Article Text

Abstract
Background The onset of disease in ankylosing spondylitis (AS) is generally earlier than in other joint diseases, exposing patients to a prolonged burden of disease. Whether this is associated with excess mortality is still uncertain. Radiation therapy for AS has previously been shown to increase mortality. The present study investigated standardised mortality ratios, causes of death and survival predictors in a large regional cohort of patients with AS.
Method A total of 677 patients with AS followed at our hospital since 1977 were matched by gender, age and postal area to three controls from the general population and standardised mortality rates (SMRs) were calculated. Cause of death was established using patients' hospital records. In a subset of 360 patients, clinical and demographic data collected during an earlier research visit (1998–2000) were used in a prospective multivariate analysis of predictors for mortality in AS.
Results The crude mortality among patients with AS in this study was 14.5% (98 patients); SMR was only significantly increased among male patients compared with female patients (1.63 vs 1.38, p<0.001). Circulatory disease was the most frequent cause of death (40.0%), followed by malignant (26.8%) and infectious (23.2%) diseases. Factors independently associated with reduced survival were diagnostic delay (OR 1.05), increasing levels of C-reactive protein (OR 2.68), work disability (OR 3.65) and not using any non-steroidal anti-inflammatory drugs (OR 4.35).
Conclusions Mortality is increased in patients with AS and circulatory disease is the most frequent cause of death. Parameters reflecting the duration and intensity of inflammation are associated with reduced survival. These results indicate that, to improve long-term survival in AS, there is a need for early detection and anti-inflammatory treatment as well as a vigilant approach for cardiovascular risk factors.
Statistics from Altmetric.com
Introduction
Ankylosing spondylitis (AS) is a chronic inflammatory disease affecting primarily the sacroiliac (SI) joints and spine. An increased mortality in patients with AS was first observed following irradiation treatment in the 1950s.1 Subsequently, increased mortality was also documented in patients with AS not exposed to therapeutic irradiation, indicating that disease-specific factors may contribute to early death.2,–,5 Death as a direct consequence of AS such as spinal fractures and cervical subluxations has been reported,6 but AS is not infrequently accompanied by serious extraspinal complications such as aortitis, atrioventricular conduction disorders, pulmonary fibrosis and amyloidosis.7 With the onset of disease usually in the third decade of life, the potential for comorbidity development is present for several decades.8 While malignant diseases occurred more frequently in patients with AS who received radiation therapy, circulatory diseases have been identified as a significant cause of mortality in AS in cohort studies.3 5 Also, an increase in alcohol-related deaths in AS has been observed in a selected group of non-surviving patients with AS in Finland.4 Given the limited amount of data on AS mortality in the literature and the fact that most of these studies were based on retrospectively collected data from the middle of the last century, it has been difficult to identify the risk factors associated with premature death in AS. In this study we present data on standardised mortality, long-term survival, cause of death and prospectively collected risk factors for premature death in a large cohort of patients with AS.
Methods
The AS cohort in this study has been described in detail previously.9 In brief, it includes all patients fulfilling the modified New York criteria for AS10 seen in this region over the last three decades. The year of onset of symptoms consistent with AS was considered as the time of onset of the disease, and the time of diagnosis as the time of definite radiographic changes in the SI joints. For this analysis, each patient was assigned three controls from the general population who were matched for gender, age and postal area of residence. Thus, if the patient experienced his or her first symptoms at the age of 25 years in 1980, three controls would be selected, matched for age, gender and area of residence, and followed retrospectively from 1980 onwards. The follow-up period was defined as the time from symptom onset to 1 May 2009 or until the date of death. The assignment of cause of death was based on data obtained from patients' records. For patients who died during or shortly after a hospital stay for a documented condition, the cause of death was considered ascertained. Our standard approach is that patients with AS are seen once every year (or more frequently when clinically indicated) and the existing data in the patient's records gave us a fairly reliable indication of the most likely contributory cause of death for patients dying ≥3 months after the last contact with the hospital. We also registered patients' reported frequency of non-steroidal anti-inflammatory drug (NSAID) use (daily, weekly, monthly or less frequently).
A subset of 360 patients in this cohort had been evaluated in a separate study designed to evaluate functional outcome of AS.8 With a follow-up period since then of nearly 10 years, we were able to perform a prospective analysis of potential risk factors for increased mortality in this subset of patients with AS.
