Article Text

Abstract
Objective: To investigate the relationship between hand bone mineral density (BMD) and radiographic joint damage, and between hand BMD and fractures in 50–70 year old women with longstanding RA.
Methods: Demographic, clinical data, and imaging data on hand radiographs and Genants vertebral deformity score on spine radiographs were collected from 135 women with RA of ⩾5 years, recruited from three European rheumatology clinics. Metacarpal hand BMD was measured by digital hand x ray radiogrammetry (DXR), and hip and lumbar spine BMD by dual x ray absorptiometry (DXA). Multiple regression analyses were used to examine associations between hand BMD and radiographic joint damage, and hand BMD and fractures.
Results: Hand BMD was strongly and independently associated with radiographic hand joint damage in a linear regression model adjusted for age, centre, BMI, disease duration, RF, 18 deformed joint count, ESR, and femoral neck BMD. In a multivariate logistic regression model adjusted for relevant variables, hand BMD and femoral neck BMD, but not spine BMD, were independently associated with vertebral deformities and with non-vertebral fractures.
Conclusion: BMD measured by DXR on conventional hand radiographs in patients with RA may potentially be used as an indicator of joint damage and of vertebral and non-vertebral fracture risk.
- ANOVA, analysis of variance
- BMD, bone mineral density
- BMI, body mass index
- CV, coefficient of variation
- DXA, dual x ray absorptiometry
- DXR, digital x ray radiogrammetry
- ESR, erythrocyte sedimentation rate
- RA, rheumatoid arthritis
- RF, rheumatoid factor
- rheumatoid arthritis
- osteoporosis
- radiographic joint damage
- fractures
- imaging
Statistics from Altmetric.com
- ANOVA, analysis of variance
- BMD, bone mineral density
- BMI, body mass index
- CV, coefficient of variation
- DXA, dual x ray absorptiometry
- DXR, digital x ray radiogrammetry
- ESR, erythrocyte sedimentation rate
- RA, rheumatoid arthritis
- RF, rheumatoid factor
In rheumatoid arthritis (RA) the osteoclast cell plays a major part in the development of bone erosions and osteoporosis, both periarticular and generalised. However, data are lacking on the relationship between these osteoclast cell driven features and both hand bone mass and fractures.
In this cross sectional study we explored the association between hand bone mineral density (BMD) measured by digital x ray radiogrammetry (DXR), firstly, with radiographic joint damage, and secondly, with fractures (vertebral deformities and non-vertebral fractures).
PATIENTS AND METHODS
Study group and clinical variables
One hundred and thirty five female patients with RA were recruited from a recently published European three centre cross sectional study examining 150 patients, aged 50–70 years, with disease duration of ⩾5 years.1 Fifteen patients from the original cohort were excluded from the current analysis owing to technical problems in assessing hand BMD with DXR, related to severe joint damage. Demographic and clinical variables were obtained on interview and clinical examination (table 1⇓). This data collection has previously been described in detail.1 Hand radiographs were read according to the modified Larsen method (range 0–120). Vertebral deformities were scored according to Genants semiquantitative method, which grades vertebral height reduction at T4–L4 into grade 0 (normal), 1 (20–25% reduction), 2 (25–40% reduction), and 3 (>40% height reduction). A scoring of at least grade ⩾1 was considered a deformed vertebra.
Patient characteristics of the 135 female patients with RA. Mean (SD) for continuous variables; percentage for counts
BMD measurement
BMD measurements of the lumbar spine and the femoral neck were performed using dual x ray absorptiometry (DXA) as described previously.1 The DXA machines were cross calibrated and long term spine phantom precision ranged from 0.4% to 0.8% expressed as coefficient of variation (CV). In vivo short term CV ranged from 1.2% to 1.6% at the femoral neck, and from 0.7% to 2.5% at the lumbar spine L2–4.
Hand BMD was measured on plain radiographs of the hand (anteroposterior view) using DXR (Pronosco x posure System, system 2.0), a computerised version of the traditional technique of radiogrammetry measuring cortical bone thickness as originally proposed by Barnett and Nordin.2 A “surrogate” mean BMD value was calculated from this cortical thickness from the regions of interest measured at the 2nd, 3rd, and 4th metacarpal joints. The theoretical background for this validated method has been described elsewhere in detail.3 Long term precision based on daily measurement of one hand radiograph was 0.2%. The in vivo precision of the DXR hand measurements was assessed by measuring radiographs of 24 randomly selected patients twice, showing a CV of 0.4%. For hand BMD we used the mean value of the left and the right hand.
Statistical analyses
Group comparisons were performed by two tailed independent Student’s t test (continuous variables) and χ2 test (categorical variables).
Correlations between Larsen score and hand, hip, and spine BMD were examined by Pearson’s correlation coefficient. BMD reduction at the different measurement sites was also explored by comparing BMD levels across quartiles of the Larsen score, using the lowest quartile as reference category. For multiple group comparison of the quartile Larsen groups we used analysis of variance (ANOVA).
