Article Text

Abstract
Objectives Accelerated cardiovascular morbidity and mortality occur in patients with rheumatoid arthritis (RA). We evaluated the presence, burden and compositional differences of coronary plaque in patients with RA without symptoms or diagnosis of coronary artery disease (CAD) compared against controls.
Methods One hundred and fifty patients with RA and 150 matched controls underwent 64-slice CT angiography (CTA) for evaluation of coronary plaque. Numbers of segments with plaque per patient (Segment involvement score (SIS)), degree of segment stenosis (stenosis severity score (SSS)), plaque size (plaque burden score (PBS)), and composition were assessed using a standardised American Heart Association 15-segment model. Lesions were classified as non-calcified plaque (NCP), mixed (MP), and fully calcified plaque (CP).
Results Higher proportion of patients with RA had plaque when compared with controls (71% vs 45%, p<0.0001); 13.5% of total RA segments harboured plaque compared with 6% in controls (p<0.0001), and all plaque types were higher (p<0.001). Multivessel disease, both non-obstructive and obstructive, was more prevalent, and quantitative measures of stenotic plaque severity (SSS) and extent (PBS) were higher in RA, even after adjustments for cardiac risk factors (p<0.01 for all). A steeper progression of plaque with age was seen in RA. Disease activity associated only with presence of NCP and MP, whereas patient age was the only predictor of fully CP.
Conclusions RA patients without CAD have higher prevalence, extent, and severity of all types of coronary plaque. Residual disease activity associates with presence of higher risk NCP and MP potentially contributing to future adverse cardiac events.
- Rheumatoid Arthritis
- Atherosclerosis
- Cardiovascular Disease
Statistics from Altmetric.com
Introduction
Individuals with rheumatoid arthritis (RA) experience a higher rate of cardiovascular events compared with controls.1 Coronary artery disease (CAD) accounts for about half of all deaths in RA,2 occurs early,3 ,4 and may precede its clinical diagnosis.5 Early mortality after acute coronary syndrome (ACS) is higher and recurrent events or death is more likely in RA than age and gender-matched controls.6 ,7 This accelerated risk transcends cardiac risk factors (CRF) and may reflect the high inflammatory state in this condition.8
The role of inflammation on progression of atherosclerosis and plaque destabilisation is increasingly appreciated.9 Therefore, the higher frequency of cardiovascular events in RA could represent either accelerated formation of coronary plaque or higher susceptibility of such plaque to rupture (vulnerable plaque), or both.2 In fact, higher plaque vulnerability has been reported in patients with RA with established CAD compared with controls,10 and vulnerability has been associated with inflammation and RA disease activity.11 However, the prevalence, burden, composition and progression of coronary plaque over time in RA, compared with controls are largely unknown.
CT angiography (CTA) is an imaging modality that accurately evaluates coronary plaque presence, burden, severity and composition in subjects without indication for invasive assessment. Detection accuracy approaches 100% in prospective assessments against conventional angiography and intravascular ultrasound.12–14 Moreover, CTA independently predicts short and long-term cardiac events in patients with suspected or established CAD,15–17 exhibiting incremental value over coronary artery calcium scores (CAC) for such outcomes.18 Its high reproducibility for quantitative measurements of coronary stenosis, plaque geometry and composition enables serial monitoring and assessment of changes as a result of therapy.19 ,20
In the present study, we used 64-slice CTA to prospectively evaluate potential differences in the presence, severity, and composition of coronary plaque in RA subjects compared with age and gender-matched controls that might provide mechanistic insights to their higher risk of future cardiac events.
Methods
Patient recruitment
One hundred and fifty patients from a single centre were enrolled and prospectively evaluated between 1 March 2010 and 1 March 2011. An equal number of age (±1 year) and gender-matched individuals without known systemic autoimmune disease served as controls. The study was approved by the local institutional review board and all the individuals signed informed consents.
Inclusion criteria comprised ages ≥18 years, fulfilment of 1987 American College of Rheumatology (ACR) criteria for RA, and no prior documentation of CAD, such as myocardial infarction or revascularisation. Similarly, the controls had no established CAD and were studied in a similar time frame (2009–2011); the majority enrolled as part of general routine health evaluation (self-referral). Alternatively, control subjects were referred for evaluation due to presence of ≥1 CRFs, electrocardiographic abnormalities, or report of atypical chest pain. Exclusion criteria comprised: concomitant autoimmune syndromes, weight over 148 kg, uncontrolled tachycardia, irregular rhythm and active malignancy. Patients were also excluded for known iodine allergy, creatinine >1.4 mg/dL, or GFR <60 mL/min.
