Article Text

Abstract
Objectives To evaluate incidence-trends and timing of large-vessel (LV) manifestations in patients with giant cell arteritis (GCA), and to examine the influence of LV manifestations on survival.
Methods A population-based incident cohort of patients diagnosed with GCA between 1950 and 2004 was used. LV involvement was defined as large-artery stenosis or aortic aneurysm/dissection that developed in the 1 year before GCA diagnosis or at any time thereafter. Patients were followed up until death or 31 December 2009.
Results The study included 204 patients, 80% women, mean age at diagnosis of GCA 76.0 years (±8.2 years). Median length of follow-up was 8.8 years. The cumulative incidence of any LV manifestation at 10 years was 24.9% for patients diagnosed with GCA between 1980 and 2004 compared with 8.3% for patients diagnosed with GCA between 1950 and 1979. The incidence of any LV event was high within the first year of GCA diagnosis. The incidence of aortic aneurysm/dissection increased 5 years after GCA diagnosis. Compared with the general population, survival was decreased in patients with an aortic aneurysm/dissection (standardized mortality ratio (SMR) 2.63; 95% CI 1.78 to 3.73) but not in patients with large-artery stenosis (SMR 1.44; 95% CI 0.87 to 2.25). Patients with GCA and aortic manifestations had a higher than expected number of deaths from cardiovascular and pulmonary causes than the general population. Among patients with GCA, aortic manifestations were associated with increased mortality (HR=3.4; 95% CI 2.2 to 5.4).
Conclusions Vigilance and screening for aortic aneurysms should be considered in all patients 5 years after the incidence of GCA. Aortic aneurysm/dissection is associated with increased mortality in GCA.
- Giant Cell Arteritis
- Epidemiology
- Cardiovascular Disease
Statistics from Altmetric.com
Introduction
Giant cell arteritis (GCA) is a chronic, granulomatous medium-size and large-vessel (LV) vasculitis that affects the aorta and its branches. The incidence of any LV manifestation such as large-artery stenosis (LAS), aortic aneurysm or aortic dissection is estimated to be 30.5 events per 1000 person-years at risk.1 Patients with GCA have a 17-fold increased risk of developing thoracic aortic aneurysm compared with the general population.2 It has been recommended that patients with GCA should be screened for this manifestation but the optimal imaging modality which should be used and the frequency with which screening should be performed are unknown.2 ,3 With the increased use of imaging modalities, involvement of the aorta and, or its branches is often detected in patients with newly diagnosed GCA with estimates ranging from 22% to 85%.4–9 Predictors of LV involvement in GCA remain poorly understood. Although overall survival in patients with GCA is similar to that in the general population, a previous study found that patients with thoracic aortic dissection have higher mortality.10–16
Our study aims were to (1) to evaluate predictors, time-trends and timing of LV manifestations in a well-defined cohort of patients with GCA; (2) to assess survival and cause-specific mortality in the patients with GCA and LV disease compared with the general population and (3) to evaluate the association between the different LV manifestations in patients with GCA and survival.
Patients and methods
This was a retrospective, population-based cohort study using the resources of the Rochester epidemiology project, a unique records-linkage system which allows ready access to the medical records of all healthcare providers for the population of Olmsted County, Minnesota.17 A cohort of patients with GCA diagnosed between 1950 and 2004 has already been established and previously described.18 ,19 All patients in this cohort met the 1990 American College of Rheumatology classification criteria for GCA.20 The complete (inpatient and outpatient) medical records for all patients in this cohort were reviewed. All patients were followed up until migration, death or 31 December 2009 (end of study). The study was approved by the institutional review boards at Mayo Clinic and Olmsted Medical Center.
