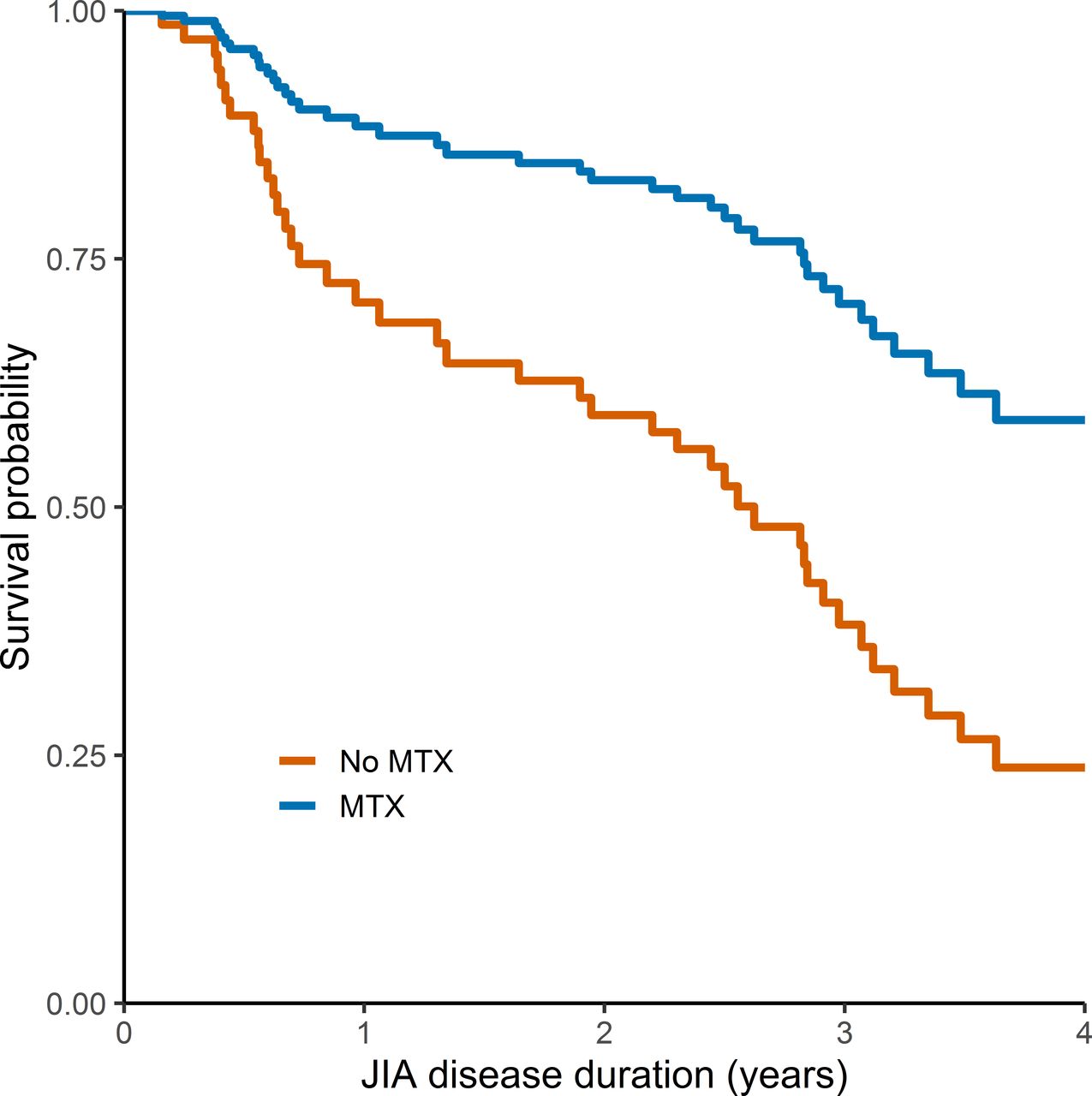
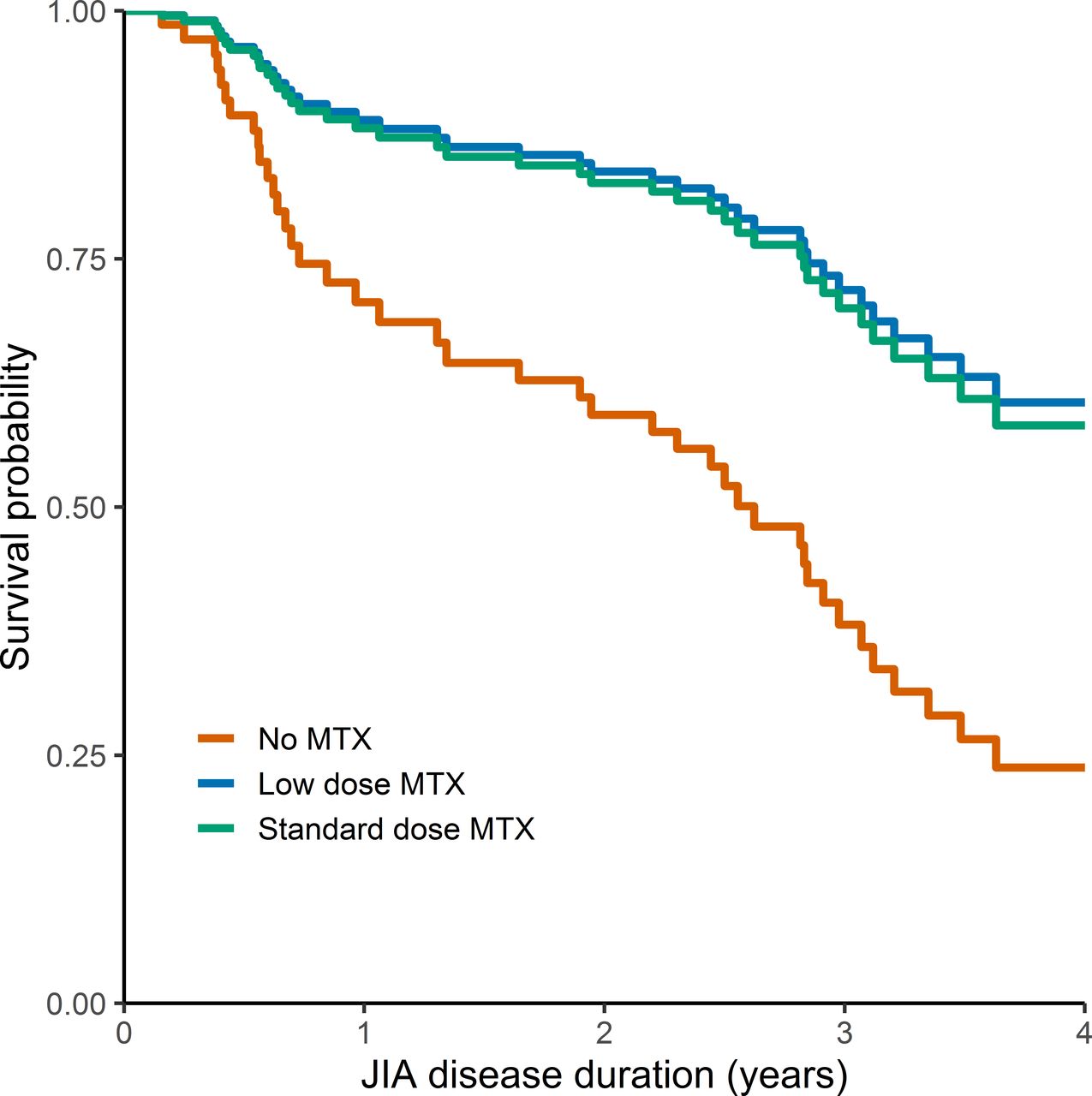
On multivariable analysis, MTX therapy was associated with a significantly reduced new-onset uveitis rate throughout the study (figure 3). The use of MTX was associated with an almost three times lower adjusted hazard for JIA-U development compared with no MTX use (HR: 0.35, 95% CI: 0.17 to 0.75) (table 3). The risk of JIA-U was not significantly different for low dose MTX therapy (<10 mg/m2/week) compared with standard dose therapy (table 4; figure 4), indicating that MTX was protective against JIA-U already at a low dose.
