Article Text

Abstract
Objective To summarise the evidence regarding the dose-response association between alcohol consumption and risk of rheumatoid arthritis (RA).
Method Studies were identified from search of MEDLINE, Embase and Web of Science databases between 1 January 1946 and 10 April 2013, and from review of the conference abstracts and the reference lists of retrieved articles. Prospective studies that reported relative risks (RRs) with 95% CIs for the association between alcohol consumption and the risk of RA were included. Results from individual studies were pooled using a dose-response meta-analysis.
Results Up to 10 April 2013, 8 prospective studies contained 195 029 participants and 1878 RA cases were included. The results indicated that low to moderate alcohol consumption yielded a preventive effect on RA development (RR: 0.86; 95% CI 0.78 to 0.94), and provided some evidence of a non-linear relationship between alcohol consumption and risk of RA. Dose-response meta-analysis of the study data revealed that compared with that for no alcohol consumption, the adjusted RR was 0.93 (95% CI 0.88 to 0.98) for 3 g/day of alcohol consumption, 0.86 (95% CI 0.76 to 0.97) for 9 g/day, 0.88 (95% CI 0.78 to 0.99) for 12 g/day, 0.91 (95% CI 0.81 to 1.03) for 15 g/day, and 1.28 (95% CI 0.94 to 1.73) for 30 g/day. Subgroup analysis indicated that women who had low to moderate alcohol consumption had a 19% reduction in RA risk. Regardless of sex, a consistent low to moderate alcohol consumption for a period of at least 10 years was found to have a 17% reduction in RA risk.
Conclusions Low to moderate alcohol consumption inversely associated with the development of RA in a manner that appears to be dose-dependent, time-dependent and sex-dependent. Large prospective studies that investigate gene-environment interactions are required to further clarify the aetiology of RA.
- Epidemiology
- Rheumatoid Arthritis
- Inflammation
Statistics from Altmetric.com
Introduction
Rheumatoid arthritis (RA), an autoimmune disease, characterised by chronic, destructive, debilitating arthritis that affects approximately 1% of the adult population,1 ,2 is hypothesised to result from the interaction between environmental and genetic factors.3 ,4 Regarding the possible environmental factors, those related to lifestyle are believed to play an important role.5 Alcohol consumption has been identified as a preventive factor, although the findings regarding its effect on RA development have been inconsistent. While the results of several observational studies suggest that moderate alcohol consumption may decrease the risk of RA,6–8 no clear-cut mechanism has been identified to explain this inverse relationship. One study that examined the association between alcohol consumption and markers of inflammation in preclinical patients with RA identified a U-shaped association between daily alcohol consumption and IL-6 levels prior to emergence of RA symptoms,9 suggesting the existence of a non-linear, possibly U-shaped or J-shaped, dose-response relationship between alcohol consumption and risk of RA.
To further examine these findings and provide evidence of a hypothesised inverse association between low to moderate alcohol consumption and risk of RA, we performed a systematic review and meta-analysis to quantitatively assess the dose-response relationship between alcohol consumption and RA.
Materials and methods
Literature search
A systematic literature search of MEDLINE, Embase and Web of Science databases for identification of articles published between 1 January 1946 and 10 April 2013 was performed by two investigators (CX and ZJ). The same search strategy was applied to Web of Science as that used for MEDLINE and Embase (see online supplementary search strategy) using the appropriate controlled vocabulary. No language restriction was imposed. The conference abstracts in the supplements of the ACR/ARHP Annual Scientific Meeting from 2006 to 2012 were also reviewed. The reference lists of the identified publications were reviewed for identification of additional studies. The headings and abstracts of the studies identified in the database were reviewed by two investigators (CX and ZJ) for identification of studies that met the following criteria: (1) use of prospective design, including cohort design or nested case-control design; (2) examination of alcohol consumption as the variable of interest; (3) determination of prevalence of RA, as identified by physicians and/or by use of the record linkage system, as the outcome of interest; and (4) reporting of the OR or relative risk (RR) of RA for high, moderate, or low alcohol consumption compared with no alcohol consumption, and their 95% CIs. All studies that used a retrospective case-control design were excluded based on recognition that (1) recall of alcohol consumption may be affected by recall bias after diagnosis or onset of disease, leading to denial of consumption or selective recall of presumed aetiological factors and (2) behavioural changes may occur after onset of symptoms that affect the reporting of consumption. However, nested case-control studies were not excluded, as these studies had collected dietary and other relevant data before diagnosis or onset of RA, and thus did not face the two limitations of retrospective case-control studies described above.