Standardised case report forms were used to abstract data. We collected information on date of diagnosis of GCA, symptoms and laboratory findings at GCA diagnosis, presence of LV involvement, date of diagnosis of LV involvement, method of diagnosis and arteries affected. Incident LV involvement or LV manifestation was defined as LV complications including LAS, aortic aneurysm or aortic dissection/rupture detected within 1 year before diagnosis of GCA or at any time thereafter.21 ‘Aortic manifestations’ were defined as aortic aneurysm or aortic dissection/rupture. Previously used definitions for LAS and aortic aneurysm, rupture and dissection were also used for this study. The diagnosis of LV disease required confirmation by imaging, histopathology or autopsy.21
Vital status at the end of the study (31 December 2009) was recorded for each patient. All subjects (irrespective of residency status) were tracked nationally to ascertain vital status, and death certificates were obtained from the respective states for subjects who died outside Minnesota. If the patient had died, death certificates were reviewed to ascertain the physician-designated causes of death.
Statistical analysis
The cumulative incidence of each LV event adjusted for the competing risk of death was estimated. Poisson regression models were used to model the rates of LV involvement over the disease duration. Smoothing splines were used to allow for non-linear time trends. Cox proportional hazards models were used to assess the association of risk factors with the development of LV events. To evaluate secular trends, we divided the cohort into two different study periods: those diagnosed with GCA between 1950 and 1979 and those diagnosed with GCA between 1980 and 2004. The cumulative incidence rates for the two time periods were compared using Gray's methods.22
The distribution of survival times after the GCA incidence date was estimated using the Kaplan–Meier method. The expected number of deaths was determined from the National Center for Health Statistics life tables for the US population, according to the age, sex and calendar year of the GCA cohort. The standardised mortality ratio was estimated by dividing the observed number of deaths by the expected number of deaths. Ninety-five per cent CIs for the standardized mortality ratio were calculated assuming that the expected rates were fixed and the observed rates followed a Poisson distribution.
The underlying cause of death was coded from national mortality statistics and grouped according to the International Classification of Diseases, 9th revision (ICD-9) and ICD-10 chapters. Cause-specific expected mortality rates were estimated by applying the age-, sex- and calendar-year-specific mortality rates from the Minnesota Caucasian population (1980–2002) to the GCA cohort. Cause-specific Minnesota life tables were available until the end of 2002. Therefore, we carried forward the 2002 expected mortality rates to 2009. American Heart Association classification was used to categorise death from cardiovascular disease into coronary heart disease (CHD), non-CHD and non-cardiac circulatory diseases.23
Survival after LV disease was estimated with each Kaplan–Meier curve starting at the date of diagnosis of LV involvement instead of at the GCA incidence date. Cox proportional hazards models were used to examine the association between LV involvement and mortality. Time-dependent covariates were used to represent LV involvement, which occurred throughout follow-up.
Results
The cohort
The study population included 204 patients diagnosed with GCA between 1 January 1950 and 31 December 2004. Temporal artery biopsy was positive in 176 (86%) patients. All subjects met the 1990 American College of Rheumatology classification criteria for GCA. Mean age (±SD) at diagnosis of GCA was 76.0 (±8.2) years. The cohort was predominantly female (163 subjects; 80%). Median duration of follow-up was 8.8 years (total 1996 person-years). Baseline demographics for the cohort are available in the online supplementary table S1.
LV manifestations and predictors
Fifty-six patients developed 63 LV events—36 aortic manifestations and 27 LAS. Aortic aneurysms were diagnosed in 33 patients (isolated thoracic aneurysm in 14 cases, isolated abdominal aneurysm in six cases and both thoracic and abdominal aneurysms in 13 cases). The cumulative incidence (±SE) of any clinically evident LV manifestation, after adjusting for competing risk of death, was 19.9% (±2.9) at 10 years. Clinical and treatment variables as predictors of LAS or aortic aneurysm/dissection are evaluated in table 1.