Data were analysed using SPSS Version 16.0. The data indicate mean/median values unless otherwise specified, and group comparisons were done by non-parametric techniques (χ2 test or Mann–Whitney test). Standardised mortality rates (SMRs) were based on observed numbers of deaths in the AS group (n=677) and the control group (n=2031) and further specified by age and gender. Survival curves were based on Kaplan–Meier estimates and compared using a log rank test (Mantel–Cox). Risk factors for early mortality in the prospectively followed subset of patients with AS (n=360) included selection of variables that yielded a significance level above 0.2 in the univariate approach and subsequent inclusion in logistic regression analyses. The multivariate regression analyses were performed using a stepwise method after controlling for multicollinearity.
Results
Descriptors
The AS cohort (n=677) showed a male preponderance with 511 men and 166 women (ratio 3.1:1) and mean (SD) age at onset of symptoms of 23.2 (8.5) years. The mean delay in diagnosis was 9.0 years (median 7.0 years) and the mean (SD) follow-up period since onset of AS was 31.9 (11.3) years. There were no significant gender differences regarding age at onset, diagnostic delay or follow-up time (data not shown). None of the patients had received radiotherapy treatment for AS.
By the end of the follow-up period 98 patients had died, yielding a crude mortality of 14.5%. In non-survivors (89 men and 9 women) the mean age at last follow-up was significantly higher than for survivors (62.8 vs 54.9 years, p<0.001), as was the male-to-female ratio (9.9:1), although age at onset was not retained in a multivariate analysis. Male non-survivors were significantly older at the time of symptom onset than both female non-survivors (28.5 vs 23.3 years; p=0.002) and male survivors (28.5 vs 22.4; p<0.001), and the diagnostic delay was significantly longer (11.2 vs 8.3 years; p=0.012) than among male survivors. When the importance of diagnostic delay in the entire patient population was considered, there was an increased risk of premature death if diagnostic delay exceeded 12 years (OR 1.65, 95% CI 1.05 to 2.58). However, we found no evidence of a ‘birth cohort’ effect or an overall effect of age at disease onset (see tables S1 and S2 in online supplement).
Mortality
The SMR for the whole cohort was 1.61 (95% C.I. 1.29 to 1.93; table 1). The SMR differed for female and male patients (1.38 vs 1.63, p<0.001) and, while this increased mortality was not statistically significant among female patients, there was a significant increase in SMR for male patients. To determine whether there was any influence of the development in healthcare over time, we also investigated whether changes in SMR had occurred over the last four decades. Based on the year of onset of AS, there was a gradual decrease in SMR for female patients while SMR in male patients showed a trend to increase that bordered on statistical significance (table 1).
Standardised mortality rate (SMR) and 95% CI in ankylosing spondylitis specified by time of symptom onset
Cause of death
A cause of death could be obtained in 82 cases (84%, table 2). In 62 patients the direct cause of death was ascertained and in 20 patients there were clear contributory causes to their sudden death. Among these patients, coronary heart disease was the most frequent condition (n=11) followed by valvular disease/thoracic aortic aneurysm (n=3), chronic renal failure (n=1), cardiomyopathy (n=1), apoplexia cerebri (n=1), atrioventricular (AV) conduction deficit (n=1), pseudomembranous colitis (n=1) and chronic alcoholism (n=1). Based on these estimates, circulatory disease (cardiovascular disease (CVD), valvular disease/thoracic aneurysms, AV conduction disease and cardiomyopathy) was the most frequent cause of death (40%), followed by malignant disease (27%) and infectious disease (23%). The group with other causes of death included patients dying from trauma (n=2), chronic renal failure (n=1), paracetamol intoxication (n=1), ventricular ulcer (n=1), degenerative neurological disease/cerebellar ataxia (n=1), cor pulmonale secondary to chronic pulmonary embolism (n=1) and chronic alcoholism (n=1). Two patients who died from cardiomyopathy and renal failure, respectively, had a recognised condition of amyloidosis.
