Article Text

Abstract
Objectives To assess the sensitivity of the phagocyte-specific molecules myeloid-related protein (MRP) 8 and MRP14 (calprotectin) for monitoring disease activity during anti-interleukin (IL)-1 therapies in patients with cryopyrin-associated periodic syndromes (CAPS), including familial cold autoinflammatory syndrome (FCAS), Muckle–Wells syndrome (MWS) and chronic infantile neurological, cutaneous and articular (CINCA) syndrome.
Methods A total of 39 patients with CAPS, including 5 FCAS, 16 MWS and 18 CINCA syndrome, received anti-IL-1 therapy. All patients with CINCA and 12 with MWS were treated with IL-1Ra (anakinra), 14 patients with MWS with a monoclonal anti-IL-1β antibody (canakinumab) and patients with FCAS received IL-1 Trap (rilonacept). During serial clinical visits serum amyloid A, C-reactive protein, erythrocyte sedimentation rate and MRP8/14 serum levels were analysed.
Results Untreated patients with CAPS had significantly elevated MRP8/14 values. In response to treatment there was a significant reduction of MRP8/14 levels in CINCA (2,830 (range 690 – 8,480) ng/ml to 670 ng/ml, p < 0.001) and MWS patients (anakinra-treated: 4,390 (1790 – 9780) ng/ml to 1,315 ng/ml (p = 0.003); canakinumab-treated: 3,000 (500 – 13060) ng/ml to 630 ng/ml (p=0.001)). However, in many patients with CAPS, MRP8/14 levels were still elevated compared with healthy individuals, reflecting residual disease activity. However, canakinumab-treated patients with CAPS showed normalised MRP8/14 levels, suggesting control of phagocyte activation.
Conclusions Monitoring of cellular systems involved in inflammatory cascades of the innate immunity was successfully applied to the IL-1-driven CAPS diseases. This is the first study illustrating different states of subclinical disease activity in all types of CAPS depending on the type of anti-IL-1 therapy. MRP8/14 is a sensitive biomarker for monitoring disease activity, status of inflammation and response to IL-1 blockade in patients with CAPS.
Statistics from Altmetric.com
Introduction
Cryopyrin-associated periodic syndromes (CAPS) comprise a group of rare autoinflammatory diseases, which include the familial cold autoinflammatory syndrome (FCAS), the Muckle–Wells syndrome (MWS), and the chronic infantile neurological, cutaneous, and articular (CINCA) syndrome.
Different mutations in the NLRP3 (also known as CIAS1/NALP3/PYPAF1) gene locus 1q44, encoding for cryopyrin/NALP3 protein, are the cause of CAPS. Cryopyrin regulates the production of proinflammatory cytokines, such as interleukin (IL)-1β, by controlling the assembly of proteins forming the inflammasome complex. The integrity of the inflammasome structure is essential for caspase-1 activity which induces the conversion of pro-IL-1β to biologically active IL-1β.1,–,4 Uncontrolled pro-IL-1β processing results in a constitutive excess of IL-1β release from phagocytic cells of patients with CAPS.5,–,7
Patients with CAPS often show fever, pseudourticarial skin rash, joint involvement of varying degree, sensorineural hearing loss and eye involvement associated with neutrophil-mediated inflammation and an intense acute-phase response. CAPS represents a continuum of clinical manifestations in which FCAS shows the mildest, CINCA the most severe and MWS an intermediate-severity phenotype.
