Article Text

Abstract
Objective To investigate whether trabecular and cortical bone structure differ between patients with rheumatoid arthritis (RA) and psoriatic arthritis (PsA). So far, no study has performed a detailed comparative analysis of bone structure in patients with RA and PsA.
Methods 110 patients (60 RA, 50 PsA) received high-resolution peripheral quantitative CT of the distal radius. Demographic and disease-specific parameters including anti-rheumatic treatment, bone erosion status and previous fractures were recorded.
Results RA and PsA patients were comparable in age, gender, body mass index, disease duration, disease activity, functional status, antirheumatic treatment and bone erosion status. No significant differences were found for volumetric bone mineral density (BMD), including total BMD (300±77 vs 316±62 mgHA/cm3), trabecular BMD (152±46 vs 165±40 mgHA/cm3) and cortical BMD (787±113 vs 818±76 mgHA/cm3) when comparing RA patients to PsA patients, respectively. However, in contrast to seronegative RA, seropositive RA showed significantly reduced trabecular BMD (p=0.007), bone volume per tissue volume (p=0.007) and trabecular number (p=0.044), as well as a strong trend towards higher trabecular inhomogeneity compared to PsA patients. In the regression analysis, higher age, female gender and presence of autoantibodies were independently associated with trabecular bone loss.
Conclusions Seropositive RA exhibits more profound changes in trabecular bone architecture than seronegative RA or PsA. The data support the concept that seropositive RA is a disease entity that is distinct from seronegative RA and PsA.
- Psoriatic Arthritis
- Rheumatoid Arthritis
- Bone Mineral Density
- Osteoporosis
Statistics from Altmetric.com
Introduction
Rheumatoid arthritis (RA) and psoriatic arthritis (PsA) are chronic inflammatory joint diseases characterised by bone destruction.1–3 Chronic synovitis occurs in RA as well as in PsA. Synovitis elicits bone erosion by inducing the differentiation of bone-resorbing osteoclasts.4 ,5 PsA is additionally characterised by pronounced inflammation at enthesial sites, where bone is also directly exposed to inflammatory tissue.6 Despite some similarities, considerable differences exist between RA and PsA regarding pathogenesis, clinical presentation and radiographic changes,7–9 and findings in RA can not necessarily be translated to PsA.
Apart from local bone destruction, inflammatory diseases like RA and PsA have the potential to disturb bone homeostasis on the systemic level. Even minor chronic increases of inflammatory activity can trigger systemic bone loss.10 Bone mineral density (BMD) is significantly decreased in RA patients compared to controls11 and the risk of fracture is increased at vertebral12 and peripheral skeletal sites.13 High disease activity is an independent predictor of bone loss in RA.14 Furthermore, high C reactive protein level, long disease duration and high radiographic erosion scores have been identified as predictors for vertebral fractures in RA patients.15–18
Far less is known about BMD changes and fracture risk in PsA patients. One study has shown decreased BMD in PsA patients compared to healthy controls,19 whereas other studies found no major differences.20 ,21 One possible explanation for ‘normal’ BMD in PsA could be pathological bone deposition along periosteal sites.21 Considering the similarities between spondylarthritis and PsA, the observation of a high prevalence of vertebral fractures in early PsA22 supports the concept that bone loss is a feature of RA and of PsA. Surprisingly, no study has yet compared the trabecular bone architecture of RA and PsA. Therefore, we aimed to perform a detailed comparative analysis of bone in RA and PsA patients by assessing volumetric BMD (vBMD) as well as trabecular and cortical microstructure at the distal radius. High-resolution peripheral quantitative CT (HR-pQCT) was used as a non-invasive imaging method that permits in vivo three-dimensional characterisation of bone microarchitecture and the assessment of vBMD for the total, trabecular and cortical bone.23 HR-pQCT has already been used with good sensitivity to detect periarticular bone changes in arthritis patients.24 ,25 Differences in the periarticular bone between RA and PsA have been documented in the metacarpophalangeal (MCP) joints by HR-pQCT.26 Detailed characterisation of bone quantity and bone quality can more easily and reliably be accomplished at the distal radius, which contains a larger trabecular network compared to MCP joints, allowing reliable calculation of bone microstructure by established algorithms.27
Methods
Patients and study design
A total number of 110 patients, specifically 60 patients with RA (33 women, 27 men) and 50 patients with PsA (24 women, 26 men), were recruited at the Department of Internal Medicine 3 of the University of Erlangen-Nuremberg. RA patients fulfilled the 2010 American College of Rheumatology/European League Against Rheumatism classification criteria for RA,28 and PsA patients fulfilled the Classification of Psoriatic Arthritis criteria.29 Patients with RA and PsA were enrolled consecutively. RA patients were divided into seropositive RA (anticyclic citrullinated peptide antibody (ACPA)-positive and/or rheumatoid factor-positive, RA[+], n=38) and seronegative RA (RA[−], n=22) patients. The study was approved by the local ethics committee and the national radiation safety agency (Bundesamt fuer Strahlenschutz). Subjects were enrolled in the study after agreeing to participate and signing informed consent forms. The study was performed in accordance with the Declaration of Helsinki.
