Article Text

Abstract
Chondrocalcinosis (CC) is the one of the most common crystal pyrophosphate disease associated arthritis in the elderly. It has been shown to coexist with seronegative and seropositive rheumatoid arthritis (RA), yet mostly with seronegative RA. Among the localisation of CC, the deposition in the ligaments surrounding the odontoid process may remain asymptomatic for years or may lead to and acute severe symptomatology, which may mimic several clinical illnesses among which meningitis (fever, severe pain, acute phase reactants). This is called the ‘crowned dens syndrome (CDS)’, which has been reported to represent an important percentage of acute neck pain needing hospital admission in neurosurgery units. In this case, the rapid demonstration of ‘crowned dens’ through CT scan may allow to avoid lumbar puncture and cerebrospinal fluid examination. The coexistence of RA and CDS is very rare, and rarely reported in the literature, yet it may represent a clinical challenge. We describe here one case that while on therapy with methotrexate (MTX) and naproxen (NPX) had an acute neck pain, and peripheral arthritis flare, that responded well to colchicine given along with MTX and NPX.
- Rheumatoid Arthritis
- Chondrocalcinosis
- Crystal arthropathies
- Therapeutics
- Arthritis, Rheumatoid
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
In an old female patient with history of seronegative arthritis presenting with acute relapse in a disease mostly stable over time, the coexistent common crystal pyrophosphate disease (CPPD) should always be considered. In fact chondrocalcinosis can coexist with seronegative and seropositive rheumatoid arthritis (RA).
WHAT THIS STUDY ADDS
When an acute neck pain, with increased acute phase reactants, and fever, is present, a ‘crowned dens syndrome’ should always be ruled out in RA through a CT scan of the atlo-axial joints, which will show if the atlo-odontoid joints have synovitis, erosions or calcifications.
The demonstration of a crowned dens may avoid lumbar puncture and cerebrospinal fluid examination.
Instead of using corticosteroids, if the patient does not respond to non-steroidal anti-inflammatory drugs, colchicine may lead to control the disease symptoms.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
It raises the issue of the coexistent RA and CPPD which is more common than usually thought. It gives indications on how to behave in case of acute neck pain simulating other clinical illnesses among which meningitis. It allows to define a therapeutic approach in such critical cases.
Introduction
Chondrocalcinosis (CC), the calcium pyrophophate deposition disease (CPPD) disease, has been reported to have a radiographycally reported prevalence of 15% in subjects aged 65–74 years, with no gender prevalence,1 The association between RA (rheumatoid arthritis) and CC occurs more often than expected in clinical practice.2 It has been reported that in 32.3% of seronegative and 16.6% of seropositive RA, CC coexist, thus even higher than in the general population. The possibility that it may represent a comorbidity needs to be explored. Even though the identification of CPPD crystals by polarised microscopy is the strongest tool to diagnose CC, the crystal deposition observed through conventional radiography is considered the most rapid and convenient tool to diagnose CC, yet to diagnose CPPD clinical criteria are necessary among which acute attacks of arthritis, flares, swollen and erythematous joints.3 These characteristics allow to identify peripheral CPPD if radiography suggests the presence of calcified cartilages at specific sites (wrists, knee menisci, pubic symphisis, etc).4 5 Since the occurrence of acute episodes and flares may occur also in a poorly controlled RA, the final diagnosis of