Demographics and laboratory evaluation
Hypertension was defined as documented history of high blood pressure (BP), current antihypertensive use, or SBP ≥ 140 mm Hg or DBP ≥ 90 mm Hg measured twice at the day of the scan; resting BP was measured twice in the seated position after a 5 min rest period using a Dinamap model Pro 100 automated oscillometric sphygmomanometer (Critikon, Tampa, Florida, USA) and the average of the readings was recorded. Diabetes mellitus (DM) was defined as documented history of DM, and/or use of hypoglycaemic medications. Hyperlipidaemia was diagnosed as fasting cholesterol >200 mg/dL (>5.2 mmoles/L), and/ or plasma LDL>130 mg/dL (>3.4 mmoles/L). Current smoking entailed cigarette consumption within the past 30 days. Positive family history was defined as presence of CAD in first-degree relatives younger than 55 years for men or 65 years for women. Disease duration, serologic status including rheumatoid factor (RF) and anticitrullinated peptide antibodies (ACPA), radiographs and treatments were verified. Disease activity was evaluated as disease activity score out of 28 joints (DAS28-CRP). Irreversible articular damage (IAD) defined as ankylosis, subluxation, arthrodesis or prosthesis was reported and joint replacement surgeries (JRS) were also tracked. Patients underwent laboratory assessments, including erythrocyte sedimentation rate (ESR) and high-sensitivity C-reactive protein (hs-CRP) at the time of CTA.
Multidetector CTA
Image acquisition
All CTA scans were performed with a 64-multidetector row Lightspeed VCT scanner (GE Healthcare) using a protocol identical to the ACCURACY trial21 and analysed by a single, experienced interpreter, blinded to subject identity (BMJ).
Image analysis
CAC was quantified by the Agatston method.22 Coronary arteries were evaluated using a standardised 15-segment model.23 Stenosis severity was scored from 0 to 4 based on grade of luminal restriction; one represented 1–29% stenosis, 2: 30–49%, 3: 50–69%, and 4: ≥70% stenosis. The area of each plaque visualised in at least two adjacent slices (slice thickness 0.625 mm) was determined on all affected slices. Plaque burden was graded from 0 to 3, defined as none (0), mild (1), moderate (2) and severe (3). Lesions rendering >50% stenosis were considered obstructive. In case of multiple plaques, the most stenotic one was assigned to the specific segment. Plaque consistency (see online supplementary figure S1) was determined as: (1) non-calcified plaque (NCP) (density lower than the contrast-enhanced lumen, identifiable in ≥2 planes; (2) calcified plaque (CP) (density greater than the contrast-enhanced lumen); and (3) mixed plaque (MP) (both non-calcific and calcific components within the same plaque).24 Segments harbouring NCP, MP and CP were recorded, as were those with obstructive lesions. Subjects received three individual quantitative scores25; segment involvement score (SIS) represented the total number of segments harbouring plaque (0–15); stenosis severity score (SSS) reported the average grade of stenosis conferred by plaque over all evaluable segments (0–60); plaque burden score (PBS) described the average grade of plaque size over all evaluable segments (0–45). Reproducibility of scoring measurements for our centre has been reported (see online supplementary text).25
Statistical analysis
Continuous variables were expressed as mean±SD (M±SD) or SE of the mean and categorical ones in absolute numbers and percentages. Mann–Whitney U, and Fisher's exact tests evaluated differences in baseline characteristics. Quantitative variations in plaque morphology between RA and controls were evaluated with analysis of variance. Logistic regression models, both crude and adjusted for all CRFs (age, gender, hypertension, diabetes, hyperlipidaemia, smoking and family history of CAD) evaluated prevalence risks of different plaque types in RA. Ordinal logistic regression models, both crude and adjusted for CRFs, evaluated risk of incremental plaque burden in RA versus controls. Finally, various clinical, structural, serologic and inflammatory RA parameters were evaluated for their ability to predict different plaque types in generalised linear models, both crude and adjusted for CRFs. Data was analysed with SAS V.9.2 (TS level 1M0).
