Article Text

Abstract
Objective: Fcγ receptor (FcγR) polymorphism influences the affinity of the receptor for Ig, which may, in turn, affect the efficacy of Ig-based therapies. The relationship between functional single nucleotide polymorphisms (SNP) of the FCGR2A and FCGR3A genes and the response to anti-tumour necrosis factor (TNF)α therapy (infliximab) in patients with rheumatoid arthritis (RA) was assessed.
Methods: A total of 91 patients with RA (89% female; 76.7% rheumatoid factor (RF) positive) starting therapy with infliximab were evaluated at 0, 6 and 30 weeks using the American College of Rheumatology (ACR) and European League Against Rheumatism (EULAR) response criteria and the 28-joint Disease Activity Score (DAS28) was evaluated using three parameters, including C-reactive protein (CRP) (DAS28 3v-CRP) changes during the follow-up. Genotyping of FCGR2A-R131H and FCGR3A-F158V polymorphisms was performed by allele-specific PCR and PCR sequence-based typing, respectively. The χ2 and Fisher exact tests were used to show differences in the outcome variables, and analysis of variance (ANOVA) to analyse the evolution of DAS28 3v-CRP. A generalised linear models multivariable analysis was also performed.
Results: At week 6 of follow-up, the proportion of patients achieving 50% improvement as per ACR criteria (ACR50) and EULAR good responses were significantly higher among homozygotes of the low affinity FCGR3A allele (FF: 24.1% and VV-VF:2.2%; p = 0.003 and FF: 44.8% and VV-VF: 22.9%; p = 0.040, respectively). At week 30, homozygotes of the low affinity FCGR2A allele had a better ACR20 response (RR: 60% and HH-RH: 33.3%; p = 0.035). Changes in DAS28 3v-CRP during follow-up were consistent with those observed in ACR and EULAR responses.
Conclusions: The response to anti-TNFα treatment with infliximab in patients with RA is influenced by the FCGR2A and FCGR3A genotypes. This effect is observed at different times in the follow-up (6 and 30 weeks, respectively) indicating the dynamic nature of the FcγR versus Ig interaction.
Statistics from Altmetric.com
The use of biological therapies targeting key proinflammatory molecules and their receptors has emerged as a powerful tool for the control of systemic inflammatory disorders in recent years. In most cases, this is achieved by the use of chimeric and humanised monoclonal IgG antibodies (ie, infliximab, rituximab and adalimumab) or fusion proteins consisting of the molecule of interest fused to the constant region (Fc) of human IgG (ie, etanercept and abatacept). The Fc portion of these biological agents binds specifically to cell surface Fcγ receptors (FcγR) and this may affect their half life and certain innate and adaptive immune responses, such as phagocytosis and antibody-dependent cellular cytotoxicity (ADCC).
Three major classes of human FcγR have been reported, encompassing eight genes (FCGR1 A, B and C; FCGR2 A, B and C; FCGR3 A and B) all mapping to chromosome 1.1 Some of these genes display functional allelic polymorphisms generating further molecular heterogeneity and interindividual differences in the effector properties of the receptors. FCGR2, the most widely expressed FcγR (found in most myeloid cells and in platelets), presents a single nucleotide polymorphism (SNP) resulting in either arginine (R) or histidine (H) at position 131 in the membrane-proximal Ig-like domain which affects receptor affinity for IgG immune complexes.2 Consequently, the most striking difference between the FCGR2A-131H and R alleles is in their affinity for human IgG2, and to a lesser degree for IgG1 and IgG3, which is higher for H alleles.3 A similar situation applies to the FcγRIIIA receptor expressed on macrophages and natural killer (NK) cells. An SNP resulting in either phenylalanine (F) or valine (V) at position 158 also affects binding to IgG; the FcγRIIIA-158V allele binds more avidly to IgG1, IgG3 and IgG4 subclasses.4 In addition, it has been reported that the FCGR3A polymorphism implies differences in receptor affinity and in levels of receptor expression.5
Rheumatoid arthritis (RA) is a multisystemic autoimmune disease characterised by synovial inflammation, the production of autoantibodies and joint destruction.6 Therapies targeting tumour necrosis factor (TNF)α (infliximab, adalimumab and etanercept), either as monotherapy or combined with methotrexate, have recently emerged as the most effective, achieving significant clinical, biological and functional improvement and halting or reducing joint destruction.7 Infliximab is a chimeric monoclonal antibody composed of a mouse Ig variable (V) region with anti-TNFα specificity and a human Ig constant (C) region of the IgG1 subclass. Among other mechanisms of action, infliximab promotes phagocytosis and ADCC following binding to membrane-bound TNFα. However, despite the proven therapeutic value of TNFα antagonists, around 25% of patients show low or no response.8 9 10
These less than optimal results may be due in part to the heterogeneity of the Fcγ receptors. Polymorphisms resulting in a higher affinity to the Fc region of TNFα antagonists may facilitate their clearance from the circulation and may therefore produce different therapeutic effects.
