Article Text

Abstract
Objective: To evaluate the efficacy and tolerability of anti-tumour necrosis factor α (TNFα) monoclonal antibody (infliximab) in the treatment of spondyloarthropathy (SpA) associated with active and inactive Crohn’s disease (CD).
Methods: Twenty four patients with SpA associated with active or inactive CD (16 active, 8 quiescent) were treated with anti-TNFα monoclonal antibody (infliximab) with repeated infusions for a period of 12–18 months. The treatment aimed at ameliorating the general musculoskeletal and spinal pain, controlling peripheral arthritis and enthesitis, decreasing the BASDAI score, modifying acute phase reactants, and reducing CD activity.
Results: Infliximab improved both gastrointestinal (p<0.01) and overall articular symptoms (BASDAI, p<0.01; general musculoskeletal and spinal pain, p<0.01; peripheral arthritis, p<0.01) in patients with active CD. Additionally, infliximab effectively controlled not only axial involvement and peripheral arthritis but also enthesitis (p<0.01) and prevented inflammatory bowel disease reactivation in patients with inactive CD and low inflammatory markers. Amelioration of gut and musculoskeletal involvement persisted for up to 12 months.
Conclusion: Infliximab may act on the inflammation of entheses and of periarticular structures, which usually does not cause a change in the haematological markers that are the main indicators of pain and joint ankylosis in SpA. Infliximab induces and maintains remission of CD while at the same time treating active and severe SpA, suggesting that it should be the preferred drug for the treatment of active and severe SpA associated with active or quiescent CD.
- BASDAI, Bath Ankylosing Spondylitis Disease Activity Index
- CD, Crohn’s disease
- CDAI, Crohn’s Disease Activity Index
- CRP, C reactive protein
- ESR, erythrocyte sedimentation rate
- IBD, inflammatory bowel disease
- NSAIDs, non-steroidal anti-inflammatory drugs
- RA, rheumatoid arthritis
- SpA, spondyloarthropathy
- TNFα, tumour necrosis factor α
- US, ultrasonography
- VAS, visual analogue scale
- infliximab
- Crohn’s disease
- spondyloarthropathies
Statistics from Altmetric.com
- BASDAI, Bath Ankylosing Spondylitis Disease Activity Index
- CD, Crohn’s disease
- CDAI, Crohn’s Disease Activity Index
- CRP, C reactive protein
- ESR, erythrocyte sedimentation rate
- IBD, inflammatory bowel disease
- NSAIDs, non-steroidal anti-inflammatory drugs
- RA, rheumatoid arthritis
- SpA, spondyloarthropathy
- TNFα, tumour necrosis factor α
- US, ultrasonography
- VAS, visual analogue scale
Musculoskeletal manifestations are the most common extraintestinal complication of inflammatory bowel disease (IBD)—in particular, Crohn’s disease (CD). These manifestations are usually included in the clinical spectrum of spondyloarthropathies (SpAs). The strong link between the bowel and the locomotor system in SpA is also supported by the evidence that inflammatory alterations of intestinal mucosa and its permeability (usually at the ileum) are present when symptoms are mild or subclinical in a high percentage of patients affected by any SpA without a manifest IBD.1 Different patterns of articular involvement have been recognised in IBD: type I, peripheral pauciarticular arthritis; type II, peripheral non-symmetric polyarthritis; and type III, an SpA resembling idiopathic ankylosing spondylitis, sometimes with peripheral joint involvement.2 In addition to axial and peripheral articular symptoms, enthesitis, tenosynovitis, and dactylitis commonly occur, sometimes representing the only manifestation3 and often causing severe and continuous discomfort, with a significant reduction of the quality of life of the patient. Type I arthritis may precede the diagnosis of IBD and, once established, often parallels the activity of the intestinal manifestation. Types II and III arthritis do not reflect the activity of the underlying IBD and rarely precede the diagnosis of IBD.
Efficacy and safety in the management of these conditions, especially when associated, is difficult to achieve. In fact, SpAs are often poorly responsive to disease modifying drugs, and the possibility of a drug triggered intestinal activation or relapse significantly limits the use of several drugs.
Tumour necrosis factor α (TNFα) is a so called “master cytokine” which has a key role in the regulation of innate immunity and in the local inflammatory response of several pathogenetically distinct diseases.4 In particular, TNFα is important in the genesis and maintenance of synovitis in rheumatic disorders and of mucosal inflammation in IBDs.
