Article Text

Abstract
Objective Studies on the association between rheumatoid arthritis (RA) and deep vein thrombosis (DVT) and pulmonary thromboembolism (PE) are scarce. This study identifies the effects of RA on the risks of developing DVT and PE in a nationwide prospective cohort study.
Methods We studied the entire Taiwan population from 1998 to 2008, with a follow-up period extending to the end of 2010. We identified patients with RA using the catastrophic illness registry of the Taiwan National Health Insurance Research Database (NHIRD). We also selected a comparison cohort that was randomly frequency-matched by age (each 5-year span), sex and index year from the general population. We analysed the risks of DVT and PE using Cox proportional hazards regression models, including sex, age and comorbidities.
Results From 23.74 million people in the cohort, 29 238 RA patients (77% women, mean age of 52.4 years) and 1 16 952 controls were followed 1 93 753 and 7 92 941 person-years, respectively. The risk of developing DVT and PE was 3.36-fold and 2.07-fold, respectively, in patients with RA compared with patients without RA, after adjusting for age, sex and comorbidities. The multiplicative increased risks of DVT and PE were also significant in patients with RA with any comorbidity.
Conclusions This nationwide prospective cohort study demonstrates that DVT and PE risks significantly increased in patients with RA compared with those of the general population.
- Epidemiology
- Rheumatoid Arthritis
- Outcomes research
Statistics from Altmetric.com
Introduction
Deep vein thrombosis (DVT) is the formation of blood clots in the deep veins, with thrombus predominantly occurring in the legs. It is a serious condition, known as post-thrombotic syndrome that can cause permanent damage to the leg. Pulmonary thromboembolism (PE) is a potentially life-threatening disorder. Together, DVT and PE constitute venous thromboembolism (VTE). VTE is not a benign disease, and has a 30-day case fatality rate of 11–30%.1–4 Atherothrombosis and VTE share common risk factors and pathophysiological characteristics of inflammation, endothelial injury and hypercoagulability.
Rheumatoid arthritis (RA) is a progressive disease involving the chronic and abnormal inflammatory reaction of the immune system against body tissues, leading to joint destruction and several systemic manifestations. Most studies on RA focus on the prevention and control of joint damage and an improvement in quality of life.5–8 Several studies have shown that chronic inflammation is connected with prothrombotic factors and endothelial dysfunction in the development of atherothrombosis in patients with RA.9–11 However, RA is not generally viewed as a risk factor for DVT and PE, although patients with RA may exhibit some abnormalities of coagulation factors. Research on the association between RA and DVT/PE is limited. Studies on the association between RA and DVT/PE are scarce.12–14 We conducted a nationwide RA cohort prospective study to investigate whether RA increases the risks of DVT and PE.
According to the American College of Rheumatology (ACR; formerly the American Rheumatism Association) 1987 criteria for RA diagnosis, RA is defined by the presence of four or more of the following criteria15: (1) morning stiffness in and around joints lasting at least 1 h before maximal improvement; (2) soft tissue swelling (arthritis) of three or more joint areas observed by a physician; (3) swelling (arthritis) of the proximal interphalangeal, metacarpophalangeal, or wrist joints; (4) symmetric swelling (arthritis); (5) rheumatoid nodules; (6) the presence of a rheumatoid factor; and (7) radiographic erosions or periarticular osteopenia in hand or wrist joints. The ACR and European League Against Rheumatism (EULAR) published revised classification criteria focusing on features at earlier stages of the disease in 2010.16
Methods
Taiwan launched a single-payer compulsory National Health Insurance (NHI) programme in 1995. This programme covers over 99% of the population of Taiwan (23.74 million people).17 The NHI programme is primarily financed through premiums, and is supplemented with user fees, copayments and direct government funding. We studied the entire Taiwan population from 1998 to 2008, with a follow-up period extending to the end of 2010.