Today, targeted treatments are available for CAPS. Anti-IL-1 therapy is highly effective in CAPS such as MWS.8,–,11 Anakinra is a recombinant non-glycosylated form of the human IL-1 receptor antagonist (IL-1Ra) which blocks the biological activity of IL-1β and IL-1α by competitively inhibiting the binding of IL-1 to the IL-1 type I receptor (IL-1RI).12 The long-acting IL-1 inhibitor rilonacept (IL-1 Trap) is a fusion molecule comprising the extracellular component of the IL-1 receptor and the Fc portion of IgG1, with high affinity to IL-1β and IL-1α.13 Recently, another IL-1 inhibiting drug was developed. Canakinumab is a human monoclonal antibody targeted to IL-1β, which has been shown to provide selective and sustained blockade of IL-1β.14 15 While anti-IL-1 therapies improve clinical disease activity, it is not entirely clear if the complex disease mechanisms leading to inflammatory complications of CAPS are completely resolved at the molecular level. IL-1 hypersecretion is not easy to determine in vivo, and it is obviously only one factor among several involved in a complex immune dysregulation, including phagocyte activation during autoinflammation.16
Inflammatory markers can help to detect residual disease activity and to adjust the treatment to the individual needs. Classical and commonly elevated inflammatory markers in patients with CAPS include serum amyloid A (SAA) and C-reactive protein (CRP) as markers of the acute phase response and inflammation, and the erythrocyte sedimentation rate (ESR).9
The promising biomarkers MRP8 (myeloid-related protein 8, also known as S100A8) and MRP14 (S100A9) are phagocyte-specific proteins belonging to the novel group of damage-associated molecular pattern molecules (DAMPs), representing danger signals which share characteristics of cytokines.17 18 DAMP proteins represent endogenous ligands of pattern recognition receptors like the receptor for advanced glycation end products and the Toll-like receptors.17 MRP8 and MRP14 are secreted by activated phagocytes and bind to Toll-like receptor 4 which mediates downstream signalling and promotes inflammation19 and autoimmunity.20
Patients with juvenile idiopathic arthritis (JIA) show elevated MRP8/14 serum levels which correlate with individual disease activity, and moreover are predictive for disease flares after induction of clinical remission.21 Recently, we dissected the positive feedback mechanism of MRP8/MRP14 and IL-1β in systemic juvenile idiopathic arthritis and showed that MRP8/MRP14 serum levels are surrogate markers of IL-1β in patients with MWS.15 16 Although the exact role of the S100-DAMPs in autoinflammatory syndromes has not yet been fully unravelled, these proteins are promising markers of IL-1β-driven inflammation in CAPS. The aims of this study were to determine serum levels of MRP8/14 in patients with CAPS with phenotypes of different severity before and during different strategies of IL-1 blockade in correlation with the clinical efficacy of treatment.
Patients and methods
Study design
A prospective cohort study of consecutive patients diagnosed with active CAPS at the participating centres was performed between September 2003 and August 2008. The cohort of patients with CINCA and FCAS was included at the National Institute of Arthritis and Musculoskeletal and Skin Diseases.8 13 Patients with MWS were included at the University Hospital Tuebingen, Department of Pediatrics.22 The study was approved by the institutional ethics committee at each centre, and written informed consent was obtained from patients or their legal guardians.
Patients
All patients showed clinical features of active FCAS, CINCA or MWS and required medical intervention. Eighteen patients with CINCA syndrome aged between 4 and 32 years and with proven central nervous system involvement, 5 patients with FCAS aged 20–64 years and 16 patients with MWS aged 3–75 years of age were included (table 1). Patients were excluded if they received other immunomodulatory therapies such as methotrexate, had been immunised by live vaccinations within the past 3 months or if they either showed evidence for a pre-existing underlying infection or severe medical conditions such as alcohol abuse, recent infections or heart disease.
Characteristics of the patient cohorts including disease laboratory findings at baseline, before application of interleukin 1 inhibitors
Treatment regimens
Anakinra therapy
Anakinra (Kineret; Amgen, Cambrige, UK) was applied once daily subcutaneously at a dose of 1–2 mg/kg/day. Patients were treated with 100 mg/dose in patients ≥40 kg body weight, children with persistent disease activity received anakinra in a stepwise escalated dose to a maximum of 8 mg/kg. If required a concomitant non-steroidal anti-inflammatory drug was given.
Canakinumab therapy
Canakinumab (Ilaris; Novartis, Basel, Switzerland) was applied at a dose of 150 mg subcutaneously for ≥40 kg body weight or 2 mg/kg for <40 kg body weight every 2 months. If complete remission was not achieved by day 8, canakinumab was applied intravenously at a dose of 5 mg/kg body weight.
IL-1 Trap therapy
IL-1 Trap (Rilonacept; Regeneron Pharmaceuticals, Tarrytown, New York, USA) was administered weekly subcutaneously. The first dose was 300 mg as initial loading dose, followed by weekly administration of 100 mg.