Infliximab is a chimeric anti-TNFα monoclonal IgG1 antibody, neutralising soluble cytokines and blocking membrane bound cytokines.5 For this reason, infliximab has been initially successfully used in patients with rheumatoid arthritis (RA).6,7 Infliximab is remarkably effective in patients with RA presenting with persistent active disease despite adequate treatment with methotrexate.8 The clinical response after 1 year of treatment (American College of Rheumatology 20%) has reached efficacy of 42–59%.9
Infliximab has been also used in CD. It induces remission of symptoms, closure of fistulae, healing of lesions, and improvement in the quality of life. A beneficial effect on extraintestinal complications, including articular complications, has been seen.10–14
These observations and the close relation between gut inflammation and joint involvement in patients with SpA, have suggested the use of infliximab in ankylosing spondylitis. Although the bulk of experience in this disease is not comparable with that of RA and CD, substantial evidence now suggest that infliximab is highly effective and well tolerated for both axial and peripheral joint disease in patients with active ankylosing spondylitis.15–17 Some reports of the use of infliximab in other SpA have also been published.18–21 By contrast with ankylosing spondylitis, few studies have examined the specific treatment of SpA associated with CD. One open, short term study of four patients with SpA associated with active CD (three patients with peripheral arthritis, one with prominent axial involvement) showed that infliximab induces a fast improvement of articular manifestations and remission of active intestinal disease.22 Another prospective, open label study from Herfarth et al evaluated the incidence of arthritis and arthralgia in a group with chronic active CD (153 patients) and the effect of infliximab on articular symptomatology after 12 weeks of treatment.23 All the patients presenting any musculoskeletal symptom, and not only those with a clear SpA, were included in the study. Musculoskeletal symptoms were evaluated by clinical examination and graded on a four point scale (severe, moderate, mild, and none) with no distinction between the different patterns of articular involvement (peripheral arthritis, axial involvement, enthesitis). Infliximab significantly reduced the arthritis/arthralgia score in this cohort of patients.
TNFα blockade with the other biological agent, etanercept, is effective in the treatment of SpA but not in the treatment of colitis. The persistence or flaring of CD despite the complete resolution of spinal pathology in two patients treated with etanercept has been reported.24
Our work aimed at investigating the efficacy and safety of a short and long term regimen of infliximab in the treatment of patients with SpA who also presented with, or had experienced in the past, intestinal inflammation due to CD.
PATIENTS AND METHODS
Twenty four patients with active SpA associated with CD (14 male, 10 female; mean (SD) age 44 (10) years) referred to the departments of medicine of the University of Florence and L’Aquila (Italy) were selected for the study. At baseline, 16 patients presented active CD (mean (SD) disease duration 9.9 (5.3) years), while 8 patients had quiescent CD (mean disease duration 10.3 (4.6) years). A further 12 additional patients presenting active CD (mean disease duration 9.16 (3.3) years) and similar articular disease served as controls and were treated conventionally (see below).
All patients had active and severe SpA (mean disease duration 9.9 (6.3) years) fulfilling European Spondylarthropathy Study Group (ESSG) criteria25 and characterised by axial involvement (25/36 subjects) and/or peripheral arthritis (23/36), and/or enthesopathy (25/36), poorly or not responsive to conventional treatments (non-steroidal anti-inflammatory drugs (NSAIDs), sulfasalazine, systemic and local steroids, physiotherapy) or for whom previous treatments had induced a worsening or a relapse of the gastrointestinal symptoms.
Disease activity was assessed by the Bath Ankylosing Spondylitis Disease Activity Index (BASDAI); visual analogue scale (VAS) for general musculoskeletal pain; separate VAS for spinal pain; presence of peripheral arthritis/synovitis; presence of active enthesitis or periarticular inflammation. The diagnosis of peripheral arthritis and active enthesitis was confirmed by ultrasonography (US). Peripheral arthritis was considered present when at least one peripheral joint showed swelling and tenderness, with documented joint effusion. The number of affected joints was not taken into account because most of the patients with peripheral arthritis had mono- or pauciarticular disease. Enthesitis and periarticular inflammation were defined both clinically (pain at pressure or mobilisation) and by US in the most commonly affected sites of insertion (greater trochanter, ischial tuberosity, pubis, patellar poles and tibial tuberosity, posterior and inferior calcaneus, medial and lateral epicondyles, chondrosternal and manubriosternalis junctions). US (ESAOTE AU5 epi, linear probe 7.5–12 MHz, pwD dynamic range 50 sB, PRF 750 Hz) was performed by an experienced echographer who was unaware of the clinical and biological findings. Oedema, thickening, erosions at the enthesis junction and increased flow by pwD were considered pathological. Enthesitis was considered active in the presence of both pain and US abnormalities due to current inflammation (oedema, thickening, and increased flow). Enthesitis was considered present when at least one site showed signs of active inflammation.
