
Abstract
Background and aims
The concurrent decrease in fat free mass (FFM) and increase in fat mass (FM), including central obesity, in patients with rheumatoid arthritis (RA) may be related to increased cardiovascular morbidity as well as to functional decline. The objectives of this study were to evaluate body composition and nutritional status in patients with RA and the feasibility of bioelectrical impedance (BIA) to detect rheumatoid cachexia.
Methods
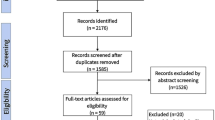
Eighty RA outpatients (76% women), mean age 61 (range 22–80) years and with mean disease duration of 6 (range 1–52) years, were assessed by body mass index (BMI), waist circumference (WC), whole-body dual-energy X-ray absorptiometry (DXA), BIA and the Mini Nutritional Assessment (MNA).
Results
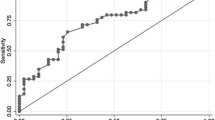
Fat free mass index (FFMI; kg/m2) was low in 26% of the women and in 21% of the men. About every fifth patient displayed concomitant low FFMI and elevated fat mass index (FMI; kg/m2), i.e. rheumatoid cachexia. BMI and MNA were not able to detect this condition. Sixty-seven percent had increased WC. Reduced FFM was independently related to age (p = 0.022), disease duration (p = 0.027), ESR (p = 0.011) and function trendwise (p = 0.058). There was a good relative agreement between DXA and BIA (FM r 2 = 0.94, FFM r 2 = 0.92; both p < 0.001), but the limits of agreement were wide for each variable, i.e. for FM −3.3 to 7.8 kg; and for FFM −7.9 to 3.7 kg.
Conclusion
Rheumatoid cachexia and central obesity were common in patients with RA. Neither BMI nor MNA could detect this properly. There was a good relative agreement between DXA and BIA, but the limits of agreement were wide, which may restrict the utility of BIA in clinical practice.


Similar content being viewed by others

Abbreviations
- BIA:
-
Bioelectrical impedance analysis
- BMI:
-
Body mass index
- DAS28:
-
Disease activity score calculated on 28 joints
- DXA:
-
Dual X-ray absorptiometry
- FFM:
-
Fat free mass
- FFMI:
-
Fat free mass index
- FM:
-
Fat mass
- FMI:
-
Fat mass index
- HAQ:
-
Health Assessment Questionnaire
- MNA:
-
Mini Nutritional Assessment
- RA:
-
Rheumatoid arthritis
References
Abernathy RP, Black DR (1996) Healthy body weights: an alternative perspective. Am J Clin Nutr 63:448S–451S
Alberti KG, Zimmet P, Shaw J (2006) Metabolic syndrome—a new world-wide definition. A Consensus Statement from the International Diabetes Federation. Diabet Med 23:469–480
Bland JM, Altman DG (1986) Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1:307–310
Calle EE, Thun MJ, Petrelli JM, Rodriguez C, Heath CW Jr (1999) Body-mass index and mortality in a prospective cohort of U.S. adults. N Engl J Med 341:1097–1105
Collins R Jr, Dunn TL, Walthaw J, Harrell P, Alarcon GS (1987) Malnutrition in rheumatoid arthritis. Clin Rheumatol 6:391–398
Ekdahl C, Eberhardt K, Andersson SI, Svensson B (1988) Assessing disability in patients with rheumatoid arthritis. Use of a Swedish version of the Stanford Health Assessment Questionnaire. Scand J Rheumatol 17:263–271
Elkan AC, Engvall IL, Tengstrand B, Cederholm T, Hafstrom I (2008) Malnutrition in women with rheumatoid arthritis is not revealed by clinical anthropometrical measurements or nutritional evaluation tools. Eur J Clin Nutr 62:1239–1247
Engvall IL, Elkan AC, Tengstrand B, Cederholm T, Brismar K, Hafstrom I (2008) Cachexia in rheumatoid arthritis is associated with inflammatory activity, physical disability, and low bioavailable insulin-like growth factor. Scand J Rheumatol 37:321–328
Hamdy O, Porramatikul S, Al-Ozairi E (2006) Metabolic obesity: the paradox between visceral and subcutaneous fat. Curr Diabetes Rev 2:367–373
Helliwell M, Coombes EJ, Moody BJ, Batstone GF, Robertson JC (1984) Nutritional status in patients with rheumatoid arthritis. Ann Rheum Dis 43:386–390
Hernandez-Beriain JA, Segura-Garcia C, Rodriguez-Lozano B, Bustabad S, Gantes M, Gonzalez T (1996) Undernutrition in rheumatoid arthritis patients with disability. Scand J Rheumatol 25:383–387
Kiebzak GM, Leamy LJ, Pierson LM, Nord RH, Zhang ZY (2000) Measurement precision of body composition variables using the lunar DPX-L densitometer. J Clin Densitom 3:35–41
Kyle UG, Bosaeus I, De Lorenzo AD, Deurenberg P, Elia M, Gomez JM, Heitmann BL, Kent-Smith L, Melchior JC, Pirlich M, Scharfetter H, Schols AM, Pichard C (2004) Bioelectrical impedance analysis—part I: review of principles and methods. Clin Nutr 23:1226–1243