Multivariable Cox regression analysis for new-onset chronic uveitis
Multivariable Cox regression analysis for new-onset chronic uveitis as a function of different MTX therapy doses

Diagram of average survival curves for new-onset uveitis in current case–control study. The separate curves for subpopulations with and without MTX use are calculated based on the adjusted time-varying Cox model, therefore they follow a similar pattern and do not represent generalisable absolute numbers of patients at risk over time. JIA, juvenile idiopathic arthritis; MTX, methotrexate.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Diagram of average survival curves for new-onset uveitis in current case–control study. The separate curves for subpopulations with and without low (<10 mg/m2/week) or standard dose (≥10 mg/m2/week) MTX use are calculated based on the adjusted time-varying Cox model, therefore they follow a similar pattern and do not represent generalisable absolute numbers of patients at risk over time. JIA, juvenile idiopathic arthritis; MTX, methotrexate.
Discussion
This study reports a significant protective effect of MTX therapy on new-onset uveitis in patients with JIA not treated with biologicals. This effect was not different for low versus standard dose MTX. Fifty per cent of patients with JIA-U that discontinued MTX therapy and did not restart developed uveitis within 1 year after discontinuation.
The results of this study are supported by current guidelines that consider MTX as effective systemic treatment for JIA-U.5 22–24 The current findings are also in line with two previous observational studies in which patients with JIA who had ever received MTX had developed less JIA-U than patients who had not received MTX.6 7 These studies, however, did not perform adjusted analyses and also did not analyse the effect of MTX as a time-varying exposure, introducing the risk of significant immortal time bias. In contrast, an RCT reported more new-onset uveitis events in patients with oligoarticular JIA treated with intraarticular corticosteroids plus MTX (n=6, 8%) than in patients with oligoarticular JIA treated with intraarticular corticosteroids only (n=3, 4%) in an additional exploratory analysis. This result was, however, not statistically significant and follow-up time was only 12 months.
Considering that untreated JIA-U can potentially lead to significant visual impairment, physicians might consider early initiation of MTX therapy especially in patients at high risk of developing JIA-U, commonly girls with ANA positive oligoarthritis onset at a young age.25 In fact, in most JIA treatment guidelines, these are exactly the patients that now often receive intra-articular corticosteroid injections instead of MTX.26 This study indicated that MTX therapy is protective against JIA-U in both low and standard doses. If future studies confirm this finding, low-dose MTX therapy (<10 mg/m2/week) could be offered to patients with JIA with low arthritis disease activity but high risk of developing JIA-U. This might also have a beneficial effect on the risk of MTX side effects, which are common and include nausea, gastro-intestinal complaints, mouth ulcers and hepatotoxicity.24 27
Our study found that the risk of JIA-U in patients who discontinued MTX therapy was highest shortly after discontinuation. This is in line with a German national register study that highlighted MTX discontinuation on successful remission of arthritis as an apparent risk factor for JIA-U.28 For this reason, physicians should consider more frequent ophthalmologic screening after MTX discontinuation in patients at high risk of developing JIA-U, which is dependent on JIA subtype, ANA status, JIA disease duration and age (at JIA onset).25 This practice is also recommended in the British Society for Paediatric and Adolescent Rheumatology and Royal College of Ophthalmology screening guidelines for JIA-U.4 Here, we recommend to increase screening frequency in the first 6–12 months after MTX discontinuation and then revert to current screening guidelines. It has long been recommended to increase screening frequency for uveitis to every 2 months in the highest risk group of patients with patients with JIA.29 Furthermore, it could be considered especially early in the disease course not to stop MTX therapy in the group of patients with highest risk of JIA-U, but rather switch to a low dose of MTX. This is in line with our finding that patients who developed JIA-U within 1 year after MTX discontinuation had used MTX therapy for a shorter time than patients who developed JIA-U more than 1 year after MTX discontinuation. The above suggestions have been discussed within the Multinational Interdisciplinary Working Group for Uveitis in Childhood, which aims to improve current international uveitis screening guidelines for JIA based on the principle of evidence-based medicine, and has expressed its support for increasing screening frequency after MTX discontinuation.