Data source
Data files from Taiwan National Health Insurance Research Database (NHIRD) contain registration files and original claims data for reimbursement. Previous studies have discussed information linking in these files.18 All data are anonymous and deidentified by scrambling the identification codes to make the NHI reimbursement data suitable for public research. The International Classification of Disease, Ninth Revision (ICD-9) was used for the diagnosis codes. Several Taiwan studies had demonstrated the high accuracy and validity of ICD-9 diagnosis in NHIRD.19 ,20
Study participants
Diagnoses associated with hospitalisation were coded according to the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM). In Taiwan, the rheumatologists can apply for the catastrophic illness card for any patient with RA, who fulfils the presence of four or more diagnostic criteria based on the 1987 ACR criteria. The application of the catastrophic illness card should be scrutinised by peer review. The patients with RA with a catastrophic illness card can be exempt from paying a copayment. We used the Registry for Catastrophic Illness Patient Database (RCIPD) to identify RA (ICD-9-CM 714) patients in the claims data, and the first-time RA diagnosis served as the index date from 1998 to 2008. We excluded patients with a history of PE (ICD-9-CM 415.1), iatrogenic PE (ICD-9-CM 415.11) and DVT (ICD-9-CM 453.8) before the index date, and those with incomplete age or sex information. The patients with RA and comparison controls were frequency matched in a 1:4 ratio on age (each 5-year span), sex and index year. Outcome variables included the development of DVT or PE during the follow-up period. Almost all patients with DVT or PE had their comprehensive examination before receiving intensive care. In Taiwan, DVT and PE patients’ medical reimbursement and discharge notes are scrutinised by peer review. Pre-existing comorbidities for each participant included atrial fibrillation (ICD-9-CM 427.31), hypertension (ICD-9-CM 401-405), diabetes (ICD-9-CM 250), hyperlipidaemia (ICD-9-CM 272), cerebral vascular disease (ICD-9-CM 430-438), heart failure (ICD-9-CM 428), lower leg fracture or surgery (ICD-9-CM 820, 821, 823, 81.51, 81.52, 81.53, 81.54), and all cancer types (ICD-9-CM 140-208). We also estimated whether participants had any of these comorbidities.
Statistical analysis
The follow-up person-years at the end of 2010 were calculated for each participant until the diagnosis of DVT or PE, withdrawal from the insurance system, censored because of death, or loss to follow-up. We analysed and stratified participants whose ages were <50, 50–65 and >65 years based on the RA index date. We used a χ2 test between the cohort with RA and the comparison cohort to determine the differences in categorical demographic variables and comorbidities, and measured and tested the mean age between both cohorts by using the t test. We also calculated the incidence densities (per 10 000 person-years) by demographic variables for each cohort, and calculated the RA-to-comparison cohort rate ratio of developing DVT or PE and 95% CIs for each variable. To compare the risk of incident DVT and PE between patients with RA and the comparison cohort, we used Cox proportional hazards regression models to calculate the HRs adjusted for age, sex and comorbidities. We further assessed the effects of RA duration by using time-dependent covariates (<4, 4–8 and >8 years since RA diagnosis). We used the Kaplan–Meier method to estimate the failure functions of DVT or PE between the cohort with RA and the comparison cohort, and assessed the differences using a log-rank test. All analyses were conducted using SAS statistical software (V.9.2 for Windows; SAS Institute, Cary, North Carolina, USA), and all statistical tests were performed at the two-tailed significance level of 0.05.
Results
Characteristics of the study participants
We identified 29 238 patients with newly diagnosed RA, from 1998 to 2008 as the exposure cohort, and 116 952 participants without any RA diagnosis as the comparison cohort (table 1). The cohort with RA and the comparison cohort showed no significant differences based on distributions of sex and age. Both cohorts included more women than men (77% vs 23%). Approximately 22% of the participants were older than 65 years of age. Patients with RA had a higher prevalence of pre-existing comorbidities in hypertension, diabetes, hyperlipidaemia, heart failure and lower leg fracture or surgery (p<0.0001).
Demographic characteristics and comorbidity in patients with and without rheumatoid arthritis
Incidence rate ratios of DVT and PE
During 193 753 and 792 941 person-years follow-up, the overall incidence density of DVT was significantly higher in patients with RA than in the comparison cohort (10.70 vs 3.22 per 10 000 person-years). The overall RA cohort-to-comparison cohort incidence rate ratio (IRR) of DVT was 3.34-fold (95% CI 3.22 to 3.46). The overall incidence density of PE was also significantly higher in patients with RA than in the comparison cohort (3.60 vs 1.75 per 10 000 person-years). The overall RA cohort-to-comparison cohort IRR of PE was 2.06-fold (95% CI 1.97 to 2.14). Results show that RA had the greatest effect on developing DVT and PE in young adults compared with middle-aged adults and older adults (IRR=5.84 for DVT and IRR=3.54 for PE). Regardless of the participants’ comorbidities, RA patients had a higher IRR of DVT and PE than the comparison cohort (table 2).