Results
Baseline characteristics appear in table 1.
Baseline demographics and CRF distribution in RA and controls
Groups were well balanced, except for family history and hyperlipidaemia both of which were over-represented in the controls (p<0.0001); however, this imbalance did not influence the results of the study (see online supplementary text). Subjects were predominantly female, with chronic and robustly seropositive disease; erosive changes were present in 66% and patients were well controlled (DAS28-CRP=2.6±1). All individuals received disease-modifying anti rheumatic drugs (DMARD) and 85% were on Methotrexate. Prednisone was used in 35% (6.2±4 mg/day), and 60% of patients were exposed to Tumour Necrosis Factor-a inhibitors (TNFi).
Prevalence and quantitative assessments of coronary plaque in RA and controls
Non-contrast scans showed higher CAC in RA compared with controls (84±379 vs 3±11, p<0.0001, table 2); CAC>0 was greater in RA (37% vs 19%, p=0.005), even after adjustment for CRFs (OR=2.5, 95% CI 1.2 to 5.2, p=0.01- table 3), and mean scores in those subjects were higher than controls (230±602 vs 18±22, p=0.0002). On contrast scans, plaque presence was greater (71% vs 45%, p<0.0001) and multivessel disease, both obstructive and non-obstructive, was more prevalent in RA (p<0.0001, table 2 and figure 1A); non-obstructive 1, 2, and 3-vessel disease was present in 59%, 37% and 17% in RA, respectively, compared with 42%, 12% and 4% in controls. Obstructive 1, 2 and 3-vessel disease was present in 12%, 6.7% and 1.3%, respectively, in RA compared with 3%, 0.7% and 0% in controls. Similarly, more RA subjects had coronaries involved with NCP, MP and CP (57%, 27% and 22%, respectively, vs 38%, 11% and 11% in controls, figure 1B). Proportions of segments with various plaques were also higher compared to controls (p<0.001, figure 1C). All these differences remained significant after adjustments for traditional CRFs (table 3).
CTA results in RA and controls
Crude and adjusted models of plaque prevalence and burden
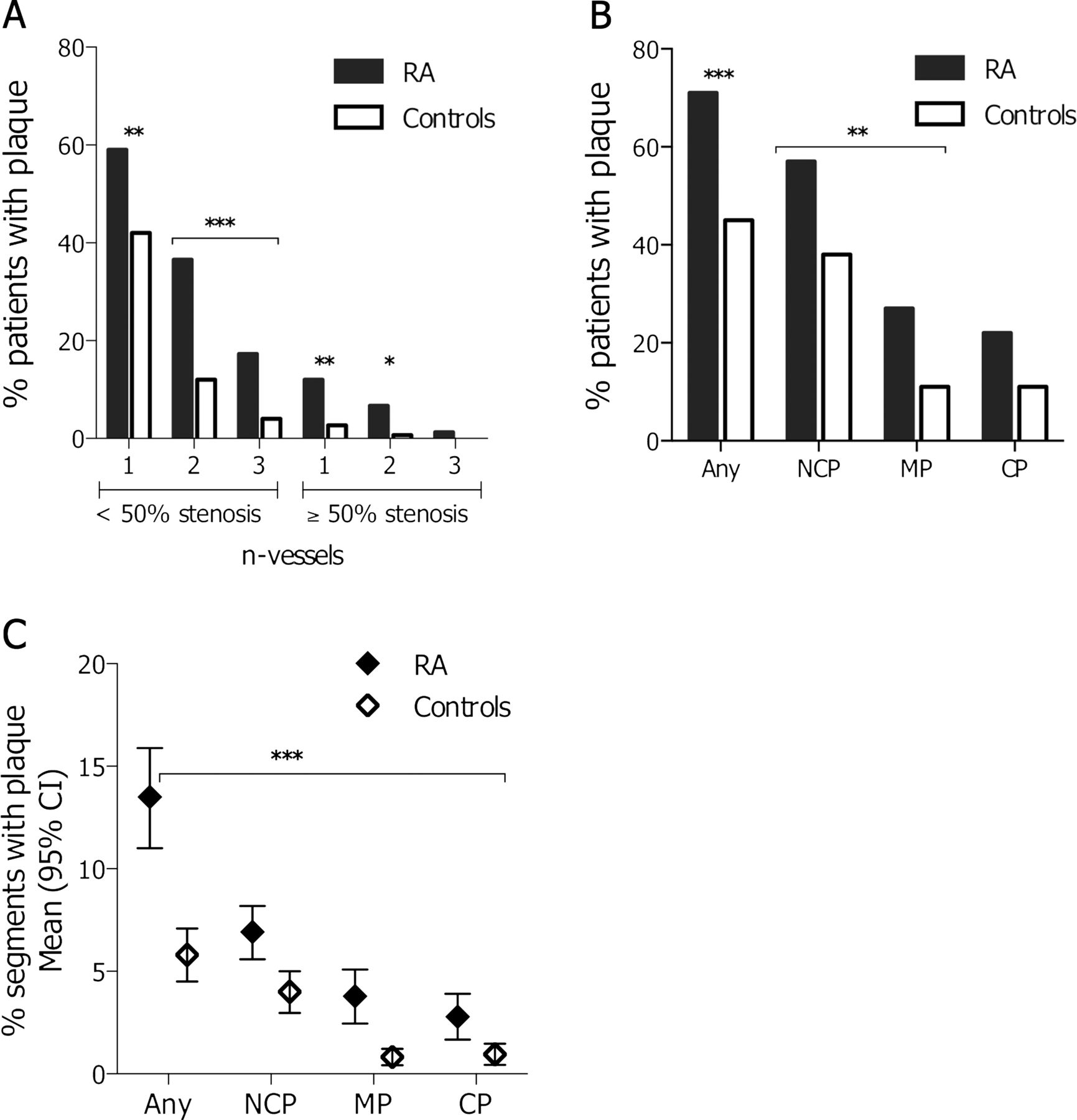
Per patient (panels A and B) and per segment (panel C) analysis of differences in coronary plaque presence and composition in RA and controls. A. Proportions of subjects with one, 2, or ≥3-vessel disease, both non-obstructive (<50%) and obstructive (≥50%); B. Number of patients with any, NCP, MP, or CP in RA and controls. C. Fraction of coronary segments harbouring any plaque, NCP, MP, or CP in RA and controls. Results in mean (95% CI). *p<0.05, **p<0.01, ***p<0.001 for all comparisons between RA and controls. RA, rheumatoid arthritis; NCP, non-calcified plaque; MP, mixed plaque; CP, calcified plaque.