Kyle UG, Piccoli A, Pichard C (2003) Body composition measurements: interpretation finally made easy for clinical use. Curr Opin Clin Nutr Metab Care 6:387–393
Manual Tanita BC-418 (2009) http://www.tanita.co.uk/index.php?id=95
Maradit-Kremers H, Nicola PJ, Crowson CS, Ballman KV, Gabriel SE (2005) Cardiovascular death in rheumatoid arthritis: a population-based study. Arthritis Rheum 52:722–732
Matarese LE, Steiger E, Seidner DL, Richmond B (2002) Body composition changes in cachectic patients receiving home parenteral nutrition. JPEN J Parenter Enteral Nutr 26:366–371
Munro R, Capell H (1997) Prevalence of low body mass in rheumatoid arthritis: association with the acute phase response. Ann Rheum Dis 56:326–329
Neovius M, Hemmingsson E, Freyschuss B, Udden J (2006) Bioelectrical impedance underestimates total and truncal fatness in abdominally obese women. Obesity (Silver Spring) 14:1731–1738
Podenphant J, Gotfredsen A, Engelhart M, Andersen V, Heitmann BL, Kondrup J (1996) Comparison of body composition by dual energy X-ray absorptiometry to other estimates of body composition during weight loss in obese patients with rheumatoid arthritis. Scand J Clin Lab Invest 56:615–625
Prevoo ML, van ‘t Hof MA, Kuper HH, van Leeuwen MA, van de Putte LB, van Riel PL (1995) Modified disease activity scores that include twenty-eight-joint counts. Development and validation in a prospective longitudinal study of patients with rheumatoid arthritis. Arthritis Rheum 38:44–48
Rall LC, Roubenoff R (2004) Rheumatoid cachexia: metabolic abnormalities, mechanisms and interventions. Rheumatology (Oxford) 43:1219–1223
Roubenoff R, Roubenoff RA, Ward LM, Holland SM, Hellmann DB (1992) Rheumatoid cachexia: depletion of lean body mass in rheumatoid arthritis. Possible association with tumor necrosis factor. J Rheumatol 19:1505–1510
Schutz Y, Kyle UU, Pichard C (2002) Fat-free mass index and fat mass index percentiles in Caucasians aged 18–98 y. Int J Obes Relat Metab Disord 26:953–960
Sun G, French CR, Martin GR, Younghusband B, Green RC, Xie YG, Mathews M, Barron JR, Fitzpatrick DG, Gulliver W, Zhang H (2005) Comparison of multifrequency bioelectrical impedance analysis with dual-energy X-ray absorptiometry for assessment of percentage body fat in a large, healthy population. Am J Clin Nutr 81:74–78
Thomson R, Brinkworth GD, Buckley JD, Noakes M, Clifton PM (2007) Good agreement between bioelectrical impedance and dual-energy X-ray absorptiometry for estimating changes in body composition during weight loss in overweight young women. Clin Nutr 26:771–777
Walsmith J, Roubenoff R (2002) Cachexia in rheumatoid arthritis. Int J Cardiol 85:89–99
WHO (1995) Report of a WHO expert committee, physical status: the use and interpretation of anthropometry. Technical report series, no 854, ISBN-139789241208543. http://www.who.int
Vellas B, Guigoz Y, Garry PJ, Nourhashemi F, Bennahum D, Lauque S, Albarede JL (1999) The Mini Nutritional Assessment (MNA) and its use in grading the nutritional state of elderly patients. Nutrition 15:116–122
Volgyi E, Tylavsky FA, Lyytikainen A, Suominen H, Alen M, Cheng S (2008) Assessing body composition with DXA and bioimpedance: effects of obesity, physical activity, and age. Obesity (Silver Spring) 16:700–705
Acknowledgments
Supported by grants from The Swedish Rheumatism Association, King Gustav V 80 year’s foundation, Capio, Stig Thunes found, the Swedish Research Council and The regional agreement on medical training and clinical research (ALF) between Stockholm county council and the Karolinska Institute. All authors contributed practically and/or intellectually to this study, as to design, collection of data and analysing data as well as writing or giving input to writing the manuscript. All authors read and approved the final manuscript.
Author information
Authors and Affiliations
Corresponding author
Additional information
This work has in part been presented at the Congress of American College of Rheumatology in San Francisco, October 2008.
Rights and permissions
About this article
Cite this article
Elkan, AC., Engvall, IL., Cederholm, T. et al. Rheumatoid cachexia, central obesity and malnutrition in patients with low-active rheumatoid arthritis: feasibility of anthropometry, Mini Nutritional Assessment and body composition techniques. Eur J Nutr 48, 315–322 (2009). https://doi.org/10.1007/s00394-009-0017-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00394-009-0017-y