Article Text

Abstract
Objective To assess in a multicentre randomised double-blind phase III clinical trial evaluating the effect of licofelone in comparison with naproxen on knee osteoarthritis (OA) the presence of, and change in, bone marrow lesions (BML) over time, their relationship to cartilage volume loss, meniscal extrusion and pain.
Methods Patients with knee OA were selected from the dataset of a recently published randomised controlled trial. MRI was performed at baseline, 6, 12 and 24 months to assess BML score (modified Whole-Organ MRI Score) and cartilage volume changes over time. Pain levels were assessed using the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) questionnaire.
Results One hundred and sixty-one patients completed the study according to protocol. The global knee and all subregions showed increased BML scores over time (p <0.001, 24 months) except for the medial tibial plateau in the licofelone group. In multivariate regression analysis, licofelone treatment predicted reduction in BML score in the medial tibial plateau (β= −0.280, p = 0.026). BML scores at baseline correlated with cartilage volume over time; however, correlation was limited to 12 months. No positive correlation was found between BML and WOMAC scores.
Conclusions BML scores were found to increase over time, probably owing to accumulation of chronic structural changes. Correlation between BML and cartilage volume was strong at baseline but not over time, probably due to the study drug. Licofelone reduced the BML score in the medial tibial plateau. In contrast to previous reports, no positive relationship was found between BML score (baseline or change over time) and pain, probably an effect of the selected population.
Statistics from Altmetric.com
Introduction
With increasing use of MRI in the assessment of knee osteoarthritis (OA), it has become apparent that the subchondral bone is frequently the site of signal alterations, indicating lesions. These lesions were first thought to be bone marrow oedema, as they showed as hypersignals in water-sensitive T2-weighted sequences, which were considered to reveal oedema.1 The loading in the respective part of the knee is hypothetically considered a causative factor for bone marrow lesions (BML),2 supported by the histopathologically depicted microfractures in BML and findings in malaligned knees: BML presented predominantly laterally in valgus lower limbs and medially in varus limbs.3 Meniscal derangement has also recently been associated with the presence of BML.4
Several studies comparing BML with histopathology presented a great variety of morphological changes—namely, hypervascularity cellular infiltration, bone marrow bleeding and fibromyxomatous transformation of the bone marrow, as well as trabecular alterations including microfractures5,–,9; a real oedema was a minor and less common finding.6 7 9 Therefore, the term used earlier, bone marrow oedema, implying a histopathological diagnosis, has been replaced by the more descriptive term, BML.10,–,12 Some of these findings, such as oedema, bleeding and microfractures, are more acute and similar to findings radiographically resembling traumatic bone bruises.13 14 While bone bruises tend to disappear within several months in the healing process,15 BML in OA tend to persist and increase in size.16,–,20
In spite of these increasing insights into the real nature of BML, knowledge of the causative factors, as well as the correlation with pain, is still limited. While some authors found a distinctive correlation between BML and pain,12 21 22 others did not.17 19 23 24 BML were also found in painless knees without radiographic signs of OA.25 These conflicting findings probably reflect a lack of complete knowledge about the nature of the lesions, as different changes may look alike in MR images, as mentioned earlier. Moreover, the effect of concurrent treatment has not always been examined in the same thorough manner and might therefore be a relevant often neglected confounding factor in assessing the correlation between BML and pain. Results of a prospective controlled clinical trial, such as provided by this study, to our knowledge have not been previously published.
BML and cartilage loss have been linked in different studies. While the presence of lesions was shown to be associated with cartilage loss,3 16 26 the absence of lesions correlated with absence of cartilage disease progression.27 Patients with BML even seem to be at increased risk for total knee replacement.28 Whether the lesions are causative for cartilage loss or only a consequence is not yet known. Furthermore, there is a lack of information about effects of medication on BML and whether it might have an impact on the progression of cartilage defects. One cross-sectional study in knee OA reported that treatment with antiresorptive drugs combined with oestrogens could decrease the prevalence of BML,29 although there was no prospective controlled trial to confirm these findings. Already published results from this dataset provided important information about the disease-modifying OA drug (DMOAD) effect of licofelone on cartilage volume loss in comparison with treatment with naproxen. Whether it was effective through its influence on BML will be further examined in this article. This is the first randomised controlled trial to examine the effect of DMOAD treatment on BML and the relationship of these BML to cartilage volume loss and pain.