Causes of death in ankylosing spondylitis
Survival
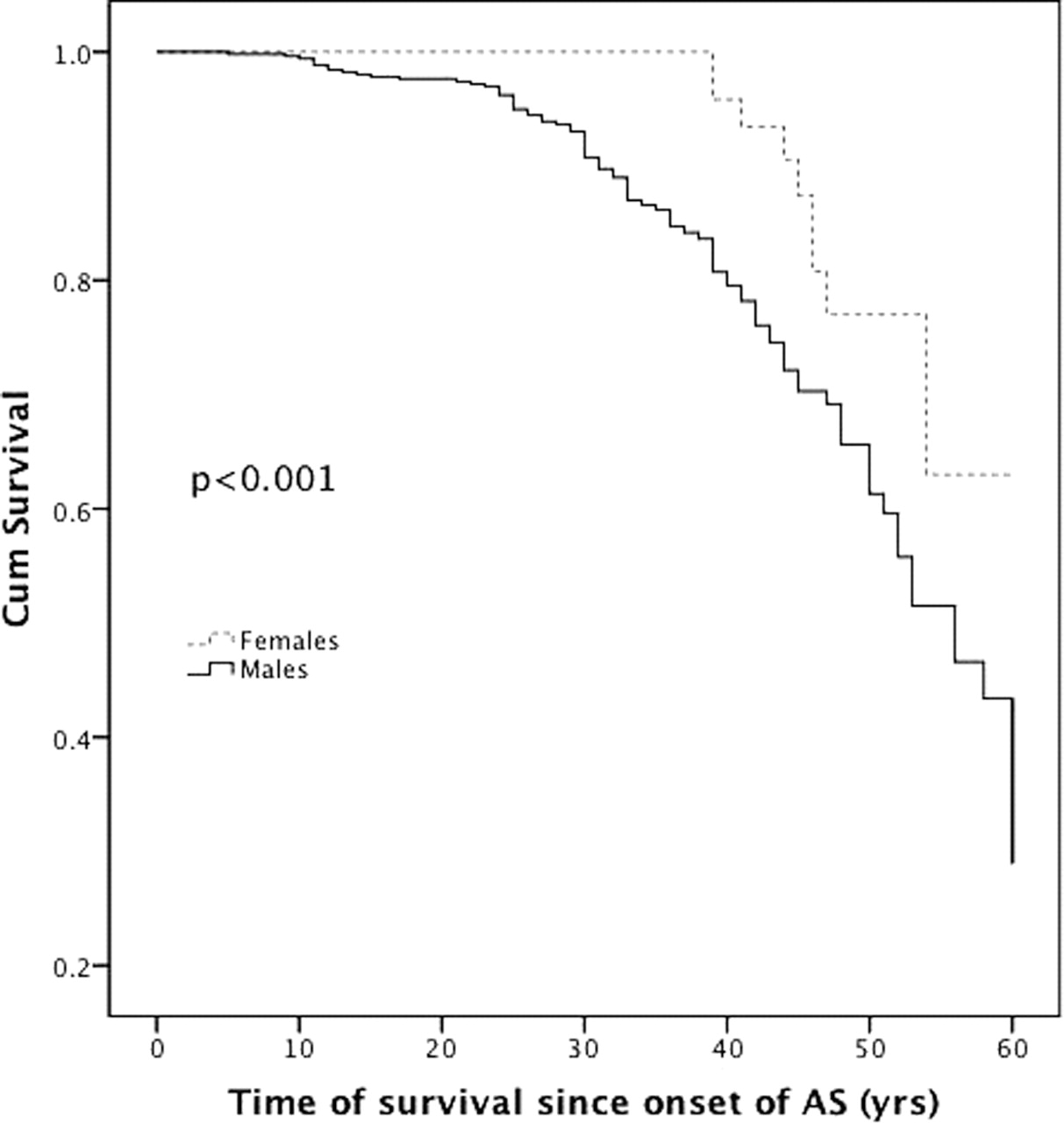
Overall survival assessed by Mantel–Cox analyses was significantly decreased in patients with AS compared with controls (χ2=48.75, p<0.0001; figure 1). The estimated 10, 20, 30, 40 and 50 year survival rates were 100%, 98%, 93%, 84% and 67%. Gender clearly influenced survival with no fatalities among women during the first 38 years of disease (figure 2); gender-specific survival after 50 years was 61% and 77% for men and women, respectively.

Kaplan–Meier survival curve of men with ankylosing spondylitis (AS) and controls matched for age, gender and area of residency, showing increased mortality among patients with AS.

{kind=link}
{kind=link}
Survival curves in patients with ankylosing spondylitis (AS) by gender.