Disease duration, disease activity according to the Disease Activity Score 28 (DAS28), C reactive protein level and ACPA as well as rheumatoid factor (RF) positivity were determined in all patients. Current and previous use of high-dose oral glucocorticoids (≥7.5 mg prednisolone equivalent daily for ≥3 months), low-dose oral glucocorticoids (≤5 mg prednisolone equivalent daily for ≥3 months), conventional disease-modifying antirheumatic drugs (DMARDs: methotrexate, leflunomide, hydroxychloroquine, sulfasalazine) and biologic DMARDs (tumour necrosis factor (TNF)-α-inhibitors, abatacept, rituximab and tocilizumab) and bisphosphonates (oral and intravenous) were recorded. In addition, the functional status of all patients according to the Health Assessment Questionnaire (HAQ) as well as fracture history was documented.
High-resolution peripheral quantitative CT
HR-pQCT measurements were performed by an XtremeCT scanner (Scanco, Brüttisellen, Switzerland) at the distal radius of the clinically more affected arm using the manufacturer's standard in vivo protocol. The reference line was set manually. The first CT slice was 9.5 mm proximal to the reference line. For scanning, the hand was immobilised in a carbon fibre cast. An antero-posterior scout view was then used to determine the volume of interest; 110 slices (voxel size 82 µm) were then carried out. Details of the HR-pQCT measurements of the distal radius have been previously described elsewhere.23 All measurements were performed with the standard analysis software. Daily cross-calibrations with standardised control phantoms (Moehrendorf, Germany) were conducted to standardise measurements.
vBMD including total BMD (mgHA/cm3), trabecular BMD (Dtrab, mgHA/cm3), the peripheral trabecular density adjacent to the cortex (mgHA/cm3), the central medullary trabecular density (mgHA/cm3), the ratio of peripheral to medullary trabecular bone density, and cortical BMD (mgHA/cm3) were measured. Bone microstructure including the trabecular bone volume fraction (BV/TV), trabecular number (Tb.N, 1/mm), trabecular separation (Tb.Sp, mm), inhomogeneity of the network (mm), cortical thickness (Ct.Th, mm), cortical porosity (Ct.Po, %), cortical pore volume (mm³) and cortical pore diameter (mm) were analysed. Bone erosion was additionally documented in scans of the MCP and the proximal interphalangeal joints.
Statistical analysis
Data analyses were performed using SPSS software, V.19 (SPSS Inc., Chicago, Illinois, USA). The analysis's first step comprised descriptive statistical measures of sample characteristics. Subsequently, Kolmogorov–Smirnov and Shapiro–Wilk tests were carried out to verify the Gaussian distribution of the sampling means for the smallest group (RA[−]). Differences among PsA, RA[+] and RA[−] were then determined either by Student's t test or the Mann–Whitney U test, depending on the test result for Gaussian distribution. In order to evaluate the relationships of demographic characteristics (ie, gender, age, disease duration and body mass index) and disease-related parameters (ie, ACPA/RF positivity, glucocorticoid treatment) with BV/TV and TB.N, we set up two linear regression models—one for each of the aforementioned imaging parameters. All independent variables were included into the regression modelling by entering all variables at a single step. A dummy coding procedure was used in order to include multi-categorical variables properly. For the current mode of glucocorticoid therapy (categories: treatment with at least 7.5 mg/day for at least 3 months, low-dose treatment with a maximum of 5 mg/day for at least 3 months, no treatment) no treatment was chosen as the reference category, while for patient subgroups (categories: PsA, RA[–] and RA[+]), PsA was designated as the reference. Both reference categories formed the largest subgroup with respect to the corresponding characteristics. Additionally, a forward and backward regression for BV/TV and Tb.N were performed. A p value of less than 0.05 was considered as statistically significant.