Two previous studies have evaluated this hypothesis by analysing the effects of the SNP of FCGR3A in the response to TNFα antagonists after 12 weeks of treatment, with controversial results.11 12 This study examines the influence of FCGR2A and FCGR3A polymorphisms on the clinical response to infliximab in patients with RA after 6 and 30 weeks of treatment.
Materials and methods
Patients
Patients diagnosed as having RA (according to American College of Rheumatology (ACR) criteria) and treated with infliximab between the years 2000 and 2005 at two hospitals (Hospital Clínic, Barcelona and Hospital Juan Canalejo, La Coruña, Spain) were included. The Ethics Committee of the Hospital Clínic approved the study and written informed consent was obtained from all participants.
All patients had established RA that was non-responsive to conventional disease-modifying antirheumatic drug (DMARD) therapy (methotrexate 12.5–25 mg/week). At inclusion and at weeks 6 and 30 of treatment, the number of tender and swollen joints, modified Health Assessment Questionnaire (HAQ), doctor’s and patient’s global assessment, erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) (mg/dl; determined by nephelometry) were recorded. Rheumatoid factor (RF) titres were determined by nephelometry (positive>20 IU/ml), and anti-citrullinated protein antibody (ACPA) titres were determined by second-generation ELISA (positive>50 IU/ml) (Immunoscan, Stockholm, Sweden) at baseline. Disease activity was evaluated by the 28-joint Disease Activity Score (DAS28) with three parameters including CRP (DAS28 3v-CRP). The efficacy of therapy after 6 and 30 weeks was classified according to 20%, 50% and 70% improvement as per the ACR criteria (ACR20, 50 and 70, respectively) and the DAS28 European League Against Rheumatism (EULAR) response criteria. The evolution of DAS28 3v-CRP during follow-up was also analysed.
All patients received infliximab (infusions of 3 mg/kg) at weeks 0, 2 and 6 and every 8 weeks thereafter. Dose and interval between infliximab remained unchanged throughout the study. A total of 83% of patients were taking prednisone (⩽5 mg/day), and all patients were taking methotrexate (range 12.5–25 mg/week) before and during treatment with infliximab.
FCGR2A and FCGR3A genotyping
Genomic DNA was purified from EDTA blood samples using the Qiagen DNA blood kit (Qiagen, Valencia, California, USA) following the manufacturer’s instructions. A previously reported allele-specific PCR method13 was used to genotype the biallelic functional polymorphism (V158F) of FCGR3A with some modifications.
The correct assignment of alleles was confirmed by nucleotide sequencing of three representative samples (VV, FV, FF) chosen at random.
The biallelic polymorphism of FCGR2A (H131R) was assessed using a PCR sequencing-based typing (PCR-SBT) method. Briefly, a 367 bp genomic DNA fragment was PCR-amplified by using the sense 5′-CTTTCAGAATGGCTGGTGCT-3′ and the antisense 5′-TTTGCTGCTATGGGCTTTCT-3′ primer pairs. The PCR reaction mix included 50–200 ng DNA, 10 pmol FCGR2A primers, 1 U Expand 20 kb plus Taq DNA polymerase (Roche Diagnostics GmbH, Mannheim, Germany), 0.5 mM deoxyribonucleotide triphosphates, diluted in Expand 20 kb plus buffer at a final volume of 20 μl. The cycling conditions were: 1 cycle of 94° for 5 min; 10 cycles of 94°C for 30 s; 65°C for 30 s and 72°C for 60 s; 25 cycles of 94°C for 30 s, 55°C for 30 s and 72°C for 60 s; and 1 cycle of 72°C for 7 min. From the resulting PCR reaction, 5 μl were treated with ExoSAP-IT (USB Corporation, Cleveland, Ohio, USA) and then subjected to direct sequencing with the BigDye Terminator V.1.1 Cycle Sequencing Kit (Applied Biosystems, Warrington, UK) following the manufacturer’s instructions with the sense gene-specific primer mentioned above. Sequencing reactions were analysed by capillary electrophoresis in an ABI PRISM 3100 Genetic DNA Analyser (Applied Biosystems).