SpA was considered active in patients presenting a BASDAI >40 and VAS for general musculoskeletal pain >40, persisting for at least 4 months.
All the variables were assessed at baseline and then at each infliximab infusion.
The activity of CD was evaluated by “Crohn’s Disease Activity Index” (CDAI),26 recorded by the patients during the 7 days before each infusion and during the 4th week after the last infusion. The disease was considered active when the score was higher than 150.
Laboratory evaluation, including erythrocyte sedimentation rate (ESR), C reactive protein (CRP), routine hepatic and renal measures, and complete blood count, was also carried out at baseline and before each infusion of infliximab or at the corresponding time for the control group.
Treatment
The patients with active CD received three infusions of 5 mg/kg infliximab (at weeks 0, 2, and 6) and later on infusions of 3 mg/kg infliximab, if the bowel disease had remitted, or 5 mg/kg when it persisted, every 5–8 weeks according to the duration of therapeutic effect (medium (SD) interval between the infusions 44.2 (9.3) days). The patients who presented inactive CD at baseline were treated with 3 mg/kg infliximab from the first dose with the same schedule (fig 1). All the patients were treated with infliximab for at least 12 months. After 12 months, the patients continued the treatment (apart from those who stopped owing to side effects or inefficacy); however, data at 18 months are available only for 12 patients.

Therapeutic flow chart for the treatment of active SpA associated with active or inactive CD.
All the patients were allowed to continue the pharmacological treatment and physiotherapy they were undergoing before the study if no modifications had occurred during the previous months (3 months for 5-aminosalicylic acid compounds, 1 month for NSAIDs and steroids).
The control patients, all with active CD at baseline, received a variety of other drugs commonly employed in CD (oral azathioprine 2.5 mg/kg/day, topical and systemic salicylates, topical and systemic steroids, antibiotics, metronidazole).
The continued use of oral 5-aminosalicylic acid compounds and steroid or 5-aminosalicylic enemas was allowed within the definition of remission.
Statistical analysis
Primary end points analysed were the BASDAI score, the VAS for musculoskeletal pain, ESR, CRP, and CDAI at 45 days, 6 months, and 12 months after the start of treatment. Variables are presented as the mean (SD), unless stated otherwise. SPSS-PC was used for data analysis. Comparison between baseline and subsequent assessments was performed with the Wilcoxon matched pairs signed rank test. The efficacy of the treatment in comparison with the control treatment was assessed by analysis of variance. The results were considered significant at p<0.05. Correlations between variables were assessed using the Pearson rank correlation coefficient. A partial correlation test was used to study the relation between the same variables after treatment had started.