Results
Demographic and disease-specific characteristics of RA and PsA patients
With respect to demographic parameters, such as age, height and body mass index, patients in the RA group were not different from the PsA group (table 1). For instance, the mean±SD age was 53.7±12.3 years in the RA group and it was 50.5±13.1 years in the PsA group. Furthermore, the two groups were comparable in disease-specific variables such as disease duration (RA: 9.1±8.4 years, PsA: 6.9±7.3 years), disease activity according to the DAS28 score (RA: 3.12±1.5, PsA: 3.09±1.4) and serum levels of C reactive protein. Also, modified HAQ scores were not significantly different between the two groups (table 1). ACPA and RF were found in 60% and 55% of RA patients, respectively. Both antibodies were found in 52% of the RA[–] and 82% of the RA[+] patients. None of the PsA patients showed a positive reaction for ACPA or RF. 38% of PsA patients had monoarticular or oligoarticular disease, and 62% had polyarticular disease. Daktylitis or a history of daktylitis was found in 24% of the PsA patients. Bone erosion was detected in 70% of the PsA patients and 72% of the RA patients. Non-traumatic fracture occurrence was similar in both groups.
Patient characteristics
With regards to antirheumatic therapy, the majority of patients received conventional or biological DMARD treatment, which was comparable between the RA and the PsA groups (table 1). The total number of previous and current DMARDs used in RA patients was higher than in PsA patients, most probably reflecting the higher abundance of effective drugs for RA as compared to PsA. Only few RA and PsA patients received glucocorticoid treatment at doses of more than 7.5 mg prednisolon equivalent (less than 10%). Use of low-dose glucocorticoid therapy was more frequent in RA (33%) than in PsA (10%). Six patients in the RA group received bisphosphonates, while none of the PsA patients did so (table 1).
Comparison of bone microstructure in RA and PsA patients
We first addressed whether the entire group of RA patients differed from PsA patients with respect to vBMD and bone microstructure. Surprisingly, no significant differences were found for vBMD, including total BMD (300±77 vs 316±62 mgHA/cm3), trabecular BMD (152±46 vs 165±40 mgHA/cm3) and cortical BMD (787±113 vs 818±76 mgHA/cm3) when comparing RA to PsA patients, respectively. Also, the parameters related to cortical and trabecular bone microstructure were not different between PsA and RA patients (table 2).