Clinical variables and their association with large-artery stenosis or aortic aneurysm/dissection in 204 patients with giant cell arteritis (GCA)*
Time-trends and timing of LV manifestations
The cumulative incidence of any LV manifestations at 10 years increased significantly, from 8.3% in the cohort diagnosed between 1950 and 1979 to 24.9% for patients diagnosed between 1980 and 2004 (p=0.004). While the cumulative incidence of LAS and aortic aneurysms increased for patients diagnosed in the earlier decades compared with those diagnosed between 1980 and 2004, the cumulative incidence of aortic dissection remained unchanged (table 2). A greater proportion of patients with GCA diagnosed between 1980 and 2004 underwent echocardiography (p<0.001), abdominal ultrasonography (p=0.03) and angiography, CT or MRI (p<0.001).
Time-trends in cumulative incidence rates at 10 years of LV involvement in 204 patients with GCA
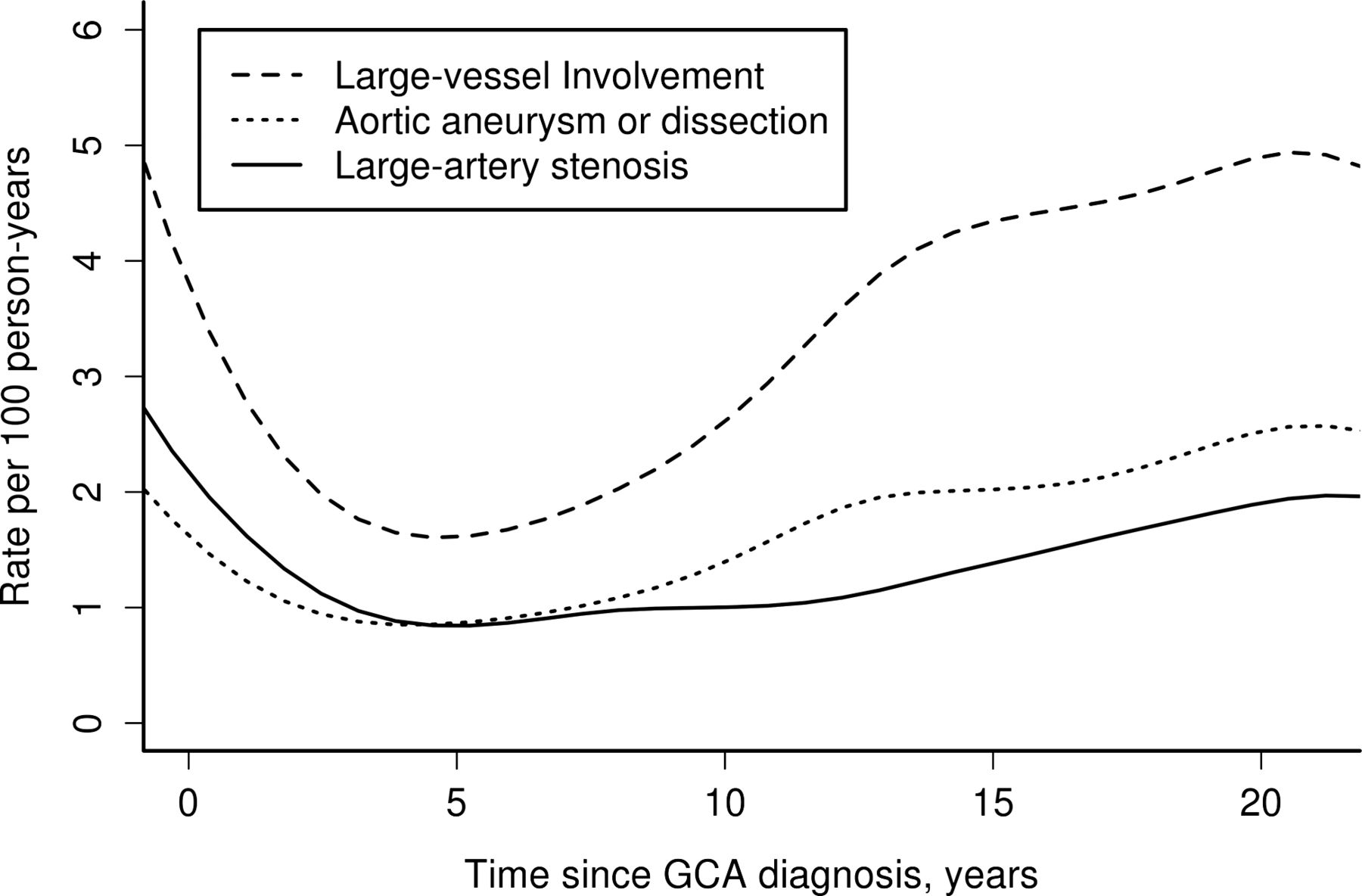
The incidence of LV disease by follow-up from diagnosis of GCA is depicted in figure 1. The rate of occurrence of any LV disease was high within the first year of GCA incidence (five events per 100 person-years). The incidence of LAS remained relatively constant beyond 5 years from diagnosis of GCA (p value for trend=0.77) but the incidence of aortic aneurysm/dissection increased after 5 years (p value for trend=0.009).