Data extraction
Data extraction was conducted by two investigators (ZJ and CX), and independently checked for accuracy by a third investigator (JH). For each included study, data regarding the title, author, publication year, country in which it was conducted, study design, sampling subjects, assessment of alcohol consumption, sample size, proportion of males, age of subjects, seropositive rate, duration of follow-up, covariates controlled for by matching or multivariable analysis, the number of cases/non-cases or person-year data and adjusted RR for each consumption category and its 95% CI were extracted. For studies that reported several multivariable-adjusted RRs, the effect estimate that was most fully adjusted for potential confounders was extracted. Study quality was assessed using the 9-star Newcastle-Ottawa Scale by two investigator (ZJ and QC).10 Online supplementary table S1 shows the definition of alcohol consumption used, and the means of conversion of categories within each study.
Statistical analysis
We examined the relationship between alcohol consumption and risk of RA on the basis of the adjusted RRs and 95% CIs reported in each study. Because the incidence of RA is low, the ORs in nested case-control studies approximate the RRs.11 ,12 Using the converted data in online supplementary table S1, meta-analyses were performed to compare the risk between high alcohol consumption and no alcohol consumption, and between low to moderate alcohol consumption and no alcohol consumption. A fixed-effects model was used to estimate the pooled RRs with 95% CIs if there was no evidence of heterogeneity; otherwise, a random-effect model was used.13 ,14 Dose-response meta-analysis was then conducted from the correlated natural log of RRs across categories of alcohol consumption.15 ,16 To derive the dose-response curve, alcohol consumption was modelled using restricted cubic splines with three knots at fixed percentiles (10, 50 and 90%) of the distribution. The p value for non-linearity was calculated by testing the null hypothesis that the coefficient of the second spline was equal to zero. The details of the methods used have been described by Larsson and Orsini.15 ,17 ,18
The χ2 test and I2 statistic were used to explore the heterogeneity among studies. The Egger's regression test,19 Begg's test,20 and visual inspection of a funnel plot were performed to assess publication bias. Subgroup analyses by geographic area, sex, years of follow-up, type of drinking and serological status were performed to examine the relationship between alcohol consumption and RA risk. Sensitivity analyses were performed in two ways: first, by excluding those studies that met relatively fewer quality criteria of the Newcastle-Ottawa Scale (<7 stars); second, by excluding the studies that used a nested case-control design.
Stata V.12.0 software (Stata, College Station, Texas, USA) was used for all analyses, and all statistical tests were two-sided; p<0.05 was considered an indication of statistical significance.
Results
Up to 10 April 2013, 2456 records were retrieved using the search strategy described. Review of the titles and abstracts according to the inclusion and exclusion criteria resulted in exclusion of 2422 articles. Reading of the full text of the remaining 34 articles for further evaluation resulted in the selection of eight studies, including five full-text articles,6 ,21–24 two abstracts,25 ,26 and one letter27 for subjection to meta-analysis. One identified study used the lowest consumption level (0.05–3.66 g/day) as the reference group.21 In an effort to avoid combining studies that were not comparable, we chose to exclude this study when comparing the risk of RA between high or low to moderate drinkers and non-drinkers. Online supplementary table S2 shows the studies that were excluded and the reason for their exclusion, and figure 1 shows the entire search process. Table 1 shows the general characteristics of the eight included studies which, together, had examined 195 029 participants and 1878 RA cases, and online supplementary table S3 presents the quality assessment of the included studies in detail.

