Article Text

Abstract
Objective This study was aimed at investigating the frequencies of non-radiographic axial spondyloarthritis (nr-axSpA) and ankylosing spondylitis (AS) diagnoses and their ratios in relation to symptom duration in patients referred because of chronic back pain and suspicion of axial SpA.
Methods In this monocentre study, orthopaedists and primary care physicians were requested to refer patients with chronic low back pain (duration >3 months) and onset of back pain before 45 years of age to a SpA-specialised rheumatology outpatient clinic for further diagnostic investigation, if proposed screening parameters were present. The ratio of nr-axSpA to AS was analysed in relation to the duration of symptoms.
Results A diagnosis of definite axial SpA was made in 43.7% of the referred patients (n=522). Axial SpA was diagnosed in a similar percentage of about 50% if back pain duration was <9 years but decreased to 36% if symptom duration was >9 years. Nr-axSpA represented the majority of patients (67.3%) only if duration of back pain was 1 year and less at the time of referral. Between 1 and 6 years of back pain duration the probability of nr-axSpA and AS was nearly equal (1–3 years: 52.5% and 47.5%, respectively; 3–6 years: 53.7% and 46.3%, respectively). In patients with back pain duration of 6–9 years, AS was more likely (61.1%) to be diagnosed than nr-axSpA (38.9%), and this increased further over time.
Conclusions Non-radiographic axial SpA represents an important differential diagnosis of back pain, especially in patients with recent symptom onset.
- Ankylosing Spondylitis
- Spondyloarthritis
- Epidemiology
Statistics from Altmetric.com
Recently new classification criteria for axial spondyloarthritis (axSpA) have been developed which cover both patients with radiographic sacroiliitis as defined by the modified new criteria for ankylosing spondylitis (AS) and patients with non-radiographic axSpA (nr-axSpA) before the occurrence of chronic structural changes in the sacroiliac (SI) joints, which is a prerequisite for a positive x-ray finding.1 ,2 In addition, diagnostic algorithms have been proposed for axSpA.3 ,4 This was an important step forward to reduce the big delay between first onset of symptoms and making a diagnosis of axSpA of between 5–10 years5 and to allow earlier treatment of these patients.
This raises the question about the relevance of nr-axSpA in daily clinical practice, especially about the ratio of nr-axSpA to AS in patients who present to the rheumatologist with unclear chronic back pain and a possible diagnosis of axSpA. Some studies have been conducted recently investigating referral strategies in primary care settings to identify patients with axSpA earlier.6–9 Here a percentage of nr-axSpA among the whole group of axSpA patients of between 25% and 58% were reported.6–9 In the current investigation we analysed in more detail the ratio of nr-axSpA to AS in relation to symptom duration in patients referred to the Berlin early spondyloarthritis clinic because of chronic back pain and suspicion of axSpA.
Methods
The applied referral strategy and the patients’ work up in the Berlin early SpA clinic have been described in detail elsewhere.6 ,10 Briefly, orthopaedists and primary care physicians were asked to refer patients with chronic low back pain (duration >3 months) and onset of back pain before 45 years of age to the rheumatology outpatient clinic of the Charité—Campus Benjamin Franklin in Berlin, if at least one of the following screening parameters was present: (1) inflammatory back pain; (2) positive testing for HLA-B27 or (3) sacroiliitis detected by imaging (only if available, was not recommended as an initial screening parameter).
In the SpA clinic, diagnostic procedures required for confirmation/exclusion of axSpA were performed. The latter included collection of patient's symptoms and history, physical examination, measurement of acute phase reactants (C-reactive protein (CRP) and erythrocyte sedimentation ratio), HLA-B27 testing, and imaging of the SI joints (x-rays, MRI, and/or CT—whatever was required in the opinion of the rheumatologist). Finally, the decision on definite axSpA, possible SpA and non-SpA was made in all cases. Definite axSpA diagnosis was further split into AS according to modified New York criteria11 and into nr-axSpA (ie, definite axSpA in the opinion of the rheumatologist without definite radiographic sacroiliitis). The rheumatologist's decision on the diagnosis was used as a ‘gold standard’. All obtained data were entered into the database and subsequently analysed. Methods of descriptive statistics, the Fischer's exact test, and the Mann-Whitney U-test were applied as appropriate.