All quantitative plaque scores (SIS, SSS and PBS) were higher in RA compared with controls (table 2); this was true for plaque at large (p<0.0001), as well as all individual plaque types (p<0.01). Importantly, RA subjects had greater risk for mild to moderate (1–2) and severe (3) plaque burden compared with controls, after adjustments for CRFs (table 3).
Effect of age and disease duration on plaque presence and composition in RA
Plaque presence increased with age in both RA and controls (figure 2A). Subjects 55–65 years and >65 years in both groups had higher proportions of segments harbouring plaque compared to those <45. These differences remained significant after adjustments for CRFs in both RA and controls (p<0.01 and p<0.05, respectively). However, RA individuals displayed a steeper increase in plaque with age; differences in involved segments between RA and controls were greater in subjects 55–65 years and >65 years compared to those <45. MP and CPs showed the greatest variation (figure 2C,D); differences in segments with MP between RA and controls were greater in subjects 55–65 years and >65 years vs those <45 years (p<0.01 and p<0.05). Similar observations held true for CP in RA subjects >65 years compared to controls (figure 2D).

{kind=link}
{kind=link}
Coronary segment involvement with various plaque types by age group (A–D) and disease duration (E). RA, rheumatoid arthritis; NCP, non-calcified plaque; MP, mixed plaque; CP, calcified plaque; *p<0.05, **p<0.01 vs controls <45 years; +p<0.05, ++p<0.01, +++p<0.001 vs RA patients <45 years; §p<0.05, §§p<0.01, §§§p<0.001 compared to the difference between RA and controls <45 years; ¶p<0.05 vs disease duration <5 years.
RA duration appears to incrementally affect coronary plaque (figure 2E); 8.1% (95% CI 3.2 to 13.1) of segments in subjects with <5 years of disease contained any plaque compared with 15.2% (95% CI 10.7 to 19.7) and 15.1% (95% CI 11.6 to 18.6) in those with 5–10 years or >10 years (p=0.04 and p=0.02, respectively). A similar trend persisted after multivariate adjustment for age, gender and CRFs for subjects with RA≥5 years (p=0.1), with age being a major confounder of the effect of disease duration on plaque presence. CP appeared more prevalent in individuals with RA>10 years (p=0.04), however, significance was lost after multivariable adjustments.