Comparison of incidence and HR of DVT and PE between patients with and without rheumatoid arthritis, stratified by sex, age and the presence of comorbidity
Hazard ratios of DVT and PE
After adjusting for age, sex and comorbidities, patients with RA had a 3.36-fold increased risk of developing DVT compared with the comparison cohort (adjusted HR=3.36, 95% CI 2.79 to 4.03). After adjusting for age, sex and comorbidities, patients with RA also had a 2.07-fold greater risk of developing PE compared with the comparison cohort (adjusted HR=2.07, 95% CI 1.55 to 2.76). In female participants, patients with RA had an increased risk of DVT or PE than non-RA comparisons (aHR=3.58, 95% CI 2.90 to 4.40 for DVT; aHR=2.20, 95% CI 1.60 to 3.03 for PE). The age-stratified effect of RA on DVT or PE was the highest in subjects aged 50 years or less (aHR=5.55, 95% CI 3.40 to 9.07 for DVT; aHR=3.13, 95% CI 1.26 to 7.77 for PE). The association between RA and the risk of DVT or PE was observed among participants without any comorbidity (aHR=3.75, 95% CI 3.00 to 4.68 for DVT; aHR=2.58, 95% CI 1.79 to 3.70 for PE) (table 2).
Interaction between RA and any comorbidity
Table 3 shows that the multiplicative risks of developing DVT and PE in patients with RA increased with the presence of any comorbidity.
Cox proportional hazard regression analysis for the risk of rheumatoid arthritis-associated DVT and PE with interaction of comorbidity
DVT in relation to time since RA diagnosis
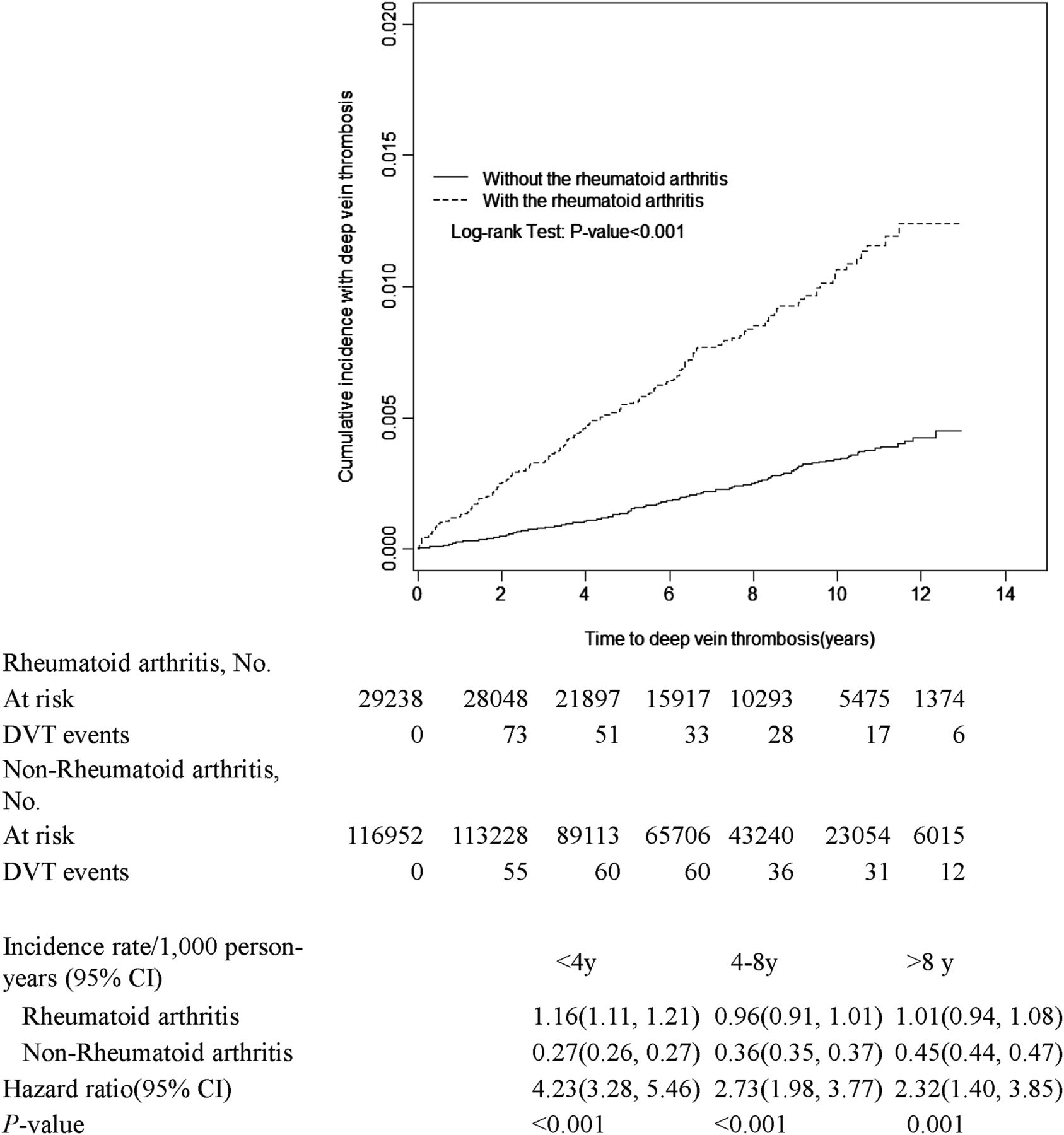
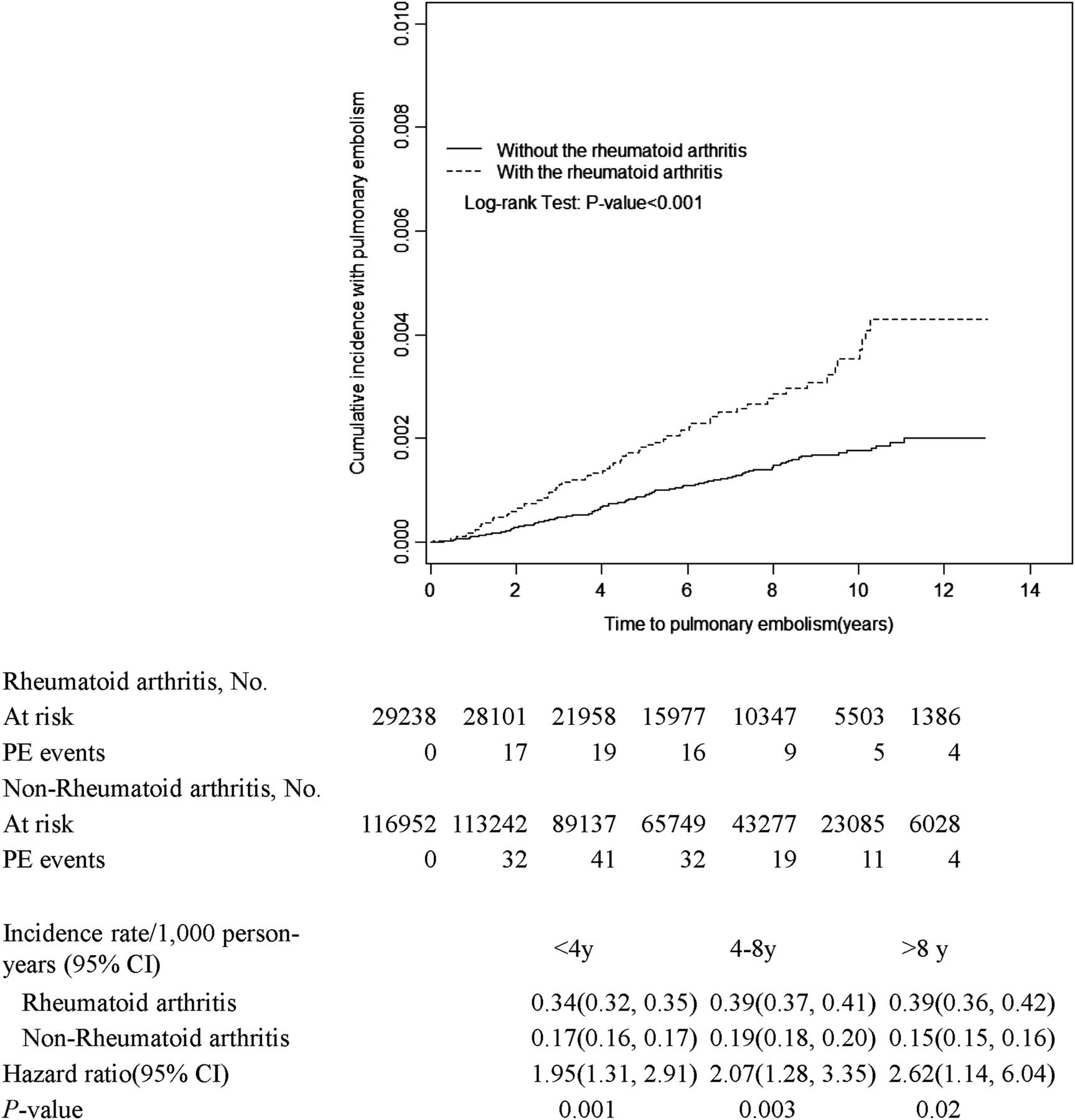
The analysis of these cohorts stratified by time since RA diagnosis shows higher incidence rates of DVT in patients with RA compared with those of the comparison cohort within 4 years since RA diagnosis, with adjusted HR, 4.23 (95% CI 3.28 to 5.46); p value <0.0001) (figure 1). The incidence rate of DVT decreased over time. When stratifying by time since RA diagnosis, the incidence rates of PE were also higher in patients with RA than those in the comparison cohort within 4 years since RA diagnosis, with adjusted HR, 1.95 (95% CI 1.31 to 2.91); p value <0.0001) and increased over time (figure 2). We have also conducted sensitivity analysis and found increased risks of DVT and PE during various follow-up periods (table 4).
Effects of RA on the risks of DVT and PE, during various follow-up periods

Failure functions of deep vein thrombosis (DVT) in patients with rheumatoid arthritis and comparison patients.

{kind=link}
{kind=link}
Failure functions of pulmonary embolism (PE) in patients with rheumatoid arthritis and comparison patients.
Discussion