Selection of studies for inclusion in meta-analysis.
Main characteristic of the included studies on alcohol consumption and risk of rheumatoid arthritis
Effects of alcohol consumption on RA
The summary RR of RA for a high level of alcohol consumption compared with no alcohol consumption (figure 2) was found not to be statistically significant (RR: 0.99; 95% CI 0.78 to 1.25). Low to moderate alcohol consumption was found to have a preventive effect for RA (RR: 0.86; 95% CI 0.78 to 0.94). No evidence of the existence of heterogeneity across studies was identified. As shown in figure 3, some evidence of a non-linear relationship between alcohol consumption and risk of RA was found (p=0.008). Compared with that for no alcohol consumption, the adjusted RR was 0.93 (95% CI 0.88 to 0.98) for 3 g/day of alcohol consumption, 0.86 (95% CI 0.76 to 0.97) for 9 g/day, 0.88 (95% CI 0.78 to 0.99) for 12 g/day, 0.91 (95% CI 0.81 to 1.03) for 15 g/day, and 1.28 (95% CI 0.94 to 1.73) for 30 g/day (see online supplementary table S4).
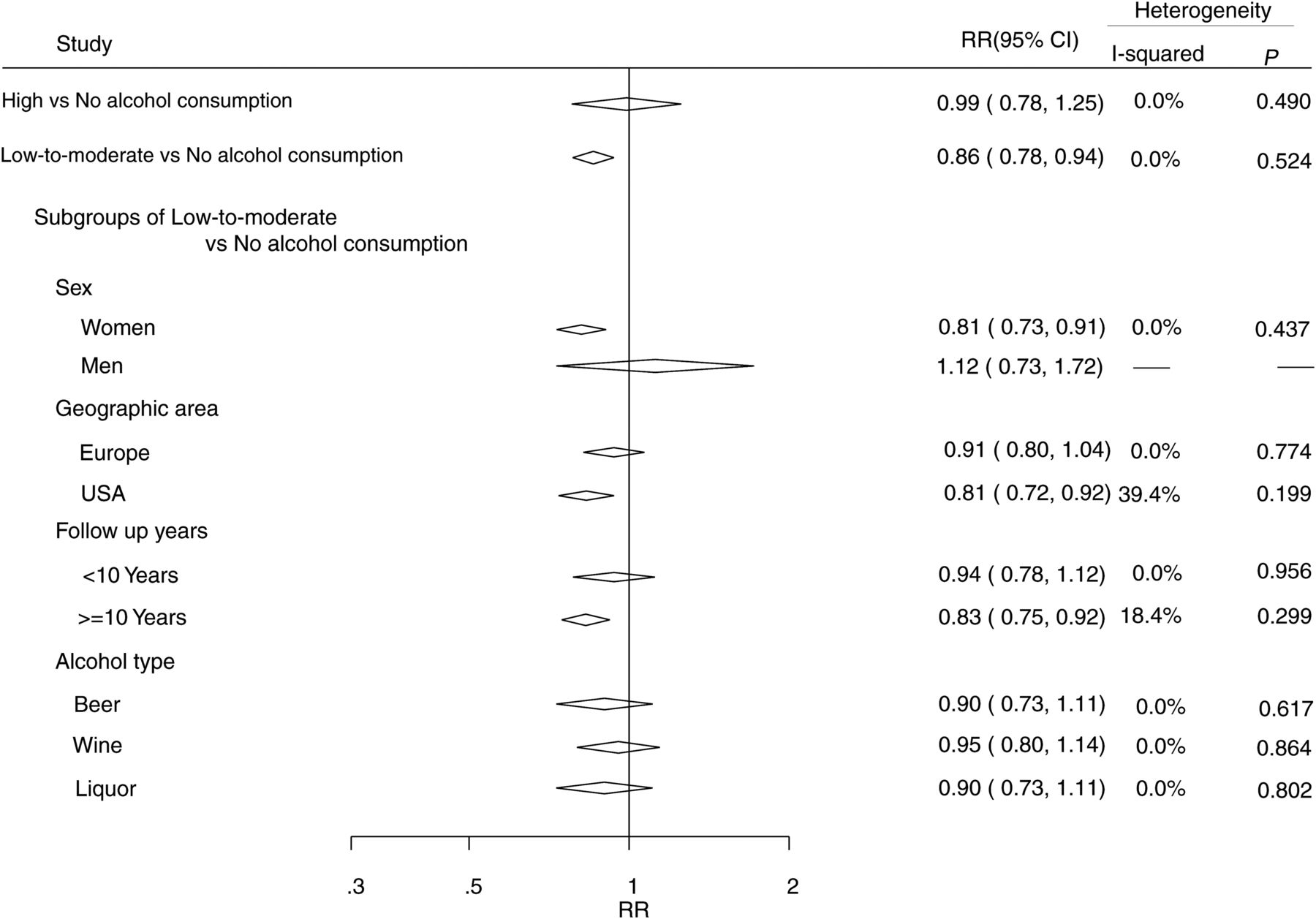
Adjusted relative risks of rheumatoid arthritis for the high alcohol consumption versus no alcohol consumption and low to moderate alcohol consumption versus no alcohol consumption.
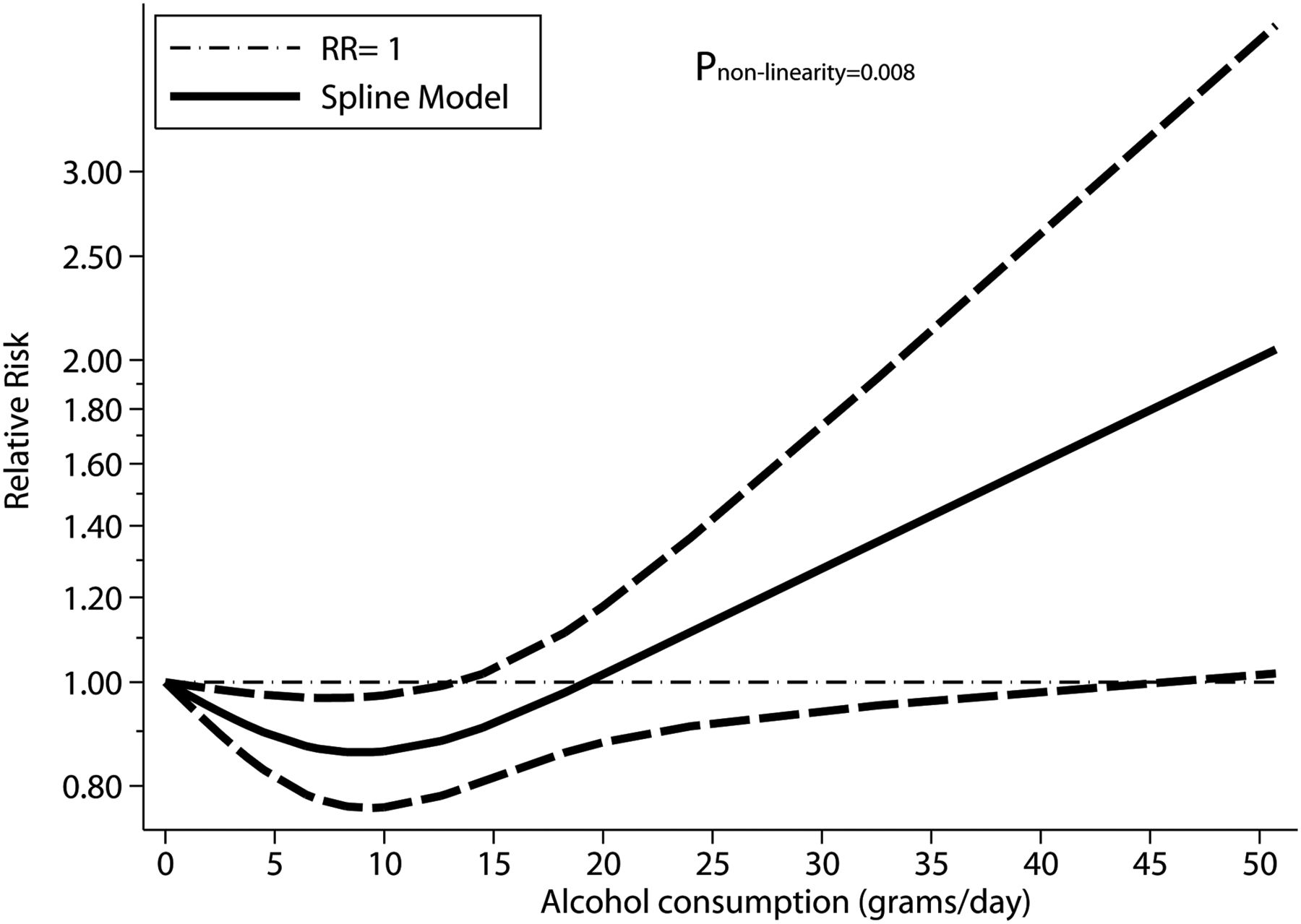
Dose-response relationship between alcohol consumption and risk of rheumatoid arthritis.
Subgroup analysis