Based on the results of the corresponding univariate regression analyses (p<0.20) and supposed clinical relevance, variables were added to the respective multiple regression models. Multivariate linear regression analyses were used to explore the associations between radiographic damage (dependent variable) and hand BMD (independent variable), adjusting for age, body mass index (BMI), centre, disease duration, rheumatoid factor (RF), deformed joint count, mean erythrocyte sedimentation rate (ESR) during the past 12 months, and femoral neck BMD. Multivariate logistic regression analyses were used to explore the association between the presence of fractures (dependent variable) and BMD at the different measurement sites (independent variable), adjusting for age, BMI, and centre (for non-vertebral fractures, also adjusted for disease duration).
All analyses were performed with the SPSS statistical package. Values of p⩽0.05 were considered significant.
RESULTS
Table 1⇑ shows the patient characteristics. Table 2⇓ shows the variables with a statistically significant difference between the 135 patients included and the 15 patients excluded.
Clinical characteristics of female patients with RA with and without hand bone density measured. Mean (SD) for continuous variables; percentage for counts
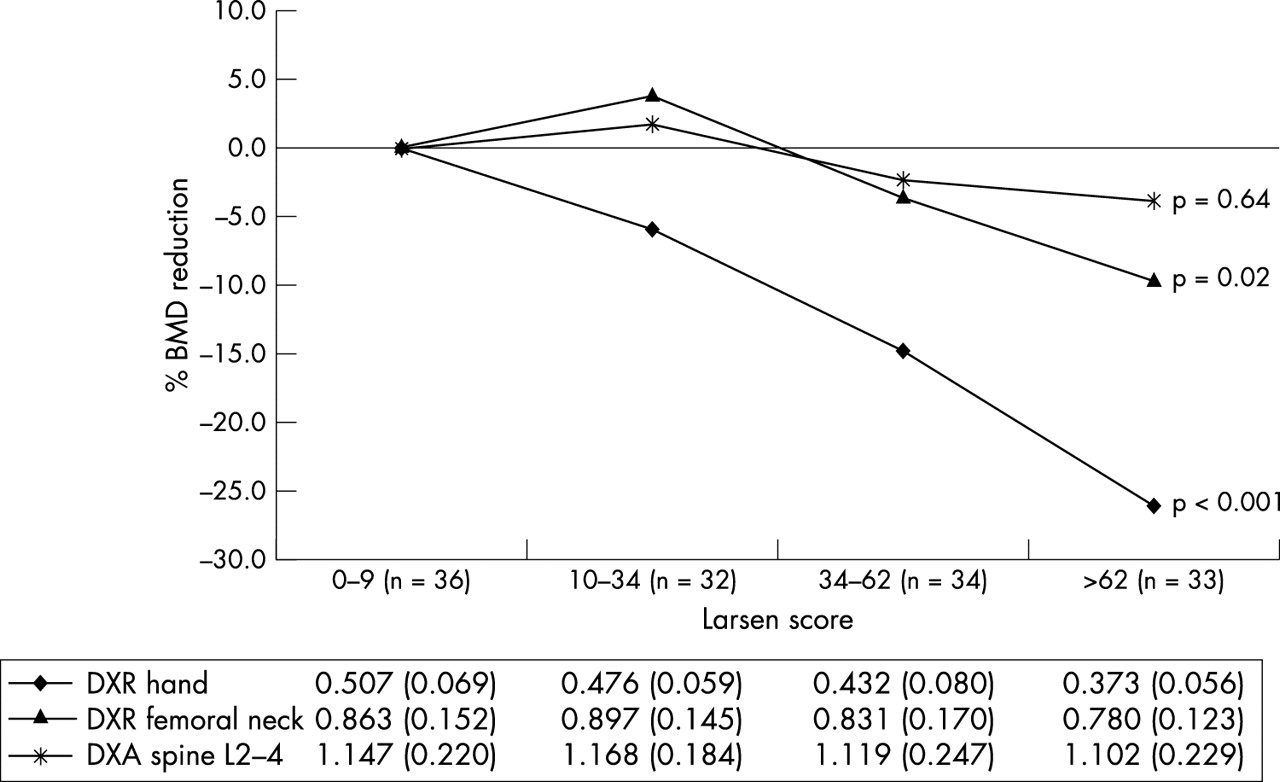
A high Pearson correlation coefficient was found between hand Larsen score and DXR hand BMD (r = −0.62, p<0.001), a moderate correlation with DXA femoral neck BMD (r = −0.27, p = 0.002), and no significant association with DXA spine L2–4 (r = −0.10, p = 0.26). The strong association between hand DXR and radiographic damage was also confirmed when BMD reductions were examined across quartiles of scores for radiographic damage (fig 1⇓).