Incidence rates of large-vessel involvement by disease duration in patients with giant cell arteritis (GCA).
Survival in patients with GCA compared with the general population
There were 154 deaths. Overall survival for the cohort of 204 patients with GCA was similar to that expected in the general population (log-rank p=0.25). Cause-specific mortality in patients with GCA compared with the general population is shown in table 3.
Cause-specific mortality compared with the general population in the cohort of patients with GCA diagnosed between 1950 and 2004, and, cause-specific mortality compared with the general population in the subset of patients with GCA and aortic manifestations*
Patients with GCA who developed any LV involvement had decreased survival compared with the general population (log-rank p<0.001). Although survival in patients with LAS was similar to that expected in the general population, patients with aortic aneurysm/dissection had a significantly reduced survival (figure 2). Evaluation of cause-specific mortality in patients with GCA and aortic aneurysm/dissection showed an excess mortality attributed to the circulatory system compared with the general population (table 3).

{kind=link}
{kind=link}
Survival in patients with giant cell arteritis (solid line) who develop large-artery stenosis (LAS) (top panel) log-rank p=0.11, or, aortic aneurysm/dissection (AA/AD) (bottom panel) compared with the general population (dotted line), log-rank p<0.001.
Influence of LV manifestations on survival among patients with GCA
Among patients with GCA, LV manifestations were associated with increased mortality compared with patients with GCA without LV involvement (HR=2.4; 95% CI 1.6 to 3.6). Aortic aneurysm/dissection was associated with increased mortality (HR=3.4; 95% CI 2.2 to 5.4). The mortality in patients with GCA and LAS was similar to that in patients with GCA without this manifestation (HR=1.5; 95% CI 0.9 to 2.5).
Time-trends in mortality were evaluated in patients with LV manifestations and showed no difference in mortality for patients diagnosed with GCA between 1950 and 1979 compared with those diagnosed between 1980 and 2004 (table 4).
Time-trends in mortality in patients with GCA and large-vessel manifestations comparing those diagnosed with GCA between 1980 and 2004 with those diagnosed between 1950 and 1979
Discussion
LV manifestations (LAS, aortic aneurysm/dissection) were common in patients with GCA and increased over the observation period, probably related to the increased use of imaging modalities. The incidence of aortic aneurysm/dissection increased 5 years after diagnosis of GCA and continued to increase throughout the follow-up. The overall survival of patients with GCA was similar to that of the general population. However, aortic aneurysm/dissection was associated with reduced survival in patients with GCA. Compared with the general population, patients with aortic aneurysm/dissection had an excess mortality attributed to cardiovascular and pulmonary causes.