As shown in figure 2, compared with women who consume no alcohol, women who had low to moderate alcohol consumption were found to have a 19% reduction in RA risk (RR: 0.81, 95% CI 0.73 to 0.91). Regardless of sex, a consistent low to moderate alcohol consumption for a period of at least 10 years was found to have a 17% reduction in RA risk (RR: 0.83; 95% CI 0.75 to 0.92). As shown in online supplementary table S4, the subgroup analyses under the dose-response setting showed comparable results, which also found that generally, individuals consuming up to 15 g/day for a period of at least 10 years had a lower risk of RA than did non-drinkers.
Sensitivity analysis
As shown in online supplementary table S4, a dose-response trend similar to that identified by analysis of all eight studies emerged when three studies of low quality were excluded.22 ,25 ,27 The results of sensitivity analysis performed after excluding the studies that used a nested case-control design also indicated that low to moderate alcohol consumption is inversely correlated with risk of RA.
Publication bias
The funnel plot and Egger’s test (p=0.047) showed some evidence of publication bias in the comparison between low to moderate drinkers and non-drinkers (figure 4). No significant asymmetry of the funnel plot was detected in the comparison between heavy drinkers and non-drinkers.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Funnel plot of log relative risk versus standard error of log relative risks.
Discussion
The findings of the meta-analysis described here indicate that alcohol consumption, but only at a low to moderate level, is inversely and significantly associated with the development of RA. Specifically, they indicate the existence of a J-shaped non-linear trend between alcohol consumption and risk of RA. This inverse association between alcohol consumption and risk of RA begins to lose its significance as consumption increases to more than 15 g/day, which is approximately 1.5 standard drinks in Europe and one standard drink in the USA.28
A plausible explanation of a reduced risk of RA with low to moderate alcohol consumption is that alcohol may downregulate immune response and decrease the production of selected proinflammatory cytokines.6 ,29–32
Compared with a newly published systematic review conducted by Scott et al,33 the results of the present study appear more reliable. Although Scott et al33 also found an inverse association between alcohol consumption and the presence of RA, they only got this result from retrospective case-control studies. The results of such studies cannot be used to identify cause–effect relationships, as inverse associations identified might simply reflect the fact that patients with RA drink less alcohol after disease onset, especially patients treated with methotrexate. By contrast, the results of prospective studies in which alcohol consumption was monitored in a cohort that was followed-up to determine which patients developed RA could be used to identify a causal relationship between alcohol consumption and risk of RA.34 Unlike the present study, Scott et al excluded abstracts and letters25–27 in their analysis. As the two abstracts included in the present study are from well-designed cohorts,35 ,36 excluding them may have resulted in insufficient statistical power and publication bias.