RESULTS
Musculoskeletal involvement
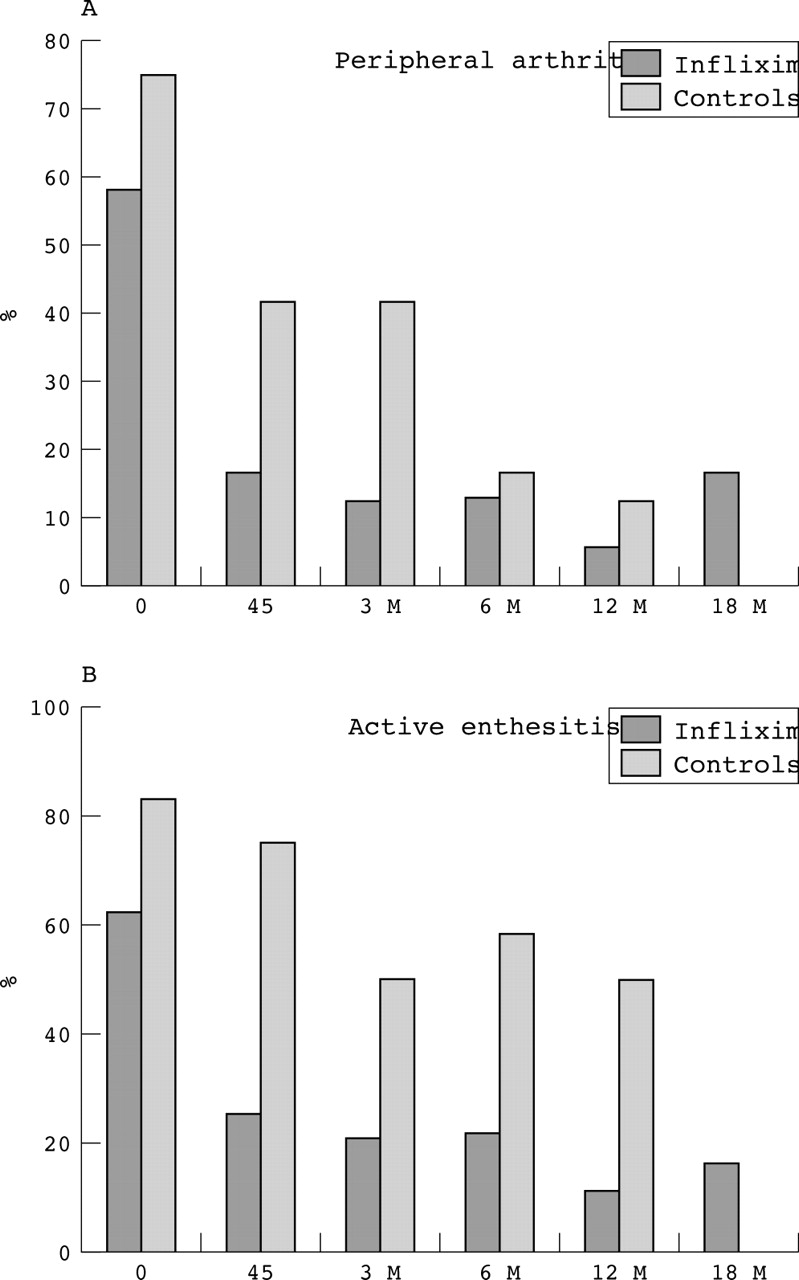
All patients treated with infliximab had significantly improved articular and periarticular manifestations of SpA, both axial and peripheral (table 1, figs 2C and 3). In these patients, the BASDAI score showed a dramatic and prompt decrease (p<0.01), which persisted throughout the treatment (fig 2A). The BASDAI score was also significantly reduced in the control group (p<0.05) but almost never below 40 (the appointed limit for active disease). The reduction of BASDAI due to infliximab was more significant than that due to other treatments (p<0.05). Infliximab significantly and rapidly reduced peripheral arthritis (from 58% to 12.5% after 6 months, from 55.5% to 11.1% after 1 year and from 50% to 16.6% in the patients who prolonged their treatment for up to 18 months) (fig 3A). Patients of the control group had a slower but progressive amelioration of peripheral arthritis, which was comparable to that of the infliximab group after 6 and 12 months (from 75% to 17% and 12.5%, respectively) (fig 3A). From the first infusions, infliximab produced a clear decrease of active enthesitis (fig 4), which persisted at 6 months (from 67% to 24%), at 12 months (from 60% to 10%), and at 18 months (from 58.3% to 16.6%) (fig 3B). In many of the patients who did not achieve a complete remission of enthesitis the number of sites of inflammation was reduced or the clinical manifestations of enthesitis improved (data not shown). The control treatments had little effect on enthesitis (fig 3B). Finally, infliximab decreased both the general musculoskeletal and the spinal pain to a significant extent (p<0.01) (fig 2C). This effect was significantly higher than in control group (p<0.05) (fig 2C).
Clinical and laboratory data of the patients with SpA and CD at baseline and during treatment with infliximab or various other conventional treatments (oral azathioprine 100 mg daily, topical and systemic salicylates, topical and systemic steroids, antibiotics, metronidazole)

(A, B, C) Clinical and laboratory data (mean) of the patients with SpA and CD at baseline and during treatment with infliximab or various other conventional treatments (baseline, 45 days, 3, 6, 12, 18 months). The values of CDAI are split into two additional groups: patients with active or inactive CD at baseline.