Patients and methods
This study is part of a recently published multicentre study of patients with knee OA comparing the effect on cartilage loss of oral treatment with licofelone, a lipoxygenase/cyclo-oxygenase inhibitor, with naproxen.30 It deals with one of the end points of the original study, specifically the BML. Briefly, patients with primary symptomatic knee OA of the medial femorotibial compartment, diagnosed according to criteria of the American College of Rheumatology,31 were recruited from outpatient rheumatology clinics. Patients included in the study had a pain level of no less than 40 mm on the visual analogue scale, radiographic OA grade 2–3 on the Kellgren–Lawrence scale and at least one of the following three risk factors for increased risk of radiographic progression: body mass index (BMI) >30, presence of Heberden's nodes, or female gender. The study was approved by the local ethics committees and all patients gave their oral and written informed consent to participate.
Subjects were randomly assigned to receive either therapeutic dosages of licofelone (200 mg twice daily) or naproxen (500 mg twice daily) for 2 years. MRI was performed at baseline, 6, 12 and 24 months. High-resolution, 3D MRI was obtained using a commercially available 1.5 T with integrated knee coil. Two sequences were used: 3D spoiled gradient recalled acquisitions with fat suppression (General Electric, Milwaukee, Wisconsin, USA) and optimised 3D fast imaging at steady-state precession (FISP) acquisitions with water excitation (Siemens, Erlangen, Germany), as previously described.32,–,34 The subchondral BML were assessed at baseline, 6, 12 and 24 months using a semiquantitative scoring system as previously described,35 with some adjustments. Briefly, the joint was divided into its anatomical regions (medial and lateral condyle, medial and lateral tibial plateau and patella), which were subdivided into anterior, central and posterior for the femur and medial and lateral for the patella and the tibial plateaus. Subchondral bone marrow abnormalities were then assessed comparing the surface of the lesion with the surface of the subregion in the corresponding image. If the lesion was depicted in multiple slides, the one with the largest extent was chosen. When the maximal extent of the lesion was oriented along the lateromedial direction, a reconstructed axial image was used for the evaluation. A scale from 0 to 3 was used, where 0=absence, 1=<25%, 2=25–50% and 3=>50% of this ratio. This method differs from the underlying Whole-Organ MRI Score system35 in only minor points as it does not include the subspinal section between the two tibial plateaus or subdivide the tibial plateaus.
The central and posterior femoral subregions and the tibial plateau formed the medial and lateral compartments. The medial and lateral anterior femoral subregions and the two patellar subregions formed the femoropatellar compartment. All three compartments combined resulted in the global value. The maximal possible scores were 9 for the medial and lateral compartment and 12 for the femoropatellar compartment. The maximal global value was 30. The inter-reader reliability in BML scoring has previously been shown to be excellent.36
Knee joint cartilage volume was measured by two expert readers using a specially developed computer program (Cartiscope, ArthroVision, Montreal, Quebec, Canada).33 The change in knee cartilage volume over time was obtained by subtracting the follow-up volume from the initial (baseline) volume. The change in cartilage volume over time was calculated for each of the medial and lateral compartments of the knee. For the femoropatellar compartment, only the anterior trochlear segments of the condyles were used. The reproducibility of the method has previously been demonstrated to be excellent.33
The extent of meniscal extrusion on the medial and lateral edges of the femorotibial joint space was evaluated at baseline as previously reported26 37 for the anterior, middle and posterior horns of the menisci, in which 0 = no extrusion, 1 = partial extrusion and 2 = complete extrusion with no contact with the joint space (severe).
Further, patients underwent clinical evaluation at baseline, 6, 12 and 24 months based on the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) pain questionnaire.38 There was a 24 h washout of rescue analgesic medication before each clinical evaluation and a 7-day washout of non-steroidal anti-inflammatory drugs (NSAIDs) before baseline evaluation.
Between treatment groups, variable changes at all time points were assessed using two-sample Student t tests. All tests were two-sided and a p value ≤0.05 was considered statistically significant but was not adjusted for multiple testing. Predictive factors for BML changes were assessed using different univariate and multivariate regression analyses. For correlation between two continuous variables, Pearson coefficient analysis was used. All statistical analyses were performed using SAS software, version 9.1 (SAS Institute, Cary, North Carolina, USA).