This study had two strengths that likely increased the reliability and validity of the findings. First, only prospective studies were included, which could eliminate selection bias and recall bias that could be of concern in retrospective case-control studies. Second, the dose-response analysis included a wide range of alcohol consumption, which allows an accuracy assessment of the dose-response relationship between alcohol consumption and RA risk.
This meta-analysis faced several potential limitations that must be considered when interpreting the results. First, a meta-analysis is not able to solve problems with confounding factors that could be inherent in the original studies. Although major potential confounders had been adjusted in most included studies, residual or unknown confounding cannot be excluded. Low to moderate drinkers may share, or be exposed to, a greater number of beneficial environmental factors compared with non-drinkers and heavy drinkers, such as a greater number of educational opportunities, greater ability to engage in physical activity, and access to a healthier diet. RA is believed to result from the interactions between environmental and genetic factors,37 but no data regarding genetic factors were contained in the primary aggregate results. Second limitation is misclassification of alcohol consumption, which was inevitable given that consumption of alcohol was self-reported in most studies and only two studies6 ,26 updated information on alcohol consumption during follow-up. Under-reporting of high alcohol consumption38 or changes in consumption during follow-up would most likely lead to underestimation of true association between alcohol consumption and risk of RA. Third, as in all meta-analyses of published studies, the possibility of publication bias was ever present. In the present study, some small studies with inverse association between alcohol consumption and risk of RA seemed to be suppressed. The presence of possible publication bias could have led to an underestimation of the beneficial effect of low to moderate alcohol consumption over RA. Fourth, results of several subgroups, for example, male subgroup, were based on a limited number of studies, and we, therefore, cannot rule out the possibility that insufficient statistical power may be present. Heterogeneity may be introduced because of methodological differences among studies. However, in this meta-analysis, no evidence of heterogeneity was found from the main results. The sensitivity analyses regarding methodological differences also have yielded consistent results with those from overall analysis.
In summary, the results of this study suggested that low to moderate alcohol consumption may reduce the risk of developing RA, possibly in a dose-dependent, time-dependent and sex-dependent manner. These results have implications for public health measures, such as guidelines for lowering the risk of RA, which may be revised to recommend low to moderate alcohol consumption. However, any advice regarding alcohol consumption should be tailored to the individual risks and potential benefits. Large prospective studies that investigate the interactions between environmental factors and functional polymorphisms are now required to further clarify the aetiology of RA, and contribute to the ultimate aims of such research: establishment of an easily applicable prediction rule for the development of RA and provision of evidence-based recommendations to decrease the risk of RA.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement 1
- Data supplement 2 - Online table 1
- Data supplement 3 - Online table 2
- Data supplement 4 - Online table 3
- Data supplement 5 - Online table 4
Footnotes
-
Handling editor Tore K Kvien
-
ZJ, CX and QC contributed equally.
-
Contributors ZJ, JH and QC discussed and developed the question for this review. CX and ZJ carried out the searches. ZJ and CX assessed the eligibility of the studies for inclusion, extracted data and carried out all analysis. All authors were involved in interpreted and discussed results. ZJ wrote the first draft of this paper and it was reviewed by QC and JH. XW was involved in interpreted and discussed results in the first round of revision. All authors agreed on the final draft of this study. JH is the guarantor.
-
Funding National Natural Science Foundation (grant number 81001287), Leading Talents of Science in Shanghai 2010 (grant number 022), the key discipline construction of evidence-based public health in Shanghai (grant number 12GWZX0602).
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.