Like MTX, the monoclonal antibody tumour necrosis factor (TNF) inhibitors adalimumab (ADA) and infliximab (IFX) are considered effective in the treatment of JIA-U. An RCT reported the effectiveness of ADA combined with MTX over MTX monotherapy30 and current guidelines recommend MTX combined with ADA or IFX in patients with severe JIA-U.5 22–24 Although there are to date no strong data from observational studies in support of a preventive effect of monoclonal antibody TNF inhibitors due to the problem of confounding by indication, paediatric rheumatologists commonly opt for ADA instead of etanercept as the biological DMARD therapy of choice in patients at high risk of JIA-U.31 Large-scale observational studies comparing the effects of MTX, IFX and ADA on the development of JIA-U report contradicting results.28 32–34 Still, TNF inhibitors are currently not considered an alternative to MTX as a first-line DMARD for treating JIA, but they are effective therapies after MTX failure or intolerance.
Our study has limitations. First, as with every case–control design, there is a certain risk of bias due to sampling of controls. However, this bias was minimised by selecting control patients from the same source population as the identified cases and who would have been selected as cases had they developed the outcome of interest.9 Cases with JIA-U and controls with JIA furthermore showed similar characteristics. Second, we only identified eligible cases with JIA-U with oligoarthritis or RF-polyarthritis. Consequently, we cannot state with certainty that our findings are applicable for patients with psoriatic and undifferentiated arthritis, who also run a notable risk of developing JIA-U.2 Third, we were unable to study the effect of MTX doses below 5 mg/m2/week on JIA-U onset rates due to very few data.
Future research should focus on studying the time-varying effect of JIA disease activity scores such as the cJADAS35 on the relationship between MTX use and new-onset JIA-U. Studies have reported higher disease activity in JIA to be associated with JIA-U, both temporarily and as a long-term predictor.34 36–38 There is a possibility that disease activity is an unmeasured confounder in the effect of MTX on new-onset JIA-U for the current study, since higher disease activity in general provides more rationale for treatment with MTX. Therefore, it could be that the independent protective effect of MTX on new-onset JIA-U is even stronger than reported here. A high disease activity could also explain why we still observed nine patients who developed JIA-U while on MTX treatment. Second, the observed protective effect of (different doses of) MTX on new-onset JIA-U should ideally be confirmed in an RCT in order to eliminate any risk of selection bias. Such a study could also provide a number of patients who need to be treated over a specific time-period to prevent one case of JIA-U.
In conclusion, we report a significantly reduced rate of new-onset chronic uveitis in patients with biological-naïve JIA treated with MTX therapy. Treating physicians might consider early initiation of MTX therapy in patients with JIA at high risk for uveitis and we advocate more frequent ophthalmologic screening especially in the first 6–12 months after MTX discontinuation.
Data availability statement
Data are available upon reasonable request. All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants but this study was classified by the institutional review board of the UMC Utrecht as exempt of the Medical Research Involving Human Subjects Act (22/604) and was carried out in compliance with the Helsinki Declaration. All included patients provided informed consent for the use of their data for scientific purposes, exempted this study. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
The authors thank Kirsten van der Velden, Marit Bijl and Annelies Suijs for facilitating the collection of informed consents. Part of this work was previously presented at the 2022 PReS congress in Prague, Czech Republic (abstract number P182).
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
JWvS and GA contributed equally.
Correction notice This article has been updated since it was first published online. Joeri W van Straalen and Görkem Akay contributed equally and this has been updated in the proof.
Contributors JWvS, GA, SdR, JFS, JdB, VKA and CVK conceptualised and designed the study. JWvS, NMW, JdB, CVK and VKA collected clinical data. GA and JWvS collected study data from electronic medical records. JWvS and GA analysed and verified the underlying study data. GA searched the literature and wrote the first draft. The manuscript was finalised by JWvS. NMW and JdB acquired funding. All authors interpreted the data, reviewed and revised the manuscript, and gave final approval for the manuscript to be submitted for publication. All authors agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. JWvS is responsible for the overall content as the guarantor.
Funding This study was financially supported by the Dutch Ophthalmology Foundation ‘UitZicht’ and ‘ODAS stichting’, and by longstanding research support from the Dutch Arthritis Foundation (ReumaNederland), grant number LLP10. Funding entities had no role in the conducting or presentation of this study.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.