Impact of RA-specific parameters on coronary plaque composition
NCP and MP carry significantly higher risk of future cardiac events than CP.18 We therefore evaluated the contribution of individual RA parameters on the risk of having NCP and MP versus CP (table 4).
Determinants of coronary plaque consistency in rheumatoid arthritis
Age ≥55 years and moderate disease activity (DAS28-CRP≥3.2) significantly associated with the presence of NCP and MP (OR=2.9, 95% CI 1.0 to 8.8 and OR=4.5, 95% CI 1.4 to 14.4, respectively). Serological parameters, inflammatory indices, erosions, IAD and JRS were not predictive of such plaques. By contrast, age ≥55 years and perhaps to a lesser extent IAD associated with CP, suggesting that active clinical inflammation related preferentially to the more vulnerable NCP and MP, whereas damage accrual predominantly associated with lower-risk CP.
Discussion
Several reports have highlighted RA as an independent risk factor for MI.8 ,26 ,27 We hypothesised that potential differences in coronary plaque prevalence, burden, or composition may underlie such an accelerated risk. We used 64-slice CTA, a non-invasive, accurate and reproducible imaging modality to assess luminal anatomy, plaque morphology and consistency.
We observed that: (1) coronary artery calcification, overall CAC scores and mean scores in individuals with CAC>0 were significantly higher in RA, consistent with prior reports.28 ,29 (2) Patients with RA had a greater prevalence of coronary plaque, frequency of single and multi-vessel disease, both non-obstructive and obstructive. (3) Higher proportions of segments were occupied by all plaque types in RA, with NCP and MP accounting for the majority. (4) Quantitative measures of plaque involvement (SIS), stenotic severity (SSS) and burden (PBS) were greater in RA. (5) RA subjects displayed a steeper increase in plaque prevalence with age compared with controls predominantly affecting MP and CP. Longer RA duration (≥5 years) also associated with greater plaque prevalence risk, an effect largely confounded by age. (6) Residual clinical activity (DAS28-CRP≥3.2) associated with presence of higher-risk NCP and MP.
CAC improves prediction of cardiac events by CRFs in the general population.30 However, CP represents roughly 20% of total plaque volume and may not be present in earlier disease31; in our cohort, 71% of RA and 45% of controls had any plaque compared with 22% and 11%, respectively, with CP. Additionally, CP represented 23% and 14% of total plaque burden in RA and controls. In a CTA study of subjects with high suspicion for ACS, Henneman et al32 noted a 30% prevalence of obstructive CAD in patients with CAC=0. Coronary CTA additionally evaluates composition, stenotic severity and burden of plaque, improving upon the predictive value of CAC for future events (area under the curve (AUC) from 0.82 to 0.93, p<0.001).18
Our observation of higher occurrence of multivessel disease in RA (43% and 19% for 2 and ≥3 vessels vs 12% and 4% in controls) is concordant with prior angiographic reports.33 ,34 Most lesions were non-obstructive. In the CONFIRM study, such lesions were associated with higher mortality17; in another prospective study, 28% of subjects with suspected CAD and non-obstructive lesions suffered cardiac events at 52 months compared with 0% in those with no plaque.16 The above are also consistent with histologic observations that over two-thirds of ACS events are attributed to disruption of non-obstructive plaque.35 ,36 Additionally, SSS and SIS were predictive of cardiac events at 52 months16; 80% of subjects with SSS>5 had events compared to 15% with SSS≤5, and 75% with SIS>5 had events compared to 23% with SIS≤5. In our study, obstructive CAD, SSS>5 and SIS>5 were observed in 12%, 15% and 9% of subjects with RA, respectively, compared with 2.7%, 3.3% and 0.7% in controls (p<0.01 for all).