Statistical analysis
The statistical analysis was performed using SPSS V.16.0 (SPSS, Chicago, Illinois, USA). A descriptive analysis of the patients was performed and the χ2 and Fisher exact tests were used to show differences in the outcome variables. Patients homozygous and heterozygous for high affinity alleles were grouped into a single category in order to perform a more robust χ2 2×2 comparison with patients homozygous for low affinity alleles. A comparison between patients with homozygous genotypes for the two genes and the remaining patients was also performed at 6 and 30 weeks. Additionally, DAS28 3v-CRP changes for the six genotypes were analysed by analysis of variance (ANOVA) according to the FCGR2A and FCGR3A genotypes at baseline, 6 and 30 weeks. Finally, we performed a generalised linear models multivariable analysis nested by patient and visit using DAS28 3v-CRP as the dependent variable and age, gender, RF, ACPA, disease duration, FCGR2A and FCGR3A genotypes as independent variables. Two-tailed p values less than 0.05 were considered significant according to the applicability criteria for the χ2 or Fisher exact test.
Results
A total of 91 patients with RA were included. The FCGR3A genotype could not be assessed in nine patients due to technical reasons. Some variables were not available for all patients and, therefore, the sample size changed accordingly for certain analyses.
Clinical and demographic data and the distribution of FCGR2A and FCGR3A genotypes, which was similar to that reported for other Caucasian populations,12 13 14 are shown in table 1.
Clinical and demographic patients data according to visit and genotypes
The ACR20, 50 and 70 responses and EULAR (DAS28 3v-CRP) responses at 6 and 30 weeks are shown in table 2.