Results
Of the 355 patients originally enrolled, 161 completed the study according to protocol (ATP), 82 in the licofelone group and 79 in the naproxen group. Patients in the ATP group at study entry had similar mean age, gender, height, weight, BMI, WOMAC pain score, cartilage volume and BML score except for a difference between BML in the medial compartment close to significance (p = 0.053) (tables 1 and 2). BMI remained equally distributed at 24 months (p = 0.646) and did not increase compared with baseline (p = 0.653). Acetaminophen as rescue analgesic medication was used in both groups in similar distribution (licofelone 65%, naproxen 67%; p=0.743). Not all of the 161 patients had completed all four MRI readings. The number of MRI readings assessed in the licofelone and naproxen groups, respectively, were 82/79 at baseline, 81/79 at 6 months, 80/79 at 12 months and 70/73 at 24 months.
Baseline demographic, clinical and imaging characteristics
Baseline and change in bone marrow lesion score over time according to treatment
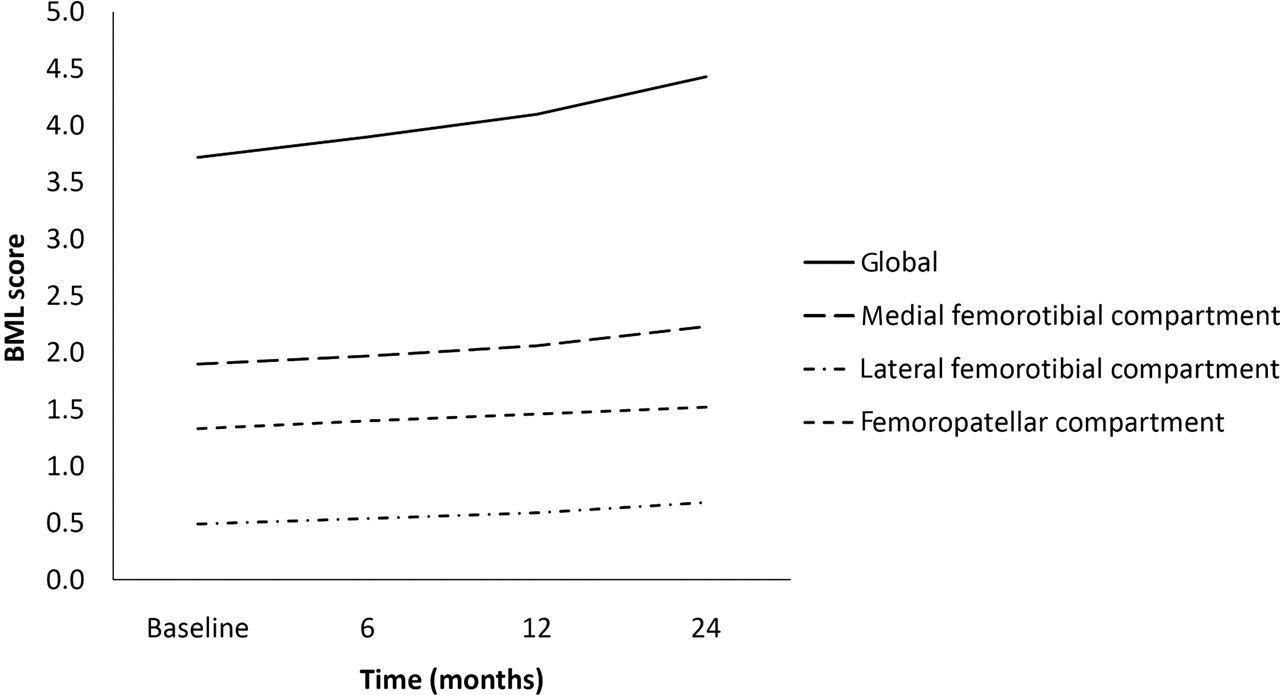
During the study's timeframe of 24 months, the BML scores similarly and significantly increased in size globally and in all three compartments (figure 1, table 2).The changes in the values for the lateral femorotibial and patellofemoral compartments not shown in the table were, at 6 months (mean ± SD (p value)) 0.05 ± 0.31 (0.045), 0.10 ± 0.69 (0.070); at 12 months 0.09 ± 0.47 (0.013), 0.16 ± 0.66 (0.002); and at 24 months 0.19 ± 0.75 (0.003), 0.19 ± 0.86 (0.009), respectively.There was no significant difference in the compartments and subregions between the two treatment groups, except for the medial tibial plateau. While the BML progressed in this subregion in the naproxen group, progression stopped or even slightly decreased in the licofelone group. The non-significant values for the remaining subregions are not shown.
