Article Text

Abstract
Objective We recently reported an association of the SPP1 rs9138 and rs11439060 functional variants with the risk of rheumatoid arthritis (RA), the association being greater in anti-citrullinated protein autoantibody (ACPA)-negative patients. We hypothesised that SPP1 may contribute to the severity of joint destruction in RA, specifically in the ACPA-negative population.
Methods Patients with RA in the ESPOIR cohort underwent genotyping for SPP1 rs9138 and rs11439060. Radiographs of the hands and feet were obtained at the first visit and at 1- and 2-year follow-up. Association analyses were performed by ACPA status. A replication study of the relevant subset of the Leiden Early Arthritis Clinic (EAC) cohort was performed.
Results In the ESPOIR cohort (652 patients), rs9138 was significantly associated with radiological progression of joint destruction at 2 years, the association being restricted to 358 ACPA-negative patients (p=0.034). In the replication study with the Leiden EAC cohort (273 ACPA-negative patients), rs4754, which is in complete linkage disequilibrium with rs9138, was significantly associated with joint damage progression in ACPA-negative patients at 2- and 7-year follow-up (p=0.019 and p=0.005, respectively). Combined analysis of the two cohorts revealed a 0.95-fold rate of joint destruction per year per minor allele (p=0.022).
Conclusions The SPP1 rs9138 variant contributes to joint damage progression in ACPA-negative RA.
- Rheumatoid Arthritis
- Ant-CCP
- Autoantibodies
- Gene Polymorphism
- Early Rheumatoid Arthritis
Statistics from Altmetric.com
Introduction
Rheumatoid arthritis (RA) is a systemic, inflammatory, autoimmune disease characterised by peripheral synovial joint inflammation which can lead to joint destruction. Approximately two-thirds of RA cases are seropositive for rheumatoid factor or anti-citrullinated protein autoantibodies (ACPAs).1 The heritability of ACPA-positive and ACPA-negative disease is comparable,2 and recent association studies have provided further support for distinct genetic aetiologies of ACPA-positive and ACPA-negative RA subsets.3 ,4 ACPA-positive RA patients are particularly characterised by progressive joint destruction.5 However, little information is available on joint destruction processes in the ACPA-negative subset. Currently, we cannot offer personalised medicine for patients with RA because we cannot identify those who will have the most severe disease course, nor do we understand the pathogenesis underlying these interindividual variances. To improve this situation, identification of risk factors for joint destruction is required.
Genetic variants are estimated to contribute to 58% of the total variance in RA joint destruction, with clinical and serological risk factors explaining only about one-third of the total phenotypic variation.6 Most risk alleles for RA joint destruction have been identified in ACPA-positive patients or in pooled ACPA-negative and ACPA-positive patients, but we lack information about the genetic contribution to ACPA-negative RA severity.7–9 Identifying individual genetic risk factors would increase our understanding of the mechanisms underlying variation in severity of joint destruction, particularly in ACPA-negative disease.
Recently, through a large case–control association study, our group reported a significant contribution of the combination of the SPP1 rs11439060 and rs9138 frequent alleles to risk of RA, the magnitude of the association being greater in ACPA-negative patients.3 These patients fulfilled the 1987 American College of Rheumatology (ACR) revised criteria for RA, which include radiographic changes typical of RA10; so ACPA-negative individuals may have had joint destruction to be classified as having RA. SPP1 encodes osteopontin (OPN), an extracellular-matrix glycosylated phosphoprotein with multiple functions including bone formation and remodelling.11 Consequently, we hypothesised that SPP1 variants may contribute to the severity of joint destruction in RA, specifically in ACPA-negative patients.
Patients and methods
Study population
The exploratory study included 652 patients with RA from the ESPOIR cohort who were positive or negative for ACPAs and were included in the large case–control association study previously reported.3 ,12 The replication study included 273 ACPA-negative RA cases from the Leiden Early Arthritis Clinic (EAC) cohort (table 1).13 All patients fulfilled the 1987 ACR revised criteria for RA.10 They all provided informed written consent as approved by the recruiting site review board at each of the affiliated institutions.
Characteristics of the ESPOIR and Leiden Early Arthritis Clinic (EAC) cohorts of patients with rheumatoid arthritis genotyped for SPP1 rs9138 or rs4574
Genotyping
In the exploratory study with the ESPOIR cohort, SPP1 rs11439060 and rs9138 variants were genotyped by use of a competitive allele-specific PCR system (Kaspar genotyping; Kbioscience, Hoddeston, UK).3 In the Leiden EAC cohort, SPP1 rs4754, which is in complete linkage disequilibrium with rs9138,3 was genotyped using Illumina Human CytoSNP-12V2.
Radiographic joint destruction
In both the ESPOIR and Leiden EAC cohorts, all radiographs of hands and feet were scored by the van der Heijde-modified Sharp score (mSHS) by one experienced reader per cohort who was blinded to clinical, biological and genetic data.14 The intraclass correlation coefficient was 0.97 and 0.91, respectively.