American College of Rheumatology (ACR) and European League Against Rheumatism (EULAR) responses of patients with rheumatoid arthritis (RA) at weeks 6 and 30; patients are classified by low affinity and high affinity FCGR2A and FCGR3A genotypes
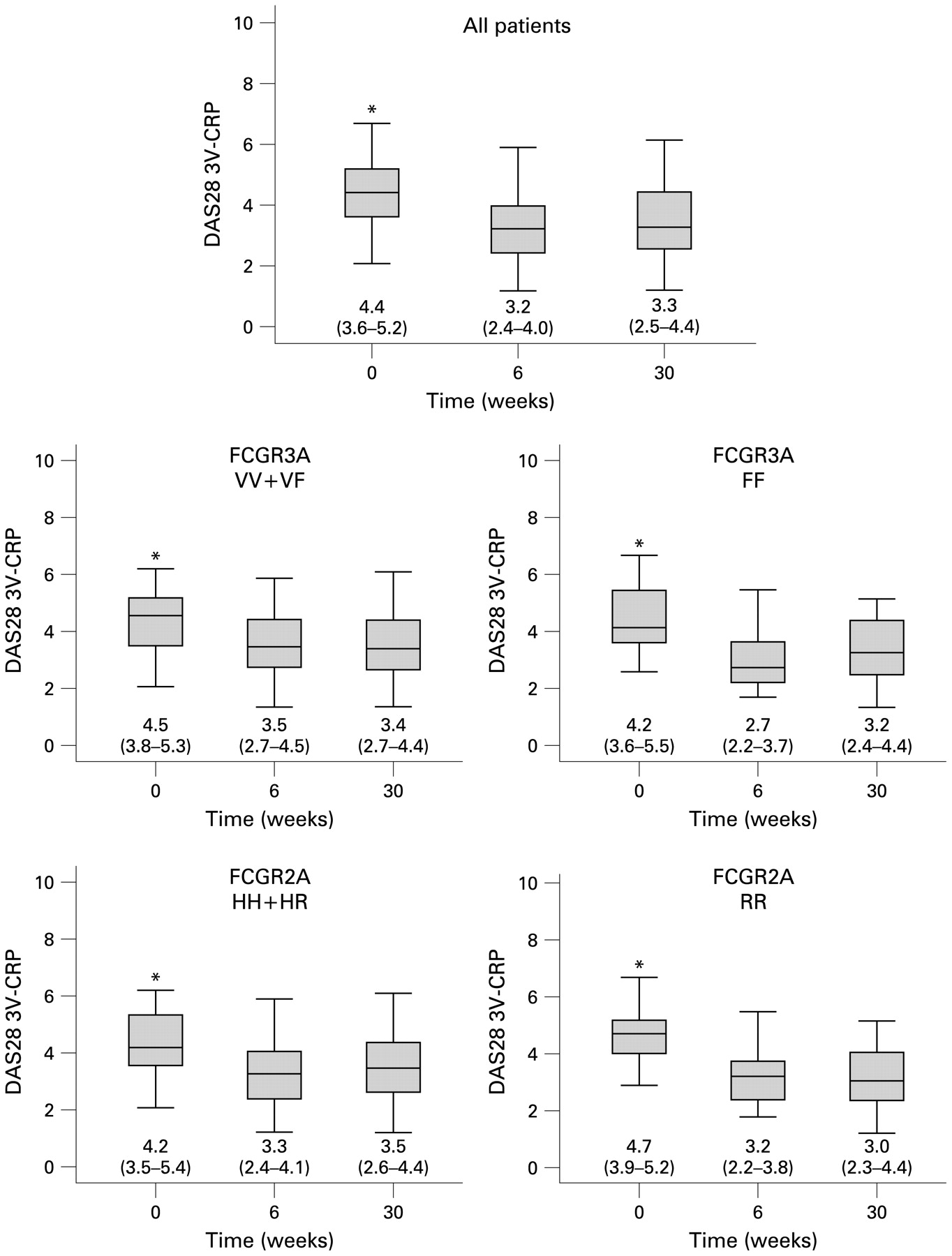
Significant results were found for low affinity FCGR3A-FF and FCGR2A-RR genotypes for ACR50 at week 6 and ACR20 at week 30, respectively. EULAR good response was also significantly higher at week 6 in patients homozygous for low affinity FCGR3A-FF genotypes. The statistical power for these outcomes was 71% (ACR50 at week 6 for FCGR3A), 46% (ACR20 at week 30 for FCGR2A) and 41% (EULAR good response at week 6 for FCGR3A), respectively. These results were consistent with the evolution of DAS28 3v-CRP during the follow-up, as it is described in fig 1.

{kind=link}
Evolution of values of 28-joint Disease Activity Score (DAS28) 3v-C-reactive protein (CRP) in all patients and according to FCGR2A and FCGR3A genotypes, separated by allele affinity. Data are presented as box-whisker plots, with median, 25th to 75th percentile and 5th to 95th percentile. *Significant differences (p<0.001) between baseline and follow-up visits.
Generalised linear model multivariable analysis nested by patient and visit using DAS28 3v-CRP as dependent variable showed that patients with the low affinity FCGR3A genotype had a significantly lower DAS28 3v-CRP at week 6 (p = 0.001), but interactions between FCGR2A and visits only showed a trend to significance (table 3).
Coefficients of multivariable generalised linear models analysis
Finally, we compared individuals with two low affinity genotypes (FCGR3A-FF and FCGR2A-RR) with those with other genotypes and found a trend to significance in the ACR20 response (78% vs 40%; Fisher exact test p = 0.069) and a greater reduction in DAS28 3v-CRP (ΔDAS28 2.10 (0.93) vs 1.06 (0.97), p = 0.003) at week 6.