Clinical and laboratory markers
All patients had typical clinical features of CAPS disease. Beside the clinical and physicians global assessment, patients recorded clinical signs and symptoms in a diary as described previously.8 13 22 Laboratory parameters were determined serially at each visit using standardised laboratory testing. This included examination of the classical inflammatory markers ESR, SAA and CRP. CRP values <0.5 mg/dl (lower sensitivity level of the used test) were defined as 0 mg/dl. Laboratory measurements of these inflammation markers were performed at the institutional laboratories either in Bethesda or in Tuebingen. Additionally, serum levels of MRP8/14 as a marker for phagocyte activation were measured for all patients in Muenster. Serum levels of MRP8/14 were determined by a double-sandwich ELISA system as described previously.23 The readers of the laboratory assay were blinded for the diagnosis and the inflammatory activity of the patients.
Statistical analysis
SPSS version 13.0 (SPSS Inc, Chicago, Illinois, USA) for windows was used for statistical analyses. Differences for parameters were compared between groups by Mann–Whitney U test. The paired samples were analysed by Wilcoxon test.
All tests of significance were two-tailed and a p value of <0.05 was considered as significant. Upper limit of healthy controls are defined as mean plus two SDs for MRP8/14,16 and are defined for the other inflammation parameters by the assay manufacturer. Data are expressed as mean with range except where stated otherwise.
Results
Patients
By the beginning of the study all patients had active disease, as indicated by clinical and laboratory examination. Twelve of the patients with CINCA syndrome had mutations in exon 3 of NLRP3, all other patients were patients with clinically defined with CINCA. All enrolled patients with FCAS were positive for NLPR3 mutations with a family history of FCAS in all but one patient. Twenty-one patients with MWS from four different families were screened for inclusion into the study. All patients were Caucasians, had clinical diagnosis of MWS and were carriers of heterozygous NLRP3 mutations. A total of 12 patients were included in the anakinra cohort. Patients were allowed to switch anti-IL-1 therapy for lack of efficacy or for patient preference. Ten of these patients later switched to canakinumab treatment. Upon discontinuation of anakinra a disease flare had to be awaited. The maximum wait time before the start of canakinumab therapy was set at 14 days. A total of 14 patients were gathered in the canakinumab cohort. Patients' and cohort specific characteristics are listed in table 1.