Previous research showed that RA affects 0.1% of the population in Taiwan, which is lower than the 0.5–1% rate in Western countries.21 ,22 We found 3.36-fold and 2.07-fold increased risks of developing DVT and PE, respectively, in patients with RA compared with the general population. Kang et al23 estimated the relationship between DVT and RA by using a case-control study, and found a 1.88-fold increased risk of DVT associated with an RA history. However, a case-control study has difficulty obtaining reliable information about an individual's exposure status over time. Matta et al used hospitalisation data to identify the association between RA and VTE. However, this approach may modify the result of patients at elevated risks of other causes, preventing a complete understanding of the effects of RA on VTE.12 Holmqvist et al13 and Choi et al14 conducted population-based cohort studies to investigate RA, showing a 2.0-fold to 2.2-fold increased risk of VTE in Western countries. This study uses a nationwide prospective cohort study to delineate RA and increased risk of DVT and PE in Taiwan. The RA with increased risk differences of DVT and PE between this study and studies on Western countries may be associated with racial differences.
We enrolled patients with RA from the catastrophic illness registry of the Taiwan NHIRD. The diagnosis of these patients is strictly based on the 1987 ACR criteria and maybe identified at a later stage. This might explain why DVT risk significantly increased in the first 4 years of RA diagnosis. Our finding regarding association between RA and the risk of VTE is consistent with the study reported by Holmqvist et al.13 Nevertheless, our study further analysed DVT and PE separately and suggested that DVT risk significantly increased in the first 4 years of RA diagnosis, while the rate of PE was higher over 4–8 and >8 years after RA diagnosis. DVT patients might subsequently develop PE, which might explain this discrepancy. Additionally, the risk of developing PE progressively increased with follow-up periods, which could be associated with RA disease and also aging process.24
Although the patients with RA in this study had a higher prevalence of comorbidities and coexistent conditions associated with the development of VTE than the comparison cohort, RA remains an independent risk factor for developing DVT and PE after adjusting for covariates. Virchow proposed the pathogenesis of VTE based on a triad of causes: alteration in blood flow (stasis), vascular endothelial injury, and changes in the blood (hypercoagulable status). The decreased mobility caused by RA could also affect venous stasis because RA is a chronic systemic inflammatory disorder. The inflammation mediators connected with prothrombotic factors and endothelial dysfunction are involved in the development