Risk factors predicting increased mortality
In the subset of 360 patients who had previously been evaluated at our outpatient clinic and thus could be studied prospectively, 28 patients had died by the end of the follow-up period. A number of clinical and demographic variables were significantly associated with mortality in the univariate analyses (table 3). In the multivariate analyses, after correcting for age (β=0.013, p=0.6), gender (β=0.76, p=0.2), disease duration (β<0.01, p=0.99) and pre-existing CVD (β=1.05, p=0.1), we found increasing levels of C-reactive protein (CRP), diagnostic delay, not using any NSAIDs and work disability to be independent predictors for increased mortality (table 4).
Univariate analyses of the association with reduced survival of various variables expressed by level of significance
Variables independently associated with increased mortality in ankylosing spondylitis
Discussion
In this study we have evaluated mortality in a population of 677 patients with AS, making it one of the largest studies of AS mortality in recent years.6 We found the mortality to be increased in men with AS (SMR 1.63) while there was no significant increase in women with AS. There was a non-significant trend towards increased mortality in women after disease duration of 35–40 years. It could well be that a larger study population and, additionally, a longer time span of observation is necessary to demonstrate excess mortality in women with AS as the longer life expectancy in women of any population would also dilute an increased mortality if the duration of the observational period is inadequate. The gender difference was not retained in the multivariate analyses and the reason for this gender difference is unclear, but a similar increased mortality among male patients has also been reported in rheumatoid arthritis.11 However, overall mortality in patients with AS was 1.61 (SMR), which is still a substantial increase in patients never exposed to irradiation compared with previous reports.12 In a previous study9 we were unable to demonstrate an increase in mortality in AS using the expected number of deaths obtained from age-grouped data from the general population as the comparator. The current observations are more reliable as they are based on individual and extended matching between patients and controls and benefit from prolonged follow-up.
Several groups have reported the increased risk of CVD in different rheumatic conditions.13,–,15 Circulatory disease was the most prevalent cause of death in this population, accounting for 27.5% of deaths (N=27) and, if we included cardiomyopathy, valvular disease and conduction disorders (N=6), this increased to 33.7% of all deaths and 40.2% if unknown causes were excluded. This is comparable to previously reported estimates,2 3 5 12 but slightly higher compared with 35% in the general population in this region (Statistics Norway).
We observed valvular disease/thoracic aneurysm as the cause of death in only three patients (3%). Pathological changes to the aortic wall or cardiac valves were reported in 82% of patients by Roldan et al,16 with an adverse outcome (heart failure, stroke, valve replacement or death) in as many as 20% of the patients. In a study comparing patients undergoing their first arterial coronary bypass operation (CABG), Hollan et al found that spondyloarthritis was a stronger predictor of early CABG than most traditional risk factors.17 It is probable that a systematic survey of our patients with echocardiography would have yielded a higher prevalence of valvular and thoracic disease, but mortality in our study is comparable to the mortality reported by Roldan et al.16
Pre-existing CVD was a predictor of premature death in the univariate analyses of the subpopulation of 360 patients but was not retained in the multivariate analyses, while increasing CRP levels were maintained as an independent predictor. This is probably not surprising given the important prognostic role of CRP in the prediction of CVD in general,18 19 and calls for an increased level of awareness of these predictors in the management of patients with AS. It would have been very interesting to evaluate the performance of a composite score of inflammation that includes CRP, like the AS Disease Activity Score,20 in this cohort. Unfortunately, this calculation was not possible based on the information in the database.
Death due to neoplastic diseases was the second largest subgroup in this study, accounting for 22.4% (N=22) of the total number and 26.8% of all known causes. This is higher than the previous estimates of mortality in patients with AS who have never been exposed to irradiation therapy,2 3 5 12 but comparable to the expected frequency in this region (Statistics Norway). As most patients who succumb to cancer have been admitted to a hospital at some time during their illness, this estimate probably reflects the incidence of death to cancer fairly accurately. The vast majority of these patients had been diagnosed with a solid tumour (N=14) and only three patients with a lymphoproliferative disease.
Infectious diseases caused 19.4% of all deaths, 23.3% of all known causes. This is substantially higher than previous reports,6 as well as the expected number of deaths compared with the general population where only 6% died as a consequence of infection. Pneumonia and septicaemia were the most frequently diagnosed infections, but there were no confirmed deaths related to tuberculosis which has been the most frequent cause of death by infection in AS according to previous reports.5 None of these infections was related to treatment with antitumour necrosis factor.