Study protocol was approved by the local ethics committee of Charité—Campus Benjamin Franklin and all participants gave informed consent.
Results
In total, 522 patients were referred between July 2004 and April 2007. The principal characteristics of the referred patients are presented in table 1. Among all referred patients, 43.7% (n=228) were diagnosed with definite axSpA (of these, 52.2% (n=119) patients with AS and 47.8% (n=109) with nr-axSpA), in 49% of the patients (n=256) axSpA was definitely excluded (non-SpA group), and only in 7.3% (n=38) an uncertain diagnosis of possible SpA was made. These data are in line with our previous report concerning a population of 350 referred patients.6 In 84 out of the 109 nr-axSpA patients (77%) with a final diagnosis of nr-axSpA an MRI of at least the SI joints was performed; in 86.9% of these patients an active MRI-inflammation of the SI joints was present. Out of the 109 patients who had a diagnosis of nr-axSpA according to the local expert 103 (95%) would have also fulfilled the new Assessment of SpondyloArthritis international Society (ASAS) criteria for axial spondyloarthritis1 ,2 (70 patients the imaging and 33 the clinical arm of the criteria).
Overall characteristics of the referred patients
The mean disease duration (duration of back pain) was 9.0±9.3 years for the whole axSpA group at the time point of the referral; this was clearly longer in patients with AS (10.3±10.0 years) as compared to nr-axSpA (5.4±6.7 years, p<0.001). Patients in the non-SpA group had a mean disease duration comparable to those in AS (10.2±9.9 years).
For a more detailed analysis, referred patients were grouped according to the duration of symptoms into the following 6 groups: ≤1 year, >1–≤3 years, >3–≤6 years, >6–≤9 years, >9–≤12 years, >12 years.
In patients with duration of back pain up to 9 years, there was no clear difference in the percentage of referred patients with a final diagnosis of axSpA of about 45–50% at the different time points—figure 1. Importantly, in patients with back pain duration of more than 9 years and, especially, more than 12 years, the probability of an axSpA diagnosis decreased substantially, while other reasons of back pain (non-SpA group) became more prevalent—figure 1.