Discussion
Our results indicate that FCGR2A and FCGR3A genotypes influence the clinical efficacy of infliximab according to ACR and EULAR response criteria and DAS28 3v-CRP changes at different timepoints during follow-up. Individuals homozygous for low affinity FCGR3A-FF have better ACR50 and EULAR good response at week 6, whereas individuals with low affinity FCGR2A-RR have better ACR20 responses at week 30 of infliximab treatment. These results probably reflect the complex, dynamic nature of the interaction between FcγR and Ig, and may shed some light on two previous conflicting reports.11 12 Tutuncu et al,11 in a study of 30 patients with RA, found that patients with the FCGR3A-FF genotype had a better response to several TNFα antagonists after 12 weeks than those carrying at least 1 FCGR3A-V allele. In contrast, Kastbom et al12 evaluated 282 patients with RA after 12 weeks of anti-TNFα treatment and found no influence of the FCGR3A genotype on the clinical response.
We included 91 Spanish patients with RA treated with infliximab due to persistent disease activity in spite of methotrexate therapy. Although with lower statistical power than the study by Kastbom et al,12 our study evaluated therapeutic responses after 6 and 30 weeks according to the FCGR2A and FCGR3A polymorphisms.
The ACR responses of the entire group at 6 and 30 weeks were lower than those observed in clinical trials,8 9 10 probably because this group of patients had long disease duration and had already failed several DMARD therapies. Interestingly, we found significant differences between individuals with FCGR3A-FF and compound VV-VF for ACR50 response at week 6, indicating that patients homozygous for low affinity variants (FF) have better clinical responses. Furthermore, reduced FCGR3A surface expression in individuals who were homozygous FF compared to individuals carrying at least one valine allele (FV or VV) has recently been reported.5 These findings suggest that patients with FCGR3A-FF clear infliximab less efficiently from the circulation, thus increasing its beneficial clinical effect.
Significant differences between low affinity individuals with FCGR2A-RR and individuals with compound RH-HH for the ACR20 response at week 30 were also observed. To our knowledge, there are no previous studies on the influence of FCGR2A variants on the response to TNFα antagonists in RA. The FCGR2A-H allele is known to interact effectively with human IgG2 but binds to human IgG1 with a lower affinity.3 15 Interestingly, the FCGR2A-RR genotype is a risk factor for susceptibility to some infections and autoimmune diseases.1 This is because immune complexes are removed less efficiently from the circulation in individuals with FCGR2A-RR, which might cause tissue injury. The significantly better ACR20 response observed at week 30 in patients with FCGR2A-RR suggests that these individuals may probably clear infliximab less efficiently than patients carrying high affinity variants (HH or RH).
Patients homozygous for low affinity FCGR3A-FF alleles also had a better EULAR good response at week 6 than patients with VV-VF, reinforcing the ACR50 response results. By contrast, patients with low affinity FCGR2A-RR alleles only showed a trend to significance in EULAR good and moderate responses at week 30. This is not unexpected, since a poor concordance between ACR and EULAR response criteria in patients with long-standing established RA treated with biological agents has been reported.16
The results for ACR20, ACR50 and EULAR good responses are supported by changes in the continuous variable DAS28 3v-CRP during the study. In addition, linear models multivariable analysis showed an association between low affinity FCGR2A-RR and FCGR3A-FF genotypes and DAS28 3v-CRP reduction throughout the study.
Taken together, the reported data support the influence of variants of different FcγR (FCGR2A and FCGR3A) on the clinical efficacy of Ig-like therapies (infliximab) in patients with RA. This probably reflects differences in the binding capabilities for human IgG1 and/or expression levels of FCGR2A and FCGR3A variants. However, this influence is complex and dynamic and requires proper evaluation at different timepoints during the follow-up.
Acknowledgments
The authors thank Loreto Carmona (Unidad de Investigación de la SER, Madrid) and Miguel Sampayo (Salutis Research, Barcelona) for their advice on statistical methods.
REFERENCES
Footnotes
Funding This work was supported by Fondo de Investigación Sanitaria (JDC: PI04/1023, PI041027). JDC was also supported by a research grant from Fundación Española de Reumatología (programa DIB/SER). FLS was supported by a grant from the Spanish Research Network on Infectious Diseases (REIPI, RD06/0008/1013) from Instituto de Salud Carlos III.
Competing interests None.
Ethics approval The Ethics Committee of the Hospital Clínic approved the study and written informed consent was obtained from all participants.