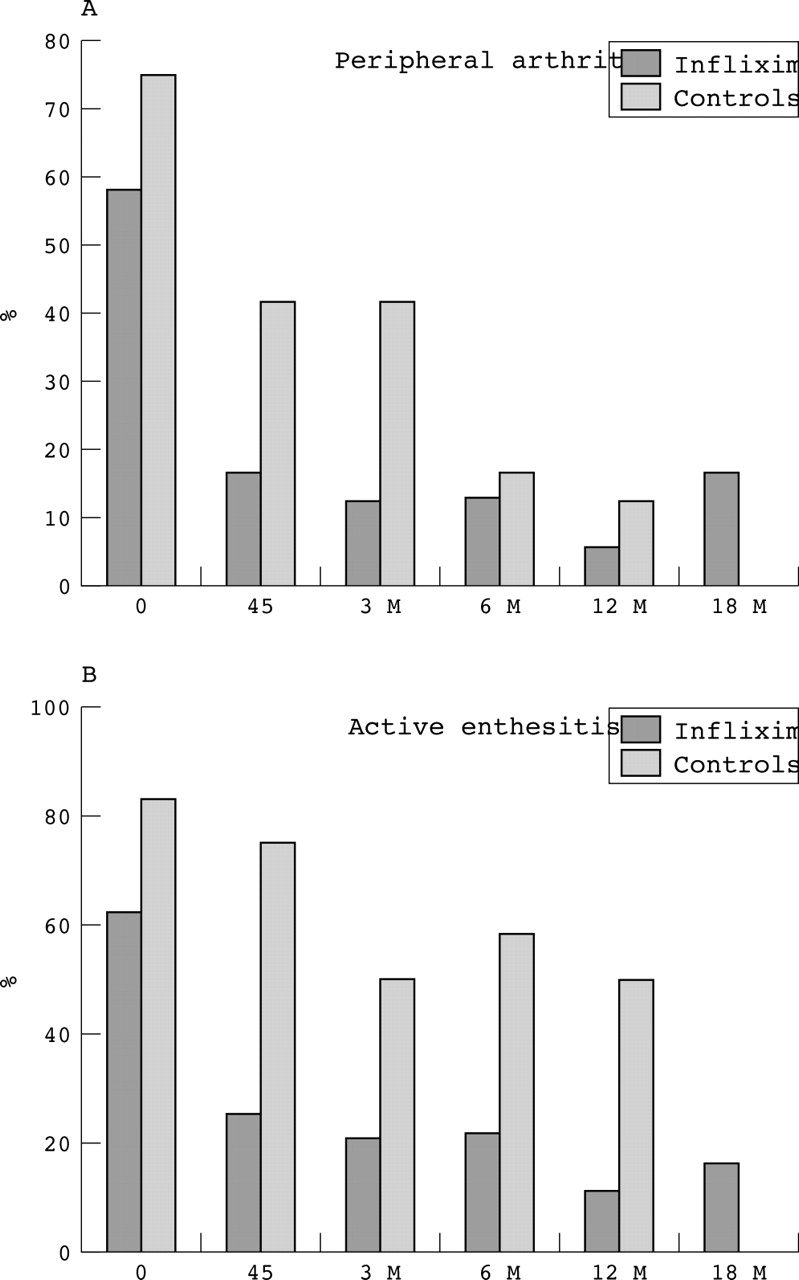
Percentage of patients presenting peripheral arthritis (A) or active enthesitis (B) at baseline and during the treatment (45 days, 3, 6, 12, 18 months) with infliximab or various other drugs (azathioprine, mesalazine, steroids, metronidazole, antibiotics). *The data reported at 12 months are relative to patients (10/21) who prolonged the treatment with infliximab for up to 12 months; no controls are available for this group.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A) Thickening and homogeneous hypoechogenicity of the Achilles tendon enthesis with distension of the retrocalcaneal bursa (arrows) which disappeared after 45 days of treatment with infliximab (B).
No patients used analgesic or anti-inflammatory drugs during the treatment with infliximab. At 12 months, three patients of the control group started infliximab treatment because of the persistence of severe spondyloarthritic symptoms (table 1).
Gastrointestinal involvement
In patients with active CD, infliximab induced a remarkable improvement of gastrointestinal signs and symptoms, with significant reduction of CDAI after the first two infusions (p<0.01), which was maintained over 45 days (p<0.01), 3, 6, and 12 months (p<0.01) (table 1). After 6 months, four patients still presented active CD and for this reason three of them had to take oral steroids. After 12 months, two patients stopped the treatment with infliximab because of CD relapse and took other immunosuppressant drugs (table 1). None of the eight patients with inactive CD at baseline had exacerbation of their disease during the study.