Frequencies of axial spondyloarthritis (SpA), possible SpA and non-SpA among patients referred because of pack pain (n=522) in relation to the back pain duration.
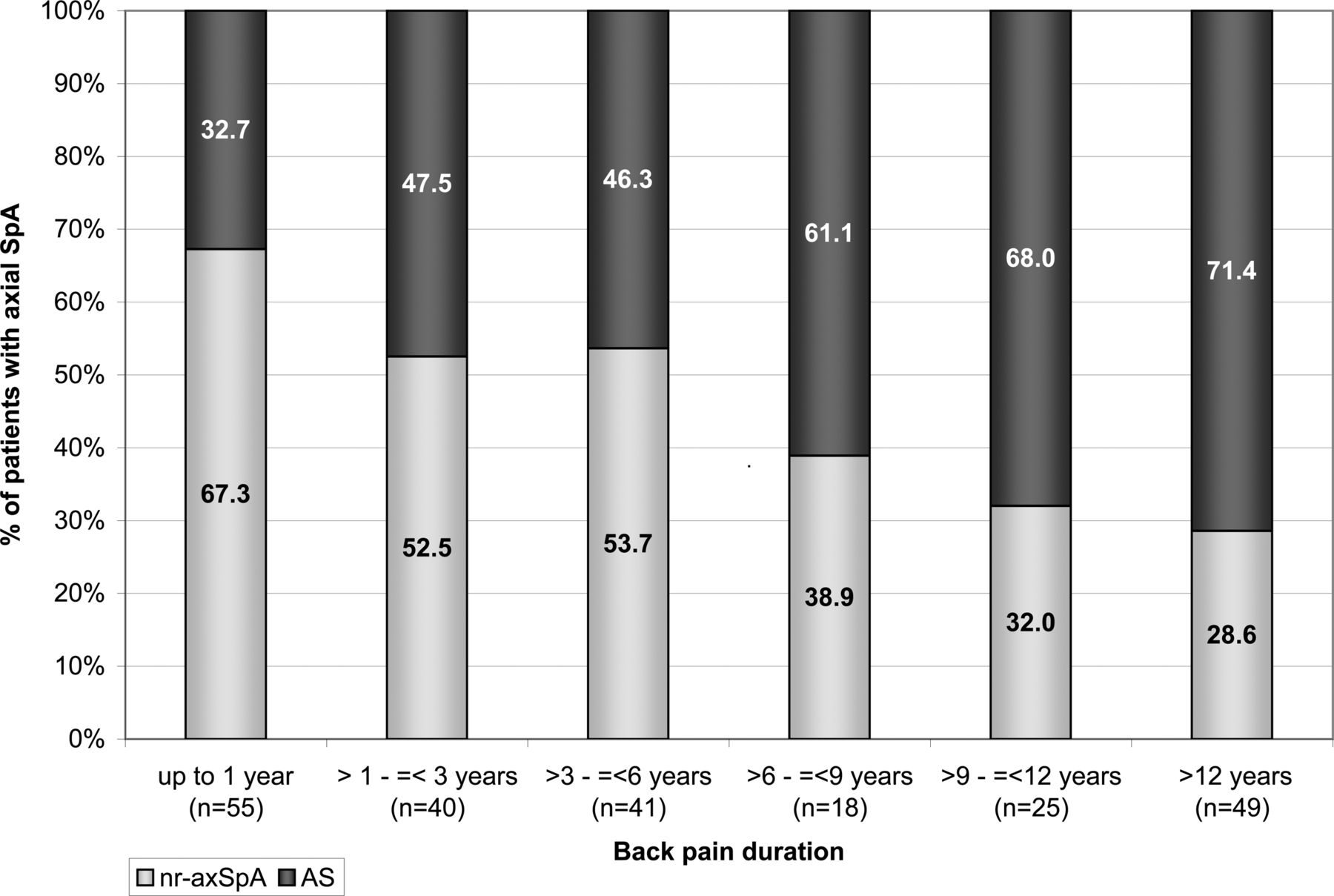
The nr-axSpA/AS ratio among the axSpA patients was also dependent on the duration of symptoms—figure 2. In the first year of back pain, nr-axSpA was more likely than AS, between 1 and 6 years of back pain both diagnoses were nearly equally probable, while after 6 years AS became more likely and this increased further over time—figure 2. Differences in the frequencies of axSpA subgroups become statistically significant after 9 years (nr-axSpA to AS ratio: 32%–68%) as compared to the group with the symptom duration of ≤1 year (nr-axSpA to AS ratio: 67%–33%, p=0.004). This difference became even more clear in the group with symptom duration of >12 years (figure 2) and statistically significant not only versus the group with the symptom duration ≤1 year (p=0.001), but also versus the group with symptom duration >1–≤3 years (p=0.029).
{kind=link}
{kind=link}
Ratio of non-radiographic axial spondyloarthritis (nr-axSpA) to ankylosing spondylitis (AS) among patients who were referred because of back pain and who were diagnosed with definite axial SpA.
The mean CRP value was significantly (p=0.001) higher in the AS group (1.67±4.18 mg/l) compared to the nr-axSpA group (0.96±2.84 mg/l). This tendency for a higher CRP in the AS group versus the nr-axSpA group, respectively, was similar for all six groups, however, this difference was not always significant due to a smaller sample size: ≤1 year: 4.33 versus 1.71 mg/l (p=0.015), >1–≤3 years: 1.25 versus 0.48 mg/l (p=0.093), >3–≤6 years: 1.52 versus 0.90 mg/l (p=0.53), >6 years–≤9 years: 2.24 versus 0.40 mg/l (p=0.011), >9 years–≤12 years: 0.97 versus 0.55 mg/l (p=0.17), >12 years: 0.91 versus 0.53 mg/l (p=0.52).