{kind=link}
Bone marrow lesion (BML) score over time in patients having completed all four MRI sets (n=143).
A multivariate linear regression analysis (table 3) was carried out to detect predictive factors for the change in BML, including the variables age, sex, BMI, WOMAC pain, treatment, severe meniscal extrusion and cartilage volume loss. Data showed a negative correlation between BML score change in the medial tibial plateau and licofelone treatment (β = −0.280, p = 0.026).
Regression analyses to predict change in bone marrow lesions at 2 years (n=143)
Regarding the cartilage volume and the BML (table 4), at baseline a significant negative correlation was found between cartilage volume and BML score in the medial femorotibial (r= −0.242; p=0.002), lateral femorotibial (r = −0.284; p <0.001) and in the femoropatellar compartment (r = −0.283; p<0.001). At 12 months, in the global (r = −0.176; p=0.026) and in the medial femorotibial compartment (r = −0.185; p=0.019) a significant correlation between the increasing BML score and cartilage volume loss was found. However, no correlation was found at 6 and 24 months. There were similar and significant improvements in WOMAC pain scores at 6, 12 and 24 months for both treatment groups compared with baseline (p <0.001), but there was no significant difference between groups (data previously reported30). Neither at baseline nor during the course of the study were any significant correlations found between BML baseline/BML change and WOMAC pain for the medial and lateral femorotibial compartments (table 4). In the femoropatellar compartment, there was a significant inverse correlation between change in BML and WOMAC pain scores at 6 (r = −0.216; p=0.006) and 12 months (r = −0.239; p = 0.002), with a negative trend at 24 months (r = −0.154; p = 0.067). WOMAC pain scores at baseline were not predictive of BML score (p = 0.937) or cartilage volume loss (p = 0.742) at 24 months.
Correlation between baseline and changes in BML scores and cartilage volume, baseline and changes in BML and WOMAC pain scores
Discussion
This study provides new and unique information about the relationship between the structural changes and pain in patients with knee OA who were continuously treated in a randomised controlled trial for a period of 24 months with either licofelone, a combined 5-lipoxygenase and cyclo-oxygenase inhibitor, or naproxen, one of the most commonly prescribed NSAIDs for the treatment of OA.
This study demonstrated as the main finding a progressive increase in BML score in all compartments of the knee joint over time in both treatment groups, which confirms the predominant findings of BML size increase in several other studies.16,–,20 The increased BML size probably reflects an accumulation of fibromyxomatous tissue in subchondral bone replacing different types of preceding histopathological alterations such as oedema, microfractures, bleeding and hypervascular repairing processes as seen in previous reports comparing MRI with histopathology.5,–,9 More acute changes such as microfractures and oedema, which are depicted similarly in traumatic bone bruises,13 14 however, tend to vanish over time during the healing process.15
One of the unique findings of the study was the demonstration that in the patients treated with licofelone the BML progression in the medial tibial plateau remained stable or even decreased in comparison with a steady increase in the naproxen-treated group. This difference between the two treatment groups was found to be statistically significant and a regression analysis identified licofelone as a negative predictive factor for BML progression in the medial tibial plateau. These findings could reflect a reversible change positively influenced by the treatment with licofelone. Licofelone was shown to reduce in the subchondral bone the number of osteoclasts containing cathepsin K and matrix metalloproteinase-13 and reduce the loss of subchondral bone volume in experimental dog OA.39 Licofelone also prevents the abnormal metabolism of osteoblasts, in vitro, in human OA subchondral bone.40 The possible advantage of licofelone over naproxen may lie in its ability to block both the leukotriene and cyclo-oxygenase pathways, preventing shunting between them.41 These characteristics of licofelone may have caused the above-mentioned findings; however, these explanations remain hypothetical.
There are clues that BML may precede changes in cartilage morphology42 and may also predict or be linked to the progression of structural changes in knee OA.3 20 28 43 Our findings documented a significant negative correlation between BML score and cartilage volume in all three compartments at baseline. Although for both BML score and cartilage volume loss progression occurred over time, no linear correlation between these two structural changes was seen. Among other factors, this may be a result of the use of a semiquantitative assessment of the BML, which might not have depicted the full extent of the lesions, as further discussed below.