{kind=link}
Mean percentage reduction of BMD at hands, femoral neck, and spine (L2–4) related to quartile groups of radiographic damage using the lowest quartile of Larsen score as reference category. Below the figure mean (SD) BMD (g/cm2) values for each quartile of the Larsen score are shown. p Values from overall ANOVA (statistically significant group differences using post hoc Bonferroni test): hand BMD: 1st quartile v 3rd and 4th quartile, 2nd quartile v 3rd and 4th quartile, and 3rd quartile v 1st, 2nd, and 4th quartile; femoral neck BMD: 2nd quartile v 4th quartile.
DXR hand BMD reduction was more pronounced than DXA BMD reduction at the femoral neck and spine L2–4 (fig 1⇑). In patients with RA in the highest Larsen quartile, DXR hand BMD was 26% lower, femoral neck BMD 10% lower, and spine L2–4 BMD 4% lower than in patients in the lowest quartile group (reference category).
In the final linear multivariate model, age, centre (dummy variables), disease duration, deformed joint count, mean ESR past 12 months, and hand BMD were independently associated with Larsen score, even after controlling for femoral neck BMD. The association between hand BMD and Larsen score was particularly strong with a β value of −163.1 (p<0.001), whereas the β values for the other significantly associated clinical variables ranged from −0.6 to 2.0.
In the final multivariate logistic regression model adjusting for age, BMI, and centre, adding BMD at hand, femoral neck, and spine subsequently, the model showed that DXR hand BMD (p = 0.04) and DXA femoral neck BMD (p = 0.01), but not DXA spine BMD (p = 0.11), were independently associated with vertebral deformities. When hand BMD and femoral neck BMD were both included in the model, the association between vertebral deformities and BMD was no longer present.
In the final multivariate logistic regression model adjusting for age, BMI, centre, disease duration, and investigating BMD at the hand, femoral neck, and spine subsequently in the model, showed that DXR hand BMD (p = 0.03) and DXA femoral neck BMD (p = 0.003), but not DXA spine BMD (p = 0.07), were independently associated with non-vertebral fractures. When hand BMD and femoral neck BMD were both included in the model, the association between non-vertebral fractures and BMD disappeared.
DISCUSSION
The main finding from this cross sectional study is that hand BMD is strongly associated with radiographic joint damage, and this strong association is present even after adjusting for the femoral neck BMD. Hand BMD was also significantly associated with the presence of both vertebral deformities and non-vertebral fractures.
Considerable evidence supports the statement that inflammation in RA is related to the progression of joint damage, on the one hand,4 and to the development of both periarticular and generalised osteoporosis, on the other. An association between radiographic joint damage and hand bone mass in RA has been found by different bone measurement devices—for example, DXA,5 quantitative ultrasound,6 and manual radiogrammetry measured as combined cortical thickness of the second metacarpal bone.7 Others have also, described a strong (r ∼ 0.6) and highly significant (p ∼ <0.01) inverse correlation between hand bone mass and radiographic damage.5,7 In our study it was demonstrated that this strong association remained present even after adjusting for a variety of other relevant measures, including age, BMI, disease duration, RF, deformed joint count, mean ESR past 12 months, and femoral neck BMD. In RA, erosive disease was also found to be independently associated with measures of generalised bone loss assessed with DXA at hip and lumbar spine,1,8,9 suggesting a close relation between bone loss and joint damage in RA.
Fracture data are lacking in RA for both the extent and the association with measures of bone density. A recent case-control study examining female patients with RA recruited from a community based RA register had an odds ratio for both multiple and moderate/severe deformities of 2.6 compared with population based controls matched for age and sex.10 In that study the presence of vertebral deformities was associated with BMD, the use of corticosteroids, but also, independently, with the diagnosis of RA itself. The latter finding is interesting seen in the light of the cross sectional RA study by Lodder et al,1 which found that radiographic joint damage (Larsen score) was an independent determinant of vertebral deformities. In our study both hand DXR BMD and DXA femoral neck BMD were to a similar extent significantly associated with both vertebral deformities and non-vertebral fractures, but this was not seen for lumbar spine BMD. This might be explained by the fact that disease related bone loss in RA is more pronounced at the hand and hip than at the spine.11 Another possible explanation might be related to, for example, osteoarthritis of the spine and vertebral deformities, artificially increasing measured BMD12 without increasing vertebral bone strength. The potential beneficial effect of hand DXR is that from conventional hand radiographs information on both radiographic damage bone mass and fracture risk could be provided.
The promising results from this study, which examined hand DXR BMD as a marker of joint damage and as an indicator of fracture risk in patients with RA, should be examined in further studies, especially longitudinal studies, before final conclusions on its use in clinical practice can be drawn.
Acknowledgments
We thank Liz Stanley for assistance in Truro and Pieter Prins in Amsterdam for reading the hand radiographs. We gratefully appreciate the technical assistance of Anders Strand, Ingerid Müller, Sidsel Arnkværn, Margareth Sveinsson, and Ann Katrine Kongtorp in Oslo, Elaine Cotton in Truro, and Ems van Vloten and Helen Wieringa in Amsterdam.