Discussion
In the current investigation we analysed data from 522 patients who were referred to the rheumatologist because of unclear chronic back pain, in whom definite axSpA was diagnosed in 43.7%. When these data were analysed in more detail in relation to the disease duration at the time point of the diagnosis, we found that the probability of a definite axSpA diagnosis remained nearly constant (about 50%) in patients with duration of the back pain of less than 10 years and decreased substantially in patients with longer duration—figure 2. These results indicate that in patients with a long history of back pain (10 years and more), in whom a definite diagnosis has not been established yet, axSpA is a less likely reason of back pain in comparison to other reasons, such as degenerative spine disease.
Even more interesting is the ratio of nr-axSpA to AS in relation to the duration of back pain. Among all patients diagnosed with definite axSpA, 52.2% were diagnosed with AS and 47.8% with nr-axSpA. However, this ratio changed over time: in patients with back pain duration of 1 year or less only nr-axSpA was more often (67%) than AS (33%), but already between the first and the third year of back pain the probabilities of nr-axSpA and AS were nearly equal—figure 2. After 6 years of back pain, established AS started to become more likely than nr-axSpA, and this increased further over time. We have reported previously that the progression rate of nr-axSpA to AS over 2 years is about 12%,12 which is in line with the increase from 33% at year 1 up to 68% at year 10 in the current cross-sectional analysis. Additional information about the relation between the ratio of nr-axSpA to AS and symptom duration came from tumour necrosis factor α blocker trials in early axSpA. In active axSpA patients with a symptom duration of less than 3 years (mean 1.3 years)13 or less than 5 years (mean 2.9 years),14 the percentage of AS as part of the whole group was 12% and 51%, respectively, which is not so different from the numbers reported here.
Our data indicate that patients with nr-axSpA represent a substantial proportion of patients with axSpA if duration of symptoms is short: more than a half of the patients presenting to a rheumatologist did have no radiographic damage in the spine within the first 6 years of the disease. On the other hand, advanced structural changes in the SI joints can occur already quite early in the course of the disease as shown by the 33% of axSpA patients with an AS diagnosis in the first year of their disease. Interestingly, the CRP value was especially high in these AS patients with such a short symptom duration indicating that elevated CRP is an important risk factor for rapid progression from nr-axSpA to AS. Indeed, we could recently already show in another longitudinal study over 2 years of axSpA patients that elevated CRP was the most relevant predictive factor for the development of radiographic sacroiliitis.12
The data presented here are based on an analysis of patients seen at a single tertiary rheumatology centre with a special interest in SpA. Thus, it has to be confirmed in additional investigations like this one that the numbers presented here are representative.
In conclusion, the present study shows that nr-axSpA is quite an important subgroup among the axSpA patients, especially in the first 10 years of the disease, and that there is a decrease in nr-axSpA to AS ratio over time confirming the concept of axSpA as the same disease. For making a diagnosis of axSpA earlier the inclusion of patients with nr-axSpA in a diagnostic approach is therefore essential.
Acknowledgments
We would like to thank all orthopaedists and primary care physicians who referred their patients. Further we would like to thank rheumatologists in our centre who performed diagnostic procedures on the referred patients: Anna Amtenbrink, Heiner Appel, Hildrun Haibel. We are grateful to Beate Buss for the support with the study documentation.
References
Footnotes
-
Contributors All the listed authors fulfill the authorship requirements.
-
Funding The study was partly supported by unrestricted grants from Essex Pharma GmbH (now MSD Sharp & Dohme GmbH), Germany and Wyeth Pharma GmbH (now Pfizer Deutschland GmbH), Germany.
-
Competing interests The authors declare no conflict of interest in relation to the content of this manuscript.
-
Ethics approval Ethics committee of Charité.
-
Provenance and peer review Not commissioned; externally peer reviewed.