of atherosclerosis and thrombosis.9 ,25–27 Common proinflammatory cytokines and inflammatory mediators also appear in the development and progression of both RA and atherosclerosis.27 Increased C-reactive protein (CRP) levels in patients with RA support the presence of chronic inflammation. A high CRP indicates a rapid increase in viscosity caused by the conversion of fibrinogen to fibrin, which may explain the increase in the risk of a postoperative thromboembolism.28
Most RA patients were women, and DVT and PE risks increased in both sexes with RA. However, this study did not show significant association between RA and risk of PE in male participants after adjusting for age and comorbidities, which is consistent with previous studies.29 ,30 The age-stratified effect of RA on DVT or PE development was the highest in subjects aged 50 years or less. However, the incidence rate of developing DVT and PE increased with age in patients with RA and non-RA cohort, which is consistent with previous studies.13 ,31 ,32 As people age, they become less active, and their cardiopulmonary systems slow down. This phenomenon contributes to DVT by developing blood stasis and clots in the deep veins. Recent studies show that frailty, which is commonly associated with aging, can activate coagulation and inflammatory pathways.32 ,33
This study shows that the incidence rates of DVT and PE increased in patients with any comorbidity in both cohorts. The increased risk of developing DVT and PE was also significant in patients with concomitant RA and any comorbidity. These results are robust using Cox proportional-hazards regression analysis for the increased risks of DVT and PE in RA with interaction of any comorbidity (table 3). Therefore, providing adequate care for patients with RA with comorbidities is an important step in preventing further development of DVT and PE. Thus, a multidisciplinary team should guide the assessment, treatment and holistic care of patients with RA.34 ,35
The highest risk of developing DVT appeared in the first years of RA diagnosis. This phenomenon may be associated with RA identification at a later stage strictly based on the 1987 ACR diagnostic criteria used in Taiwan. The ACR and EULAR have posited revised classification criteria to focus on features at earlier stages of RA in 201016 which may be helpful to identify patients who may benefit from early effective intervention.