Study duration
The mean study duration and the short-term study follow-up varied from patient group to patient group (see table 1 and figures 1–3). This is owing to the different patient cohorts, which have been assermbled at different institutions and at different time points. Treatment safety was recorded and treatment efficacy was determined at each follow-up visit with clinical disease activity and inflammatory markers, including ESR, CRP, SAA and MRP8/14.

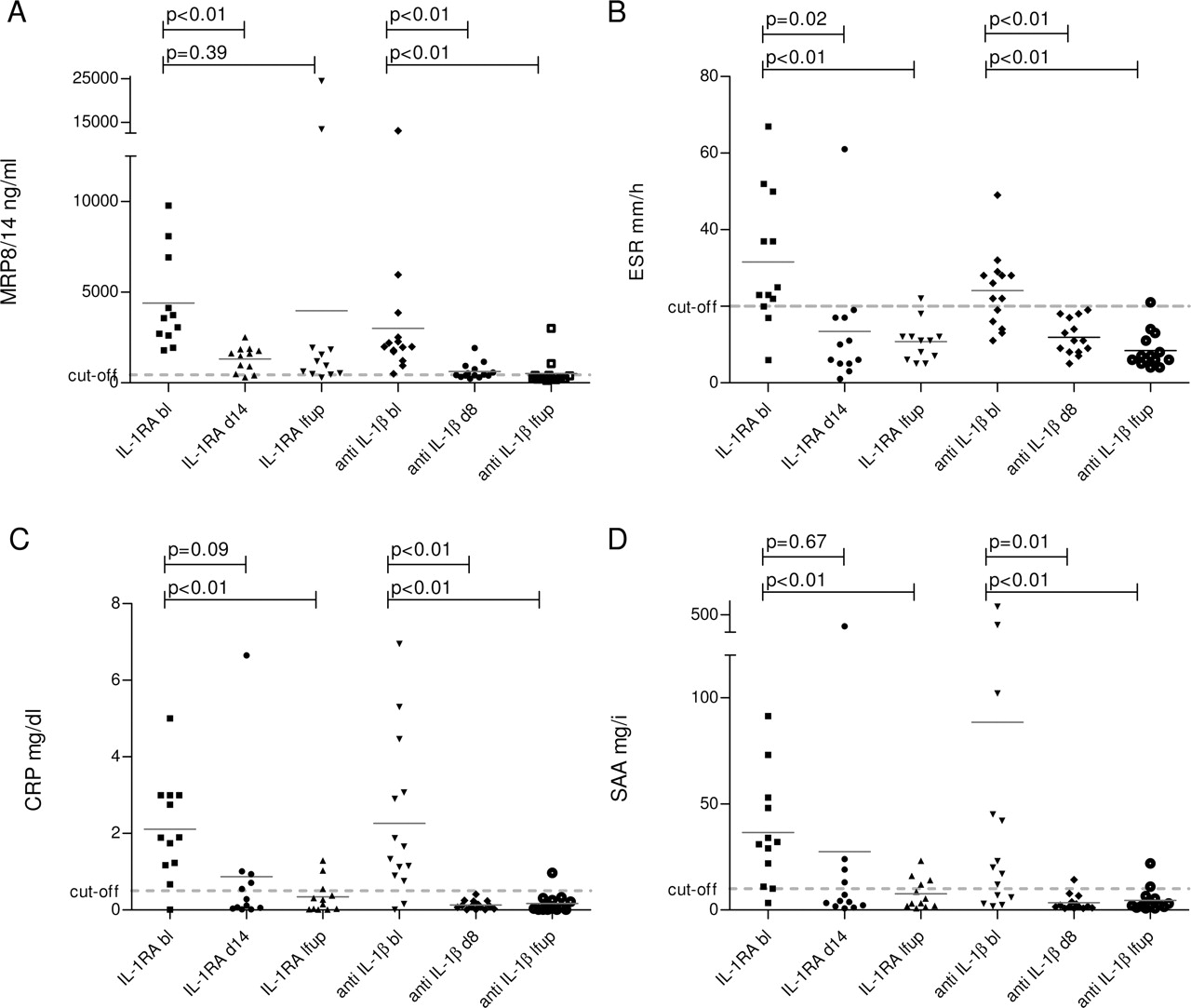
Interleukin (IL-1) blockade in patients with Muckle–Wells syndrome (MWS): anakinra versus canakinumab. (A) Serum concentrations of MRP8/14 (myeloid-related proteins); (B) ESR (erythrocyte sedimentation rate); (C) CRP (C-reactive protein) and (D) SAA (serum amyloid A) were determined in anakinra- (N=12) and canakinumab-treated patients with MWS (N=14) at baseline, short-term (day 14 in anakinra-treated patients, and day 8 in canakinumab-treated patients) and last follow-up (4–19 months in anakinra-treated patients, and 6–15 months in canakinumab-treated patients). The scatter plot depicts the measured values for each patient. Horizontal grey line indicates mean. Dashed grey lines indicate the upper limit of healthy individuals (MRP < 450 ng/ml, ESR < 20 mm/h, CRP < 0.5 mg/dl, SAA < 10 mg/l).

Individual follow-up of patients with chronic infantile neurological, cutaneous and articular (CINCA) syndrome treated with anakinra. (A) Serum concentrations of MRP8/14 (myeloid-related proteins); (B) ESR (erythrocyte sedimentation rate); (C) CRP (C-reactive protein) and (D) SAA (serum amyloid A) in 18 patients with CINCA before starting of interleukin 1 receptor antagonist (IL-1Ra; anakinra) treatment at baseline, after 3 months of treatment, after 12 months of treatment and at last follow-up (18 months). The scatter plot depicts the measured values for each patient. Horizontal line indicates mean. In general, MRP8/14 serum levels and the other inflammatory markers mirror the clinical response to treatment after starting anakinra therapy. Nevertheless, none of the inflammation markers normalise (and are less than the cut-off point of healthy controls as indicated by the grey dashed line) in a substantial proportion of patients.