Statistical analysis
A multivariate regression analysis (MRA) was used, with radiographic damage as the response variable (see online supplementary text for a detailed description of the MRA). The analyses were performed with the genetic variable and its interaction with time in the model, reflecting a constant and a time-dependent effect of progression of joint damage, respectively.15
To validate our a priori hypothesis (ie, the contribution of SPP1 rs11439060, rs9138 and the rs11439060–rs9138 risk allele combination in the ACPA-negative population), we selected the best-fit model at the exploratory stage, as previously described, which was then replicated in the Leiden EAC cohort.3 MRA of both ACPA-negative populations was used to assess the magnitude of the SPP1 effect on radiographic joint destruction in early RA. Analyses used SPSS V.20.0.
Results
Exploratory study
We analysed data for 652 patients with RA and 1768 radiographs. For a complete overview of the MRA of SPP1 rs11439060, rs9138 and risk allele combination, see online supplementary table S1. Briefly, the best-fit model involved rs9138 (see online supplementary table S2). In agreement with our a priori hypothesis, rs9138 was significantly associated with radiographic progression over a 2-year follow-up in ACPA-negative patients, as seen by an additive model with a 0.93-fold rate of joint destruction per year per minor allele as compared with the wild-type (p=0.034) (figure 1A–C).

Association of SPP1 rs9138 and joint damage progression in patients with rheumatoid arthritis (RA) in the exploratory study. Multivariate regression analysis modelled median van der Heijde-modified Sharp score (mSHS) in patients with RA in the ESPOIR cohort (exploratory study) at 1- and 2-year follow-up. 1, rs9138 common allele; 2, rs9138 minor allele. (A) Overall RA patients. (B) Anti-citrullinated protein autoantibody (ACPA)-positive RA patients. (C) ACPA-negative RA patients.
Replication study
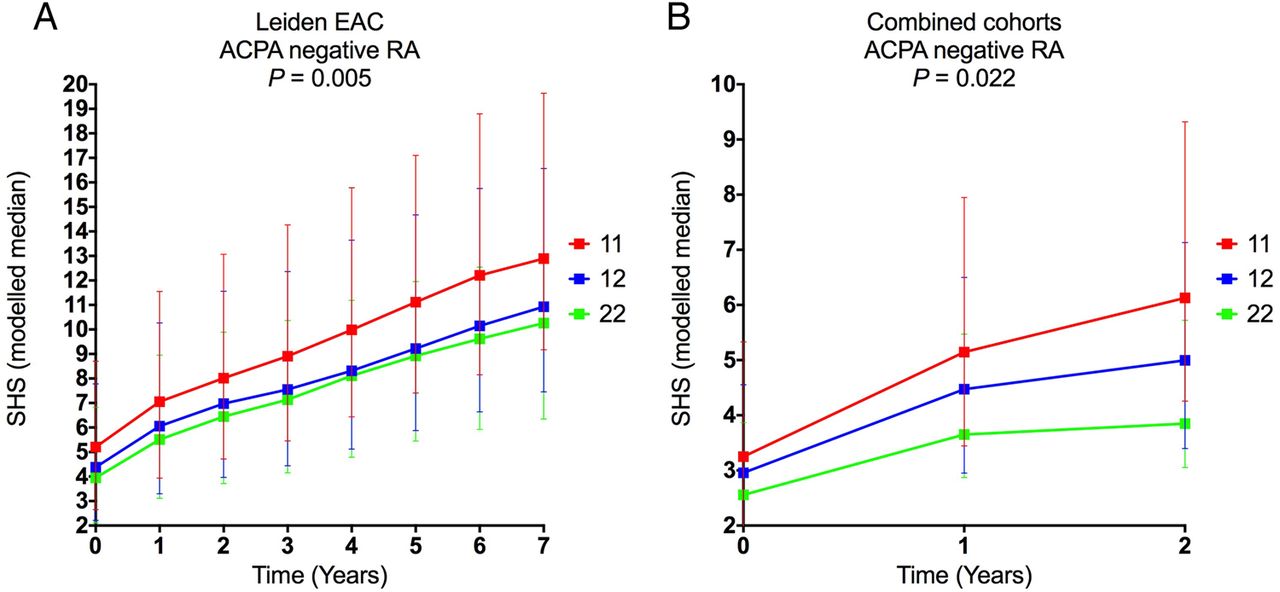
We analysed data for 273 ACPA-negative patients in the Leiden EAC cohort and 704 radiographs over a 2-year follow-up. We replicate the contribution of rs9138, as MRA revealed that rs4754 was associated with radiographic progression over the 2-year follow-up with a 0.81-fold rate of joint destruction for each minor allele at any time compared with the wild-type (p=0.019). Analysis of 1316 radiographs over 7 years of follow-up revealed a persistent effect of rs4754, with a 0.78-fold rate of joint destruction for each minor allele at any time compared with the wild-type (p=0.005; figure 2A).