The strength of this study is that it provides a nationwide population-based cohort longitudinal study on the risk of DVT and PE development in Asian people with RA. These findings can be generalised to the general population. However, several limitations must be considered when interpreting these findings. The NHIRD does not provide detailed lifestyle information, such as smoking, body mass index and physical activity, all of which are potential confounding factors for this study. Although the RA treatment and lifestyle modification of RA patients may benefit from physical inactivity and obesity, no clear evidence implicates these factors in accelerated atherosclerosis in RA.36 Additionally, information on RA severity scale, such as disease activity, functional impairment and physical damage was unavailable in our data. The lack of drug data, such as hormone replacement therapy, anticonceptive drugs, and glucocorticosteroids to adjust for the outcomes of interest could be another limitation. Despite our meticulous study design in controlling confounding factors, a key limitation of this study is the potential for bias caused by possible unmeasured or unknown confounders.
In conclusion, this nationwide study of approximately 30 000 patients with RA with 193 753 follow-up person-years shows that patients with RA have 3.36-fold and 2.07-fold increased risks of developing DVT and PE compared with the general population. These findings highlight the importance of a multidisciplinary team adopting an integrated approach to the intervention of potential risk factors among patients with RA. Future research concerning RA severity scale, such as disease activity, functional impairment and physical damage are warranted.
References
Supplementary materials
Press release
Files in this Data Supplement:
Footnotes
-
Handling editor Tore K Kvien
-
Correction notice This article has been corrected since it was published Online First. ‘per 1000 person-years’ has been amended to read ’per 10 000 person-years’. Reference 16 has also been updated.
-
Contributors These authors’ individual contributions were as follows. Conception and design: W-SC and C-HK. Administrative support: C-LP, C-LL, F-CS and Y-JC. Collection and assembly of data: All authors. Data analysis and interpretation: W-SC, C-LP, C-LL, Y-JC and C-HK. Manuscript writing: All authors. Final approval of manuscript: All authors.
-
Funding The study was supported by grants from the study hospital (DMR-102-014 and DMR-102-023); Taiwan Department of Health Clinical Trial and Research Center and for Excellence (DOH102-TD-B-111-004), Taiwan Department of Health Cancer Research Center for Excellence (DOH102-TD-C-111-005); and International Research-Intensive Centers of Excellence in Taiwan (I-RiCE) (NSC101-2911-I-002-303).
-
Competing interests None.
-
Ethics approval This study was exempted by the Institutional Review Board of China Medical University (CMU-REC-101-012).
-
Provenance and peer review Not commissioned; externally peer reviewed.