Plaque composition predicts both short and long-term outcomes; non-obstructive NCP and MP had HRs of 7.4 and 3.2 over CP for all-cause mortality at 8 years.37 Similarly, ≥2 segments with NCP, or ≥3 with MP had HR of 5 and 3.5 for cardiac events over 18 months.38 In another investigation of 4425 patients, 3-year major adverse cardiovascular event (MACE) was higher for MP (37.7%) and NCP (22.7%) than for CP (5%, p<0.001).18 In our study, 30% and 7.3% of patients with RA had ≥2 segments with NCP and ≥3 with MP, compared with 9.3% and 2.7% in controls (p<0.05). Lipid-laden plaques are considered most vulnerable, leading to subsequent clinical events.39 In ACS, NCP was always present in culprit lesions and very frequently absent in stable lesions; absence of CP was very rare in stable lesions, but very frequent (34%) in culprit lesions.40 Furthermore, CPs are less inflammatory,41 with smaller necrotic cores, and less likely to be thin-cap fibroatheromas on intravascular ultrasound.12 Higher calcification arc and length correlate preferentially with chronic stable angina,42 ,43 and calcification does not increase vulnerability to shear stress but rather contributes to stabilisation.44
In our study, age ≥55 years and residual disease activity (DAS28-CRP≥3.2), were the sole predictors of NCP and MP suggesting a link between clinical inflammation and more vulnerable lesions. This impact of clinical activity on NCP/MP was even higher in subjects <55 years (OR=6.5, 95% CI 1.1 to 39.2), likely reflecting the lower accrual of CRFs in that age group. Despite that, there is no current evidence for more aggressive treatment or revised therapeutic thresholds for traditional CRFs in individuals failing to achieve low disease targets.45 Of note, when DAS28 was used as a continuous variable, enhanced risk for NCP and MP was not noted (OR=1.2, 95% CI 0.8 to 2, adjusted model); a possible reason is that 75% of our patients had DAS28<3.2 and, therefore, there was not enough variability, or spread for significance to be achieved. However, since low disease activity is a recommended target of therapy,45 reporting risk for NCP and MP presence based on that cut-off is clinically relevant and meaningful. Despite evidence for association of CRP with CAD events in the general population,46–48 such risk has not been assigned to specific ranges of CRP in RA. Notably, neither CRP nor ESR alone predicted higher risk for NCP or MP in our study.
To our knowledge, this is the first study to address differential presence, burden, composition and associations of coronary plaque in patients with RA without symptoms or prior diagnosis of CAD versus age and gender-matched controls. An earlier study investigated the presence of obstructive CAD in 47 patients with RA in stable remission using CTA.49 Incidence rates were similar to ours (19.1% for RA and 6.4% for controls versus 12% and 3%, respectively, in ours). However, quantitative and qualitative plaque differences, and their associations where not explored. Our study has certain limitations: (1) Given its cross-sectional nature, causal relationships cannot be inferred. (2) Patients with RA were well controlled, with 75% and 58% achieving low disease activity and remission, respectively. Therefore, overall plaque occurrence and burden in our population may be inferior to patients with RA with higher disease activity. (3) Our RA group included asymptomatic, largely female (90%) subjects with low prevalence of CRFs; 52/150 (35%) had no CRFs and may therefore represent a lower risk group than the general RA population. Nonetheless, plaque differences were robust compared with matched controls. (4) An important concern with the use of CTA may be the radiation exposure (see online supplemental text). Our centre uses low radiation prospective scanning with average doses of 1.9 mSv (background ambient radiation ranges between 3 and 7 mSv per year based on geography).50
In conclusion, subjects with RA have greater prevalence, burden and severity of coronary plaque compared with controls, in particular, the more vulnerable NCP and MP types, providing perhaps a mechanistic insight to their higher risk of cardiac events. Steeper increases in plaque occur in RA at earlier time points, and higher risk NCP and MP preferentially associate with residual clinical inflammation.
Acknowledgments
The authors would like to thank Ferdinand Flores RN for study-related procedure facilitation and blood sample acquisition, handling, storage and shipping. We would also like to express our gratitude to the patients participating in the study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement 1
- Data supplement 2 - Online figure
Footnotes
-
Handling editor Tore K Kvien
-
Contributors All authors were involved in drafting the article or revising it critically for important intellectual content, and all authors approved the final version to be published. GAK and MJB were responsible for study concept and design. GAK, JM, TYC and SM were responsible for data acquisition. Data analysis and interpretation was done by GAK, JM, TYC, DL and MJB.
-
Funding American Heart Association AHA 09CRP225100.
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval Institutional Review Board, Harbor-UCLA Medical Center.
-
Provenance and peer review Commissioned; externally peer reviewed.