{kind=link}
{kind=link}
{kind=link}
Individual follow-up of patients with familial cold autoinflammatory syndrome (FCAS) treated with interleukin 1 (IL-1) Trap. (A) Serum concentrations of MRP8/14 (myeloid-related proteins); (B) ESR (erythrocyte sedimentation rate); (C) CRP (C-reactive protein) and (D) SAA (serum amyloid A) in five patients with FCAS before starting IL-1 Trap (rilonacept) treatment at baseline, after 3 months of treatment, after 6 months of treatment and at last follow-up (24–32 months). The measured values are heterogeneous in the five patients and have a trend to decrease after the start of treatment. Nevertheless, significant differences cannot be seen in this small number of patients. The scatter plot depicts the measured values for each patient. Horizontal line indicates mean. Dashed grey line indicates the upper limit of healthy individuals (MRP < 450 ng/ml, ESR <20 mm/h, CRP < 0.5 mg/dl, SAA < 10 mg/l).
Serum concentrations of inflammatory markers before anti-IL-1 therapy
Before the start of treatment all patients with CAPS had raised MRP8/14 serum levels compared with healthy controls.16 Patients with CINCA syndrome had mean MRP8/14 levels of 2830 (range 690–8480) ng/ml, patients with FCAS of 3600 (300–11 570) ng/ml. Serum samples from patients with MWS from the anakinra cohort revealed MRP8/14 concentrations of 4390 (1790–9780) ng/ml and in the canakinumab cohort the mean serum concentration was 3000 (500–13 060) ng/ml (see table 1, figure 1). Mean MRP8/14 serum concentrations of the four patient groups did not differ significantly. In contrast, classical inflammatory markers at baseline were significantly higher in patients with CINCA syndrome than in patients with MWS. This is mainly because ESR, CRP and SAA values of the individual patients with CINCA were raised above normal cut-off values in all cases. In patients with MWS these inflammatory markers were raised only in 64–92% of the cases. Therefore, in a substantial number of these patients inflammatory activity was not detectable by ESR, CRP or SAA, but by MRP8/14.
Response to anakinra therapy
As reported in previous studies all patients with CAPS had an immediate clinical response to anakinra.8,–,10 Dermal symptoms, in particular, and overall patient well-being improved as documented in the diaries.8 22 Mean levels of MRP8/14 at day 14 in patients with MWS and after 3 months in patients with CINCA (short-term response) were significantly decreased to 670 ± 640 ng/ml (p < 0.001) in patients with CINCA syndrome and to 1315 (300–2510) ng/ml (p = 0.003) in patients with MWS. ESR levels decreased in both patient groups significantly (CINCA: mean 18 mm/h; p < 0.001 and MWS: 13 mm/h; p = 0.02). While CRP and SAA levels at short-term follow-up in patients with MWS decreased non-significantly, both classical inflammation markers were significantly decreased in patients with CINCA (both p < 0.001).
Patients with MWS treated with anakinra had raised MRP8/14 levels, even in 83% of the cases at the last follow-up—that is, after 4–19 months, although acute phase reactants normalised in the majority of these patients. Individual MRP8/14 values varied substantially at that time point so mean serum levels increased again, and the difference from pretreatment values did not reach significance any more (p = 0.386). We analysed individual MRP8/14 levels, especially in outlier measurements, but we found no obvious correlations with more severe disease activity or with clinically defined flares in these patients. One reason for the variance of patient values may lie in ongoing subclinical phagocyte activation of the patients with MWS, as already detected in patients with JIA at risk for flares (figure 1).21
During follow-up for 18 months of patients with CINCA who were receiving anakinra, there was a sustained clinical response to treatment in all patients.8 MRP8/14 serum levels remained lower in general, but throughout the study period until last follow-up, at least 44% of the patients had levels above the cut-off value of normal controls (figure 2). CRP, ESR and SAA had a similar response pattern to that of MRP8/14 and also remained elevated in roughly half of the patients with CINCA throughout the whole study period. At last follow-up only two patients had normalised levels of all four markers of inflammation (MRP, ESR, CRP and SAA).
Response to canakinumab therapy
The short-term response rate of patients with MWS to canakinumab at day 8 was excellent. Clinical symptoms of the patients and global assessment improved. Mean levels of MRP8/14 after 8 days of canakinumab therapy (short-term end point) were significantly decreased to 630 (240–1920) ng/ml (p=0.001) (figure 1). In contrast to the anakinra-treated patients levels of classical inflammatory markers had already decreased significantly at the short-term end point. None of the canakinumab-treated patients showed abnormal ESR levels or abnormal CRP levels at this time point, only one patient had an abnormal SAA value.