concomitant illnesses RA and CPPD may be delayed and often not made. A further confounding factor is represented by the presence of erosions. As reported by Krekeler et al, erosions are similarly present in CPPD and in RA, even though more often in seropositive RA.2 Even though the difference in the degree of the erosiveness is not well defined in the literature, nevertheless the item ‘erosiveness’ cannot be fully discriminative, though much more relevant in RA.6 However, the erosions at the craniocervical region (atloepistrophic joint) are quite distinctive; we showed they may occur already in early RA7 and have very rarely been described in CPPD. Therefore, one possibility to discriminate between an acute attack of RA or an acute arthritis episode CPPD-related, may be the demonstration of CC at the craniocervical region, in the presence of an acute flare of pain. In fact, up to 51% of CPPD may present periodontal calcified deposits.8 These calcifications may appear with the shape of a crown and in fact they were defined as ‘crowned dens’ by Bouvet et al.9 If the crowned dens presents with acute severe pain,10 sometimes mimicking a meningitis it has been defined as a ‘crowned dens syndrome (CDS)’.11
Case report
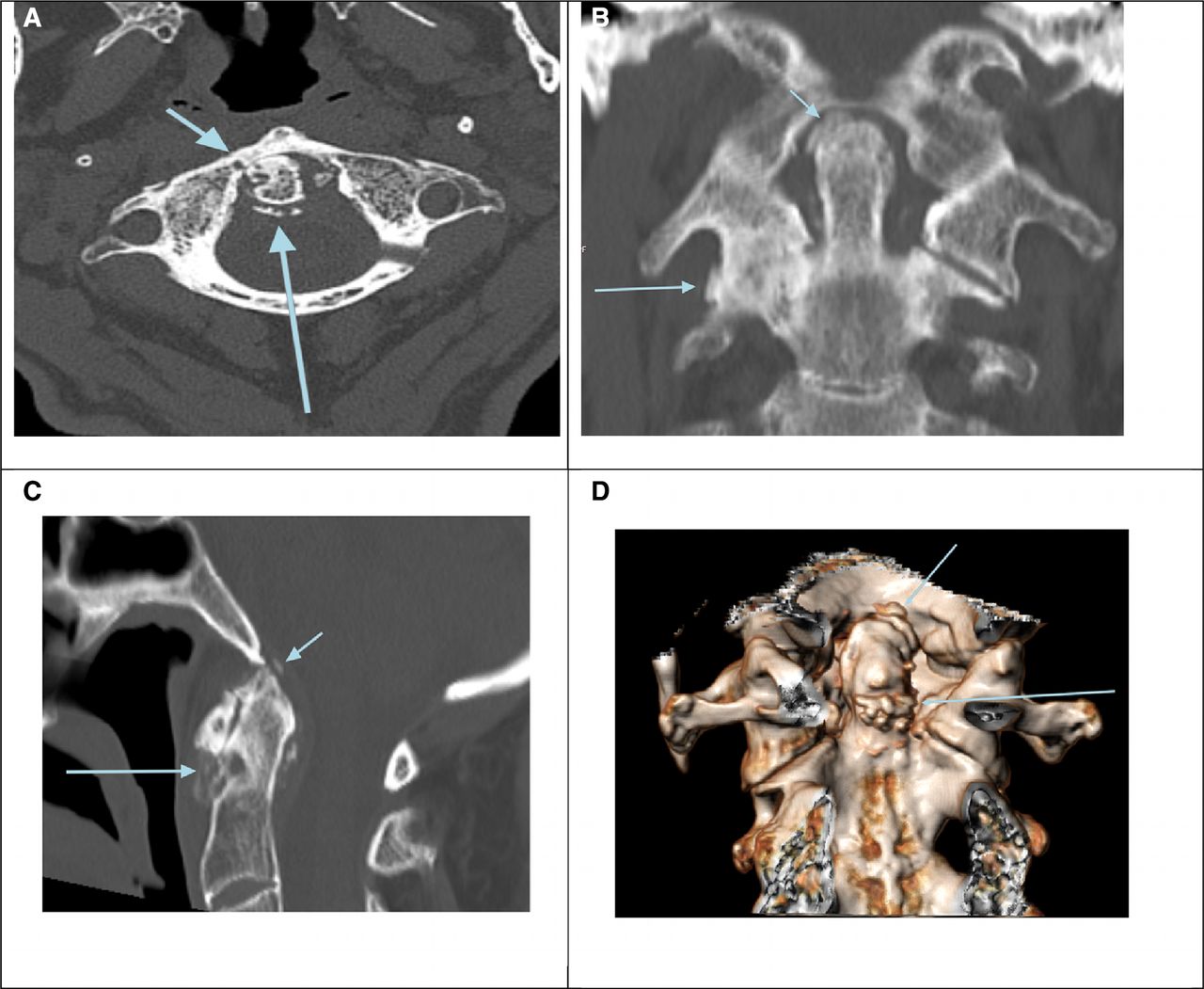
We present here the case of a 75-year-old woman with a diagnosis of RA made 5 years earlier (poliarticular arthritis of wrists, 2’ metacarpophalangeal, 3’−5’ metatarsophalangeal and knee joints), who came for acute pain relapse in wrists and cervical spine. Over the years, she already had intermittent cervical pain, always considered as a consequence of muscle contractures and cervical pain osteoarthritis, VAS (Visual Analogue Scale) pain was 9/10 at the cervical spine. Physical examination revealed swollen and painful wrists, tenderness but no swelling of the 2–3’ metacarpophalangeal joints. She had fever at 38.2 ’C, she had severe cervical pain, rotation was almost impossible and flexion was 30°C. Two years earlier, she had sudden knee swelling, resolved with intraarticular injections of triamcinolone exacetonide 40 mg per joint. She was on Methotrexate (MTX) 12.5 mg/week (plus folic acid) and naproxen (NPX) 750 mg/daily pro re nata. Lab tests showed C reactive protein (CRP) 22 mg/L, uric acid 6.1 mg/dL, normal haematology, no rheumatoid factor, no ACPA, no ANA. The hypothesis that an acute cause of arthritis could be involved was raised because of the few infrequent, sudden relapses. An immediate C1–C2 cervical spine CT scan revealed a deep erosion of the dens, erosions of the athlantoepistrophic joint, calcium-crystal deposition in the transverse atlas and in the alar and apical ligaments, surrounding the odontoid process (Figure 1). A knee radiograph confirmed calcium pyrophosphate deposition disease (CPPD). The final diagnosis was CDS-CPPD in RA. The preliminary, never validated, criteria for CDS were all fulfilled: (1) a history of acute neck pain and limited cervical activity, (2) laboratory tests showing elevated inflammatory markers such as erythrocyte sedimentation rate, CRP.12

{kind=link}
(A) Axial view—The dens presents multiple geodes (short light blue arrow) and erosions, calcified transverse ligament (long light blue arrow) and calcified alar ligaments. (B) Coronal view. The right atloepistrophic joint presents fusion and erosions (long light blue arrow) . Calcified apical ligament (short light blue arrow) and soft calcified alar ligaments. (C) Sagittal view. Massive erosion of the anterior surface and of the apex of the odontoid (long light blue arrow), calcified apical and alar ligaments (short light blue arrow). (D) Volume rendering view—The posterior view of the odontoid shows the calcified cruciate ligament (long light blue arrow) and calcified apex deposits (long light blue arrow).