The patients of the control group also showed a reduction of the CDAI, which persisted over the 12 months of study (p<0.01). At 12 months, one patient interrupted treatment with conventional drugs and started infliximab because bowel inflammation was reactivated. Notably, no significant difference in the ability to induce and maintain remission of CD was seen between infliximab and the control treatments. In most patients, the treatments significantly and rapidly reduced laboratory inflammatory measures (ESR and CRP) (table 1). Indeed, a significant reduction of these measures was also seen in patients with inactive CD (p<0.05) (data not shown).
Correlations between variables
At baseline, the following correlations were found: ESR correlated with CRP (r = 0.79; p = 0.002) and, slightly, with CDAI (r = 0.67; p = 0.06) and peripheral arthritis (r = 0.69; p = 0.054); CRP also showed a very mild correlation with peripheral arthritis (r = 0.66; p = 0.83); BASDAI correlated only with general musculoskeletal pain (r = 0.69; p = 0.054). Notably, BASDAI, as well as axial pain and enthesitic involvement, did not correlate with theacute phase reactants. None of the pharmacological treatments significantly modified these correlations.
Tolerability
Infliximab was well tolerated throughout the study. One patient stopped the treatment after 6 months owing to an allergic reaction after the infusion (cough, dyspnoea, flush) (table 1). Other minor side effects were headache, dizziness, and transient leucopenia that regressed spontaneously and required treatment to be interrupted. No infections occurred.
In the control group, two patients treated with azathioprine had nausea and vomiting, one patient treated with mesalazine and metronidazole had a transient rise in γ-glutamyltransferase that required reduction of the drugs.
DISCUSSION
In enteropathic arthopathies, management of bowel inflammation is the main task because this may indirectly induce remission of musculoskeletal manifestations. However, in a large number of patients, despite the amelioration or disappearance of gut inflammation, joint disease persists.2 In these cases, NSAIDs must be carefully used because of the possibility of gastrointestinal side effects and of IBD activation. Indeed, steroids and disease modifying antirheumatic drugs are often ineffective in controlling axial pain and enthesitis27 and, with the exception of sulfasalazine, they cannot completely prevent relapse of bowel inflammation.
When both intestinal disease and arthropathy are in an active phase, the preferred drugs are those potentially effective on the inflammation in both areas. Sometimes, even though CD is in remission and laboratory inflammatory markers are normal or scarcely altered, the musculoskeletal symptoms associated with SpA may persist. In these cases, control of the musculoskeletal symptoms, especially enthesitis and spinal pain that potentially mirror progression of the disease towards ankylosis,28 becomes the primary task together with the restoration of the quality of life.
Our preliminary data are generated in an open study but confirm that infliximab controls the inflammation and the symptoms of SpA associated with active CD. Moreover, infliximab significantly controls musculoskeletal pain derived not only from axial and peripheral articular involvement but also enthesitis, even in patients with quiescent CD and with no or moderate increase of acute phase reactants.
Almost all of our patients reported the disappearance of enthesitis, strongly suggesting that infliximab specifically acts on inflammation of periarticular structures. It is well known that entheseal involvement does not alter haematological measures but is evidence of the persistence of disease activity and may contribute to joint ankylosis.28
The positive results, promptly achieved after the first infusions, persisted over the whole treatment and the infusions were reasonably well tolerated. In the control group (especially in patients treated with azathioprine, data not shown) the treatment effectively controlled gut inflammation, peripheral arthritis, and acute phase reactants but it had a poor effect on axial and enthesitic pain. The results of treatment were better in patients with pauciarticular peripheral disease, which often parallels the activity of the intestinal manifestation, the so called “type I”.2
In conclusion, infliximab, because of its remarkable anti-inflammatory effect on both the articular and intestinal systems, may be a pivotal treatment in severe SpA associated with active CD, often presenting with peripheral arthritis and increased acute phase reactants. Moreover, because infliximab acts on all musculoskeletal inflammatory components of SpA and, at the same time, maintains the remission of gut inflammation, it may be a useful therapeutic tool also for patients with inactive CD and modest laboratory signs of inflammation but who have persistent and severe axial and enthesitic pain. Extension of the treatment beyond the standard three infusions, usually reserved for active CD, may be advisable in both types of patient if inflammation persists. In IBDs and SpA, double blind studies with infliximab are warranted to verify these data and evaluate the efficacy and tolerability of the drug in long term use.