At last follow-up only 14% of canakinumab-treated patients had elevated MRP8/14 levels. Moreover, the mean further decreased to 520 (140–3010) ng/ml (p=0.002). ESR, CRP and SAA remained in the range of healthy individuals.
Response to IL-1 Trap treatment
All patients with FCAS responded immediately to the administration of rilonacept with reduced cold-induced attacks and improvement in symptoms.13 MRP8/14 serum levels in the five patients were heterogeneous (figure 3). Although the mean levels before treatment were in the same range as for the other CAPS diseases and there was a clear downwards trend, the small number of patients did not allow significant differentiation between levels before and after successful treatment. ESR, CRP and SAA levels during rilonacept treatment reduced significantly. However, our data suggest that subclinical inflammatory activity may still be present in patients with FCAS receiving treatment, which needs to be further analysed in larger sets of patients.
Discussion
Monitoring disease activity in CAPS is challenging. To determine treatment response, and to possibly adjust treatment, it is useful to evaluate inflammation markers. The main goal of treatment is to prevent organ damage from continuing inflammation. Commonly elevated inflammatory markers include SAA, CRP and ESR.9 ESR has been used in previous anti-IL-1 studies and SAA was previously described as an important predictive marker for amyloidosis.8 9 24 The primary goal of this study was to identify the potential of MRP8/14 as a sensitive biomarker for IL-1β-driven inflammation in patients with CAPS.
MRP8/14 has been already proposed as an inflammatory marker in rheumatoid arthritis, JIA, inflammatory bowel disease and sepsis.17 25 However, MRP8/14 is most markedly elevated in diseases involving systemic autoinflammation such as systemic-onset JIA.16 The feedback link between MRP8/14 and IL-1 hypersecretion, in particular, as described by us previously, is a key phenomenon in this disease. The close correlation of these molecules, and the difficulties of measuring IL-1β in patient samples are the rationale for analysing MRP8/14 as a surrogate marker for IL-1β-driven inflammation.15 Our analysis of serum samples from patients with CAPS with severe disease activity showed significantly elevated MRP8/14 serum levels for CINCA, for FCAS and in the same range for patients with MWS. These concentrations are in a similar range to those for patients with other inflammatory diseases, in which the MRP8/14 complex has already been proposed as a reliable biomarker for disease activity.25 Neither of the measured inflammation markers could be correlated to the clinical phenotype of the different CAPS diseases.
Response to treatment in the short term was mirrored by classical inflammation markers and by MRP8/14 regardless of patient group and treatment. When monitoring disease activity during IL-1 blockade treatment in the long term, different dynamics of inflammatory markers were found to depend on patient and treatment group. Despite clinical response, patients with CINCA treated with anakinra displayed slightly elevated MRP8/14, CRP, ESR and SAA levels during the whole follow-up, in accordance with ongoing clinical symptoms such as bony overgrowth, this is not responding to IL-1Ra therapy. Multiple determinations of inflammatory markers may improve the diagnostic ability of detecting subclinical disease activity in this patient group. Even more striking than in CINCA, anakinra-treated patients with MWS in clinical remission had classical inflammatory markers in the normal range but MRP8/14 serum concentrations were still increased, indicating that during IL-1Ra therapy some inflammatory activity may persist or reoccur involving innate immune mechanisms.
Clinically useful cut-off values above the normal range are hardly to define from these data and should be examined in future studies. However, MRP8/14 identified subclinical inflammation in more patients receiving anakinra than when disease activity was monitored with acute phase reactants. MRP8/14 was more sensitive at day 8 of the canakinumab treatment than classical inflammatory markers. Thus MRP8/14 could be used to identify patients who need to adjust their anakinra therapy (increase in dose) or those who should be switched to canakinumab. This is of clinical relevance, as patients with MWS have a greater risk of developing SAA amyloidosis and other disease-related complications. Switching treatment to the anti-IL-1 antibody canakinumab led to a significant improvement and normalisation of all disease activity parameters including MRP8/14 in the short and long term. This reflects a sustained and stable remission of MWS disease activity following canakinumab therapy and indicates that MRP8/14 is the most reliable surrogate marker for IL-1β-driven inflammation.