We observed an increased incidence of LV manifestations in patients with GCA. However, the use of CT, MRI, abdominal ultrasonography and echocardiography also increased for the cohort diagnosed with GCA after 1980 compared with those diagnosed in the earlier decades. This observation may account for the increased incidence of LV manifestations rather than a change in disease expression over time. Additionally, greater physician awareness of the extracranial manifestations of GCA over the study period might have led to an increased use of imaging to evaluate for LV disease. Although the numbers were small, surprisingly, the incidence of aortic dissection remained fairly stable in this cohort for the different time periods analysed. Pre-existing aortic aneurysm is a risk factor for aortic dissection. With the increased use of imaging modalities over the decades and the increased detection of aortic aneurysms, one might have expected aortic dissection to decrease over time. One possibility is that the detection of an aneurysm did not alter the management of the patient. Alternatively, the increased use of more sensitive imaging modalities (echocardiography, CT, MRI) in patients diagnosed in the latter decades might have resulted in the detection of aneurysms at a smaller size. If aortic size is a predictor of dissection in GCA, the smaller size at detection may explain why no increase in aortic dissections was seen despite the increased incidence of aortic aneurysms. It remains unclear whether patients with GCA differ from patients with non-inflammatory aortic aneurysms, where size and rate of growth of the aneurysms appear to be major factors in risk of rupture.24
Transient ischaemic attack or stroke, smoking (ever) and presence of a vascular bruit at diagnosis were the only factors associated with LAS in this study, whereas coronary artery disease (CAD) was associated with an increased risk of aortic aneurysm/dissection. The only other population-based study evaluating predictors of aortic aneurysm/dissection in GCA did not evaluate CAD and its association with this manifestation.25 The mechanism underlying the increased risk of aortic aneurysm/dissection in patients with GCA who have CAD is unclear. A common underlying pathogenic process such as atherosclerosis may be responsible. However, traditional cardiovascular risk factors such as hypertension, hyperlipidaemia or smoking were not associated with an increased risk of aortic aneurysm/dissection in this study. While the association we observed may be spurious or due to chance, the magnitude is large and warrants further study.
A better understanding of the timing of LV events is clinically relevant. In a significant proportion of patients with newly diagnosed GCA the aorta (45–65%) and its branches (29–74%) was shown to be involved on imaging studies.4–9 Patients in our study did not undergo systematic screening. However, we found that the incidence of LV events was high within the first year of diagnosis of GCA. This suggests that disease may be present well before clinical detection. While the rate of LAS did not significantly increase after 5 years, the rate of aortic aneurysms/dissections increased 5 years after diagnosis of GCA and continued to increase during the entire period of observation. A smaller cross-sectional imaging study of 54 patients with GCA (median duration 5.4 years) showed evidence of aortic aneurysm or dilatation in 12 patients (22.2%); five of whom were candidates for surgical repair based on aneurysm size.26 These findings highlight the importance of long-term surveillance in patients with GCA to monitor for aortic aneurysm formation.
Overall survival in our cohort of patients with GCA was similar to that in the general population, a finding that has been reported in previous studies.10–16 While a few studies have reported increased mortality in patients with GCA,27–30 they usually included small numbers of patients with GCA. An analysis of cause-specific mortality found an excess of death attributable to the gastrointestinal system. The numbers were small, but the increased number of deaths due to mesenteric vascular disease in our cohort was unexpected. Mesenteric arteritis from GCA has not commonly been diagnosed, but may be under-recognised clinically.31–34 Imaging studies have described the involvement of the mesenteric arteries in 18% (cross-sectional study) and 22% (newly diagnosed) of patients with GCA.8 ,35
A previous study from this cohort did not find any increase in mortality in patients with GCA and LV manifestations with the exception of those who developed aortic dissection.1 The analysis in the previous study compared patients in the different subgroups of LV involvement from the time of diagnosis of GCA.1 However, as our data show, LV events are detected months to years after the initial GCA diagnosis which was not accounted for by the previous analysis as patients in the different groups could not experience the outcome of death until after they developed LV manifestations.