{kind=link}
{kind=link}
Association of SPP1 rs4754 and joint damage progression in patients with rheumatoid arthritis (RA) in the replication study and combined analysis at 2-year follow-up. Multivariate regression analysis modelled median van der Heijde-modified Sharp score (mSHS) in patients with RA in the Leiden Early Arthritis Clinic (EAC) anti-citrullinated protein autoantibody (ACPA)-negative cohort during a 7-year follow-up (A) and combined analysis of the ESPOIR and Leiden EAC ACPA-negative cohorts at a 2-year follow-up (B). 1, rs9138/rs4574 common allele; 2, rs9138/rs4574 minor allele.
Combined analysis of early RA during the 2-year follow-up
Data for 631 ACPA-negative patients and 1664 radiographs were available for the combined analysis of the ESPOIR and Leiden EAC cohorts. MRA over the 2-year follow-up revealed a 0.95-fold rate of joint destruction per year per minor allele compared with the wild-type (p=0.022; figure 2B).
Discussion
The rate of progression of joint damage in RA is highly variable and is associated with the severity of the disease. Genetic variants are estimated to contribute to most of the local variance in RA joint destruction. Several data have suggested that OPN, encoded by SPP1, may be involved in bone erosion. In addition, we recently identified SPP1 as a new RA susceptibility gene, the magnitude of the association being greater in ACPA-negative disease.3 Because ACPA-negative patients fulfilled the ACR modified criteria, SPP1 may contribute to the variation in joint destruction in this particular subset of the disease.
For the two SPP1 rs11439060 and rs9138/rs4754 RA risk variants investigated, the rs9138/rs4754 common allele contributed to joint destruction of RA—that is, the minor allele had a protective effect. This finding is in agreement with our a priori hypothesis because the rs9138 common A allele has been identified as an ACPA-negative RA risk allele.3 The replication study, including analyses at the same time of follow-up (2 years) and also after a longer period (7 years), provided evidence that the SPP1 rs9138 variant contributes to the severity of radiographic damage in ACPA-negative RA in both the early and intermediate course of the disease. Analyses of the combined sets revealed an interaction between SPP1 rs9138/rs4754 and time at the 2-year follow-up, which suggests a strong effect of SPP1 on radiographic damage at the early stage of the disease. A recent study of the ESPOIR cohort found that the first-year radiographic progression was a predictor of further progression in early RA, which suggests that, after the early period of the disease, time has a constant effect.16
Complex diseases, such as RA, invariably involve multiple genes and often exhibit variable symptom profiles. The extent to which disease symptoms, course and severity differ between affected patients may result from underlying genetic heterogeneity. Genes with modifier effects may or may not also influence disease susceptibility. Indeed, SPP1 seems to act as a susceptibility and a modifier gene. The effect of the rs11439060 variant differed in this study compared with our previous case–control study,3 the rs11439060–rs9138 risk allele combination not being identified as the best-fit model. Nonetheless, a contribution of rs11439060 could not be definitely excluded; the sample size required to detect such association with a power of 80% would be 1000 ACPA-negative patients with early RA.
To our knowledge, this is the first report of the identification of a genetic variant associated with joint damage progression in ACPA-negative RA. We took advantage of two cohorts including sequential radiographs of hands and feet, which strengthened the evidence of the contribution of SPP1 rs9138. Several studies have reported an association of the rs9138 A risk allele with low serum levels of soluble OPN.3 ,17 However, to date, the exact role of OPN in RA joint damage is controversial: distinct murine models of RA have shown conflicting results on the relevance of OPN in bone erosion pathogenesis,18 ,19 and, more importantly, OPN blockade was found to be unlikely to induce robust clinical improvement in patients with RA.20
In conclusion, we have identified and replicated a genetic SPP1 variant predisposing to joint damage progression in ACPA-negative RA. Further studies of OPN at the protein level are required to better understand the role of this variant in the pathogenesis of the progression of radiographic damage in ACPA-negative RA.
Acknowledgments
We thank Nathalie Rincheval for expert monitoring and data management and all the investigators who recruited and followed patients.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Handling editor Tore K Kvien
-
P-AJ and HWvS contributed equally.
-
Contributors P-AJ and PD: designed the study. HWvS, SG, DN, AHMvdHvM and PD: carried out the statistical analyses. All authors collected the patients’ data. P-AJ and PD: wrote the first version of the manuscript. All authors read and approved the final version of the manuscript.
-
Funding PD is supported by a grant from the French Society of Rheumatology and an unrestricted grant from Pfizer. An unrestricted grant from Merck Sharp and Dohme (MSD) was allocated for the first 5 years of the ESPOIR cohort. Two additional grants from INSERM were obtained to support part of the biological database. The French Society of Rheumatology, Pfizer, Abbvie and Roche-Chugai also supported the ESPOIR cohort study.
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval Medical ethics committees of the participating centres.
-
Provenance and peer review Not commissioned; externally peer reviewed.