Conclusions for patients with FCAS may be preliminary, because of the small number of patients, and need to be confirmed in a larger cohort of patients for the analysis of statistical significance and also to evaluate how patients with FCAS might benefit from improved medication monitored by biomarkers. Interestingly, as for anakinra-treated patients with CAPS, the MRP8/14 levels do respond to treatment but remain increased above normal values for the whole follow-up. Patients with FCAS in this study are generally older, which may represent a confounding variable for the comparison of initial MRP8/14 levels, although previously published data showed no differences in MRP8/14 values between adults and children.16 Previous studies have suggested the possible dynamics of normalising MRP8/14 and of other phagocyte-specific S100 protein levels during effective anti-inflammatory treatment in the range of 1–2 weeks.15 16 26
The phagocyte-specific MRP8/14 complex is a marker for monocyte and neutrophil activation. Accordingly, MRP8/14 levels might be elevated, while ESR, CRP and SAA, which reflect the acute phase reaction of the liver, remained low or even decreased further. A similar phenomenon has been described for patients with JIA. Patients with JIA during clinical remission but prone to relapse exhibit elevated MRP8/14 serum levels but no alterations of the classical inflammatory markers CRP and ESR. Patients with MRP8/14 serum concentrations >700 ng/ml could be identified with a sensitivity of about 85% as likely to relapse in the next 3 months.21 27
Our data suggest that the MRP8/14 complex is a sensitive marker in patients with CAPS, with the ability to detect subclinical, IL-1β-dependent disease activity. Expressed in phagocytes, MRP8/14 is released actively into the extracellular space upon inflammatory activation.28 This cell system is the source of a number of proinflammatory cytokines and can be found at affected sites in several autoimmune diseases. For instance, MRP8/14 has been identified in early infiltrating phagocytes in rheumatoid arthritis and vasculitis.23 29 30 As an endogenous danger signal, MRP8/14 mediates early inflammatory responses and recruits immune cells to inflamed tissues.31 MRP8/14 induces both increased permeability of endothelial monolayers and raised adhesion of neutrophils to the endothelium. This results in increased leucocyte extravasation and further propagates inflammatory processes.32 33 Measuring MRP8/14 concentrations in the serum of affected individuals is a reliable tool to monitor inflammation at the cellular level. Phagocyte activation locally and/or systemically is reflected, while classical inflammation markers reflect late systemic inflammatory responses.
This study illustrates different states of subclinical disease activity in patients with CAPS depending on the type of anti-IL-1 therapy. The study demonstrates (a) increased initial levels of classical inflammation markers in patients with CAPS, pronounced in CINCA and FCAS and less pronounced in patients with MWS, before starting anti-IL-1 therapy; (b) clearly elevated initial MRP8/14 serum concentrations in the range of other inflammatory diseases and with no significant difference between CINCA and FCAS and MWS; (c) good correlation of classic inflammation markers and MRP8/14 with early response to treatment in patients with CAPS and (d) lower levels of MRP8/14 serum concentrations in patients with CAPS successfully treated with canakinumab than in anakinra-treated patients, indicating continuing subclinical disease activity in the latter patients.
Taken together, this is the largest biomarker study in CAPS to date, investigating all phenotypes of CAPS diseases, treated with all types of available anti-IL-1 strategies. The MRP8/14 complex is a reliable marker for phagocyte activation and is therefore an appropriate marker to reflect the activity of inflammation in CAPS as a surrogate marker for IL-1β. Long-term data for anti-IL-1 treatment are still lacking, therefore the impact of probable subclinical disease activity on the later outcome of patients will have to be investigated with further longitudinal studies. Individualised treatment strategies may evolve in the future to identify patients with CAPS with continuing subclinical inflammation and need for additional/different treatment to prevent late sequelae of the disease and to improve the quality of life of the patients.
Acknowledgments
The authors thank Melanie Saers, Susanne Schleifenbaum and Dorothee Lagemann for excellent technical assistance.
References
Footnotes
HW and JBK-D have contributed equally to the manuscript
-
Funding Supported by grants from the Interdisciplinary Centre for Clinical Research at the University of Muenster (project Foe2/005/06), the Deutsche Forschungsgemeinschaft (DFG project FO 354/2-2), and the Bundesministerium für Bildung und Forschung (AID-NET, project 01GM08100).
-
Ethics approval This study was conducted with the approval of the institutional review boards of the NIH, the University Hospital Tuebingen and the University Hospital Muenster.
-
Provenance and peer review Not commissioned; externally peer reviewed.