Since she was already on NPX therapy, we started colchicine 2 mg on day 1, and 1 mg/day thereafter, but the day of MTX. Blood cultures and procalcitonin resulted negative. After 24 hours, she was better with no fever, and progressively she improved the cervical and wrists pain. At the latest follow-up, she had a cervical VAS pain of 3–4/10, no swollen wrists, and a CRP of 5.9 mg/L.
Discussion
Coexistent RA and CPPD has been well discussed by Krekeler et al,2 yet the involvement of the odontoid process and atlas by RA and the coexistent ‘CDS’ has never been described in the literature to our knowledge. In a retrospective series of 37 patients, Moshrif et al13 showed that cortical erosion of the posterior face of the odontoid, large erosion of the apex, erosive changes of the vertebral endplate and of the facet joints were seen, thus suggesting that even in our case CPPD could be the underlying diagnosis since the onset. We still maintained the coexistent diagnosis of RA and CPPD, because the involvement of both wrists, metacarpophalangeal joints, metatarsophalangeal joints and knees, thus a true polyarthritis, which is quite rare in CPPD14 and the good response to MTX over the years after a poliarticular acute onset, suggest that RA was the most likely diagnosis. In fact, in a randomised trial Finckh et al, after stressing that no specific treatment exists and that in patients refractory to non-steroidal anti-inflammatory drugs (NSAIDs) even glucocorticoids may fail, concluded that MTX had no strong effect on disease activity.15
In a retrospective study involving more than 2000 patients with acute neck pain, Goto et al16 observed that 60% of CDS were elderly female patients. In the radiological classification of CDS calcification may be present posterior (50%), posterolateral (27.5%), circular (12.5%), anterior (5%), lateral (5%) to the odontoid process. Importantly, in our patient the calcifications were in transverse, alar and apical ligaments.17
It is clear that CDS can be misdiagnosed as several conditions, including trauma, meningitis, discitis/osteomyelitis, giant cell arteritis, polymyalgia rheumatica, osteomyelitis, fever of unknown origin must be considered and as such an high index of suspicion, for this relatively benign condition is needed.18 In our case, in particular, the presence of fever, acute cervical pain in an RA patient already taking MTX and NPX raised several diagnostic queries and it was crucial to have the immediate answer through the CT scan that allowed us to avoid steroids and prefer the combination of NPX plus colchicine. This approach led to an almost immediate resolution of fever, and as reported in the literature steroids and NSAIDs may be sometimes unsuccesful.3 19 CDS may be detected in up to 2%–5% of patients over the age of 70 who present to hospital with severe neck pain,18 20 and since the CDS may cause chronic pain and even spinal cord compression, the diagnosis of simultaneous RA and CDS may represent a really challenging clinical setting. The prompt diagnosis of CDS led us to avoid lumbar puncture and CSF (cerebrospinal fluid) examination. In an interesting report from a neurosurgical unit in Japan, out of 554 patients admitted to the neurosurgical ward because of acute cervical pain, calcifications around the odontoid process were found in 15.8%, the age ranging between 60 and 96 years for those with calcifications and between 0 and 99 years for those without calcifications and found in 56 (22%) of 259 women compared with only 32 (11%) of 295 men, thus suggesting that elderly females are at greater risk.20 CDS should be always considered in the differential diagnosis in patients presenting with acute cervical pain especially in old females. This case also highlights the possibility of controlling the acute symptoms, resistant to NSAIDs (the patient was already taking NPX), with colchicine and without using corticosteroids, that in a patient with fever and possibly mimicking meningitis, should be, in our view avoided, unless CSF examination is made. The possible alternative approach could be interleukin 1 α/β antagonist which has been used in small case series.15
Ethics statements
Patient consent for publication
References
Footnotes
Contributors GF and EG cared for the patient in the acute phase of neck pain and followed up the patient over the following months and wrote the draft and finalised the paper. RZ performed the CT scan, prepared the images and discussed the paper. GF, RZ and EG approved the final draft.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
© Author(s) (or their employer(s)) 2023. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.