Regarding the treatment effect, the findings of the original study showed in the ATP population a significant protective effect of licofelone on cartilage volume loss both globally and in the lateral compartment, with a trend in the medial compartment. However, in the intention-to-treat (ITT) population, this protective effect was significant in the medial compartment also, whereas the effect on BML was present in the medial tibial plateau only. These findings may reflect the fact that the protective effect of licofelone on cartilage loss is not based on its effect on BML but rather on its direct effect on cartilage.
A number of reports have demonstrated a distinctive correlation between BML size and pain12 21 22; however, the findings of our study did not confirm this. A lack of correlation between the two has also been reported by others.17 23 24 BML can even be found in painless knees.19 25 44 As previously mentioned, different histopathological changes can be depicted similarly in MR images.5,–,9 13 14 Therefore, the discrepancies between the results of these studies may be related to the fact that they might have dealt with different morphological changes. For example, oedema and microfractures, as in bone bruises, can easily be imagined to be painful, while fibrotic changes would be rather painless. In addition, we believe that the contribution to the pain level by BML in patients was probably influenced by NSAID treatment during the follow-up visits, as there was a 24 h washout only for rescue analgesic treatment before each visit and NSAIDs were taken throughout the follow-up assessments. Additionally, according to the inclusion criteria, a minimal pain level of 40 on the visual analogue scale was mandatory, excluding painless patients who might have presented BML. This is a limitation that should be taken into consideration in the context of any trial dealing with pain in which analgesics/NSAIDs are part of the treatment.
This report has some obvious limitations. We purposely elected, in this post hoc analysis, to analyse only those patients who completed the study while taking all the study drug (licofelone or naproxen). We felt this was critical to assess biomarkers that may be rapidly susceptible to change and to ensure data consistency. Although we did not analyse the whole ITT cohort (355 patients), the baseline characteristics of the patients analysed in the ATP cohort were similar to those of the entire ITT cohort. We recognise however, that the randomisation process was designed for the original primary end point, cartilage loss, in the ITT population. As we used the ATP population (who completed all four MRIs), the randomisation process was not optimal for the distribution of the BML between the two groups. In addition, owing to the post hoc design and the exploratory character of this study, there was a risk of finding significant values through multiple testing. This is further underlined by the findings of relatively small r and R2 values. Furthermore, subchondral bone signal abnormalities were identified using FISP and gradient echo sequences designed for optimal depiction of cartilage.45,–,48 It is known that these sequences do not depict BML to as great an extent as T2-weighted sequences. Data from an internal revision process using a dataset including T2-weighted sequences and reports of our earlier findings on BML using FISP sequences show, however, that the ratio of change in BML size in human OA remains the same for either the sequences used in this study or T2-weighted sequences that were not added to the protocol in order to keep the duration of an MRI session as short as possible.36 49 Therefore, we do not believe that the choice of sequences confounded our final results.
Another limitation is the absence of a placebo arm that would have allowed exclusion of a possibly deleterious effect of NSAIDs on subchondral bone; however, for such a lengthy study of a painful condition, it would have been unethical to treat patients with a placebo. Furthermore, the number of participants was limited which may have weakened the meaningfulness of the results. In a slowly progressing disease such as OA, a longer follow-up period would also have been desirable.
In conclusion, this report shows that in knee OA, BML scores increase globally and in most of the subregions over time, probably reflecting an accumulation of fibromyxomatous tissue. The DMOAD effect of licofelone on cartilage is not mediated by its effect on subchondral bone alterations. In contrast to previous reports, the relationship between BML at baseline and BML changes over time, to pain level and its changes over time, could not be documented in this study. Interference with the study drug and the selected population may provide some explanation for the latter findings and should be taken into account for further similar trials.
Acknowledgments
The authors thank Virginia Wallis for her assistance with the manuscript preparation.
References
Footnotes
-
Funding This study was supported in part by grants from Merckle GmbH (Ulm, Germany) and ArthroLab (Montreal, Quebec, Canada).
-
Competing interests LMW received a grant from the Swiss National Science Foundation. JPR is a consultant for ArthroVision. MD is a consultant for ArthroLab. JMP and JPP are consultants for and shareholders in, ArthroLab and ArthroVision. FA is an employee of ArthroVision Inc.
-
Ethics approval Approved by the local ethics committees.
-
Provenance and peer review Not commissioned; externally peer reviewed.