Violence-related deaths have been reported to occur more frequently in patients with AS than in the general population, and a Finnish study also suggested a link with alcohol.3 4 This is not supported by our data as only 2% suffered a traumatic death; none of these events was related to intake of alcohol compared with 6.5% in the general population in this region. It is therefore possible that the increased mortality due to alcohol is related to regional cultural differences and not to AS per se.
Reduced level of function, as measured by the Bath Ankylosing Spondylitis Functional Index, contributed to the increased risk of premature death in a univariate but not a multivariate model. In a recent Dutch study the level of function, as measured by the Bath Ankylosing Metrology Index, was related to cardiac conduction disturbances in a population of patients with AS.21 However, this study was not designed to evaluate any increase in mortality as a consequence of the conduction disturbance. Related to function, we found that work disability was independently associated with increased mortality (OR 3.65). This, of course, is a much wider definition of function than any composite score, but can also be interpreted as an indirect marker of disease activity.
There was a significant inverse relationship between mortality and use of NSAIDs at the time of follow-up, and patients who reported taking NSAIDs less frequently than on a monthly basis were clearly at increased risk of premature mortality (OR 4.35). Increased NSAID-related mortality has previously been reported,22 but other publications have contradicted these reports and actually found a reduced overall and CVD-related mortality in patients with polyarthritis using NSAIDs.23
In the multivariate analyses we found that diagnostic delay was independently associated with mortality (OR 1.05). In addition, there was a tendency towards increased mortality among patients who were older at the time of onset of AS, but this was not retained in the multivariate analyses. We have previously observed a relationship between a worse functional outcome in AS and age at disease onset,8 and speculated whether this relationship could be associated with the level of education. However, level of education did not contribute significantly to mortality. Instead, one could speculate that the tendency towards increased mortality observed in patients with a late onset may genuinely reflect a more severe course of AS in this subgroup of patients. It is also possible that this subset of patients has shown a particular neglect towards early symptoms of AS, and that ‘diagnostic delay’ rather than ‘late onset’ contributes to increased mortality as there will be a degree of uncertainty in the recollection of many subjects of the time of symptom onset.
CRP is a direct measure of disease activity and increasing levels of CRP were associated with increased mortality (OR 2.68). The excess mortality in patients with increased CRP, diagnostic delay, work disability and less frequent use of NSAIDs seems to point to a common feature of inflammation. An association between inflammation and increased risk of mortality has also been demonstrated by other groups.3 Traditional risk factors of cardiac disease such as hypertension, dyslipidaemia, elevated levels of fibrinogen and CRP have been reported to be more prevalent in patients with AS than in healthy controls,24 as well as a connection between cardiovascular risk factors and activity of AS.25 In a study by van Eijk et al26 it was also shown that there is a connection between microvascular function and level of disease activity in AS.
The diagnostic delay could imply that some patients have an unrecognised state of inflammation for several years prior to the start of any treatment. It has also been demonstrated that, even in longstanding disease with widespread ankylosis, histology demonstrates ongoing inflammation and active disease.27 In such a situation the use of NSAIDs could perhaps have an anti-inflammatory effect and thereby reduce the risk of cardiovascular events as indicated in the report by Goodson et al.23
A limitation of our study is that we were not able to extract data from the official Cause of Death registry and had to rely on the patients' hospital records to obtain the most likely cause of death. However, given the uncertainties in the reliability of death certificates in general28 and rheumatic diseases in particular,29 this may not have been a large disadvantage. With cause of death not established in 16 patients, this has probably led to an underestimation of circulatory diseases as a cause of death as cases of sudden death due to a circulatory event are likely to be found in this group.
In conclusion, we found standardised mortality to be increased in men with AS and circulatory disease was the major cause of death among patients with AS with measures of duration and intensity of inflammation as the significant prognostic factors of premature death. The implications of these findings are that a vigilant approach to the control of cardiovascular risk factors should be adopted in patients with AS, in addition to efforts for early detection and treatment of the disease.
References
Supplementary materials
Web Only Data
Files in this Data Supplement:
Footnotes
-
Funding GB has received a research grant from Northern Norway Regional Health Authorities and the Eimar Munthe memorial fund.
-
Competing interests None.
-
Ethics approval This study was conducted with the approval of the ethics committee of Northern Norway (REK Nord).
-
Provenance and peer review Not commissioned; externally peer reviewed.