In our study, we used Cox regression models with time-dependent covariates which allowed patients with GCA to be modelled as unexposed to the risk factor (ie, LV manifestations) until they developed the LV event. Contrary to the previous report, we found that patients with GCA and aortic manifestations had a 3.4-fold increased risk of death compared with patients with GCA without LV manifestations. Our study also comprehensively evaluates survival and cause-specific mortality in patients with GCA and LV involvement. Survival compared with the general population was also decreased in patients with GCA and LV manifestations. In these patients increased numbers of deaths were found to be attributable to the cardiovascular and respiratory systems. Since aortic dissection is a dreaded complication of aortic aneurysms and is often catastrophic, the greater than expected number of deaths from cardiovascular causes is not entirely surprising. However, patients with aortic manifestations from GCA also had a greater than expected number of deaths from ischaemic heart disease and non-ischaemic cardiac disease. Conceivably, the aortic inflammation in GCA and atherosclerosis share common pathobiological pathways which may account for our observed association.36 ,37 It is also possible that the underlying cause of death in patients with aortic aneurysms was dissection but was misdiagnosed as another event such as a coronary event, which is common in the elderly. While there were also a higher than expected number of deaths from respiratory causes, the reason for this is unclear and might be related to the small number of cases.
Since the cohort spans several decades, during which medical practice has changed, time-trends in mortality were evaluated in patients with LV manifestations. Overall, there were no differences in mortality between the two cohorts. One might expect that aggressive modification of cardiovascular risk factors, changes in practice including the serial imaging of patients with aneurysms and surgical intervention might have resulted in improved survival in patients with aortic aneurysms and dissections in recent decades but this was not supported by our data, although the total number of events was low.
The strengths of our study include the population-based incident cohort of patients with GCA. We had access to the entire medical record from all providers in Olmsted County, which allowed more complete data collection. Since our primary outcome was death, vital status for each subject regardless of residency status was collected. We also had access to the death certificates for 98% of patients who died (data missing only in three patients). According to the 2000 US census data, 90.3% of the Olmsted County population is White. Since GCA predominantly affects individuals of Northern European descent, our population is representative of patients with this disease.
Limitations include the retrospective design. As is the case in current clinical practice, not all patients were systematically screened for development of LV disease, which might have resulted in misclassification of patients. Additionally, given this limitation, we were only able to evaluate complications of LV disease including LAS and aortic aneurysm/dissection. Using death certificates to determine the underlying cause of death has its limitations. Census data for the Minnesota population were available for the years 1979 through 2002 and were extrapolated for the missing years. A separate analysis using only the cohort diagnosed between 1979 and 2004 did not change our findings.
Our findings have important clinical implications for the care of patients with GCA. Since aortic aneurysm/dissection is associated with decreased survival, screening for aortic aneurysm formation is important. The incidence of aortic aneurysm/dissection increased 5 years after GCA diagnosis and continued to increase over the period of observation, emphasising the need for long-term surveillance of these patients. Patients with GCA and aortic manifestations had excess deaths from cardiovascular causes including ischaemic heart disease in patients with aortic aneurysm/dissection. A better understanding of the mechanisms of aortic complications in GCA, and optimal imaging strategies for detecting them, would provide useful information and might help to guide future decisions about the care of these patients. Prospective studies of the cost-effectiveness of screening and whether they translate into improved survival for patients with GCA are needed.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online table
Footnotes
-
Handling editor Tore K Kvien
-
Contributors All authors were involved in the study conception and design, acquisition of data or analysis and interpretation of data. All authors made significant contributions to drafting the article or revising it critically for important intellectual content and all authors approved the final version of the submitted manuscript. We also confirm that there is no person who fulfils the criteria for authorship who has not been included as an author.
-
Funding This project was supported by NIH/NCRR CTSA grant number UL1 RR024150. Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the NIH. This study was made possible by the Rochester Epidemiology Project (grant number R01 AG034676 from the National Institute on Aging. TAK was supported by the Vasculitis Clinical Research Consortium (VCRC) which has received support from the National Institute of Arthritis and Musculoskeletal and Skin Diseases (U54AR057319), the National Center for Research Resources (U54 RR019497) and the Office of Rare Diseases Research. The VCRC is part of the Rare Diseases Clinical Research Network (RDCRN).
-
Competing interests None.
-
Ethics approval Institutional review boards at Mayo Clinic and Olmsted Medical Center.
-
Provenance and peer review Not commissioned; externally peer reviewed.