High-resolution peripheral quantitative CT results
Comparison of bone microstructure in RA[+] and PsA patients
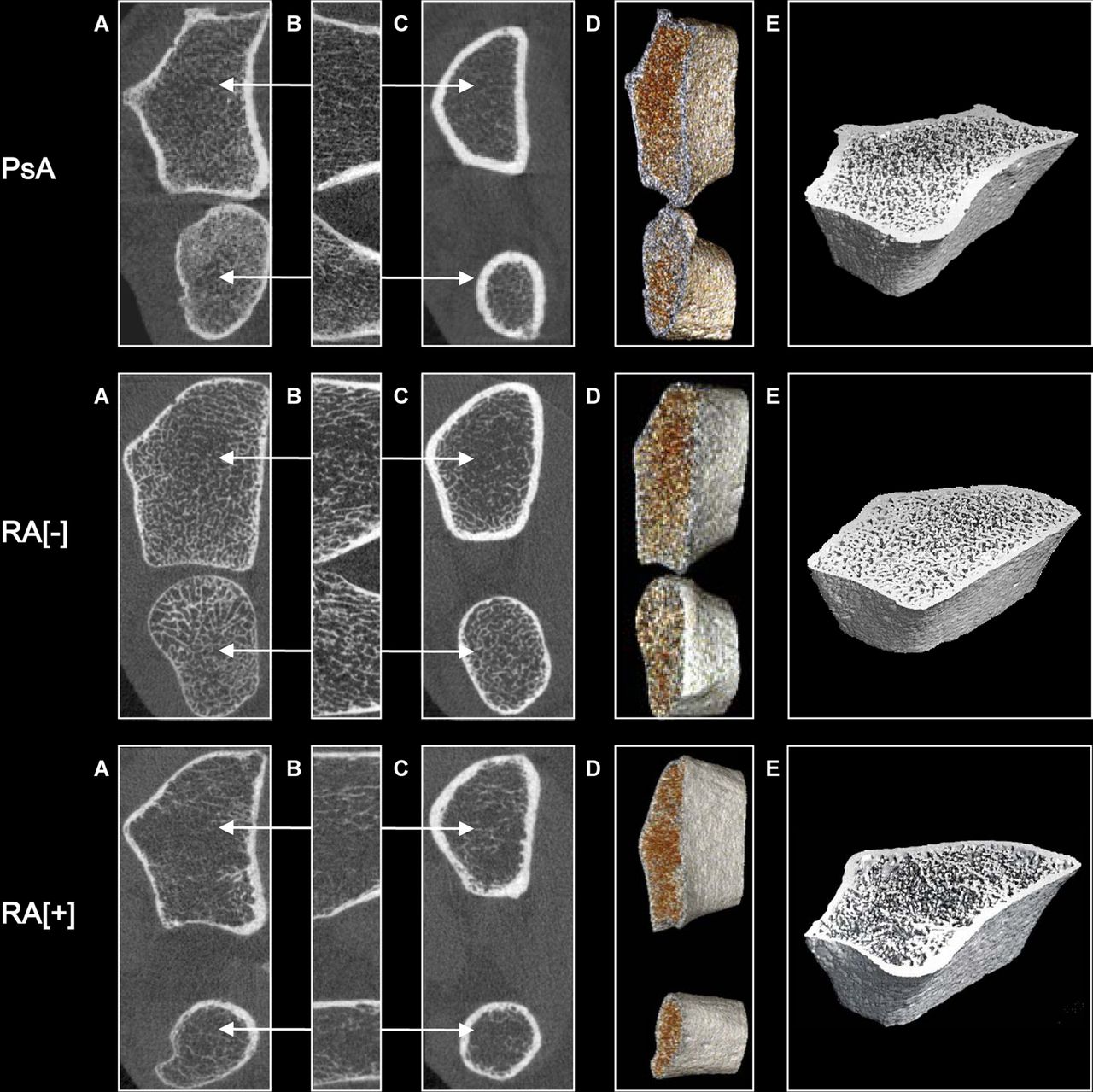
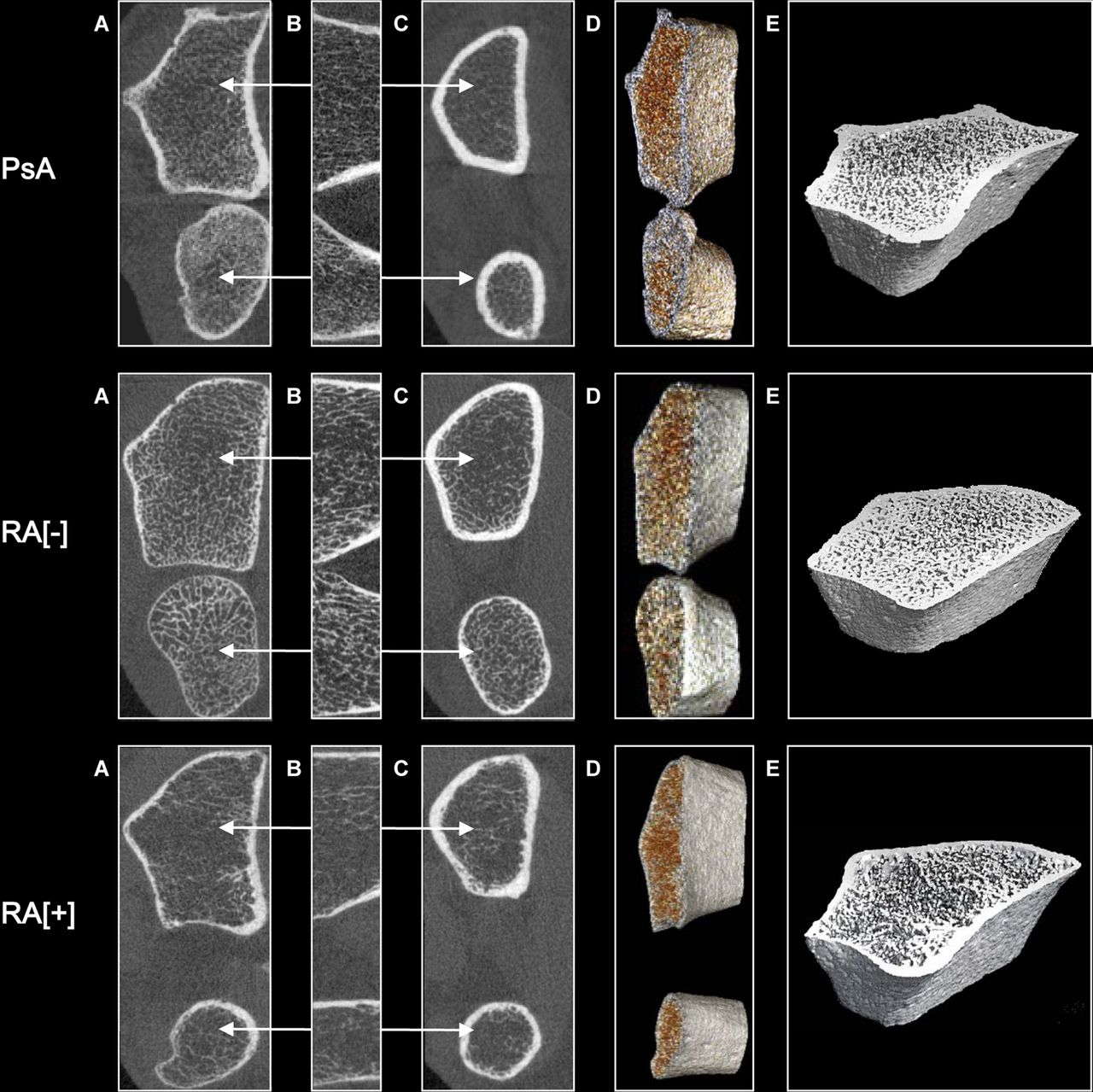
Based on recent findings on the importance of autoantibodies on bone,30 we decided to perform a separate analysis of RA[+] as well as RA[−]patients. RA[+] patients showed a significantly decreased total trabecular density (Δ15.2%), meta-trabecular density (Δ12.2%) and inner trabecular density (Δ19.3%) compared to PsA patients. In addition, the BV/TV (Δ14.6%) and the Tb.N (Δ10%) were significantly decreased in RA[+] patients. Furthermore, a strong trend towards higher Tb.Sp and inhomogeneity of the network was found in RA[+] patients compared with PsA patients. No differences were detected in Ct.Th, cortical density or Ct.Po between the two groups (all data are shown in table 2). Representative HR-pQCT scans of PsA, RA[+] and RA[−] patients are presented in figure 1.
{kind=link}
High-resolution peripheral quantitative CT scans of the distal radius (upper bone) and ulna (lower bone) of patients with psoriatic arthritis (PsA), seronegative rheumatoid arthritis (RA[−]) and seropositive rheumatoid arthritis (RA[+]). (A) Most distal slice, axial view; (B) total scan region of the 110 slices, coronar view; (C) most proximal slice, axial view; (D) three-dimensional (3D) reconstruction of the total scan region; (E) 3D reconstruction of the distal radius.
Comparison of bone microstructure in RA[+] and RA[−] patients
Similar results were found when the RA[+] group was compared to the RA[−] group. RA[+] patients showed significantly decreased total trabecular density (Δ17.9%), meta-trabecular density (Δ14.2%) and inner trabecular density (Δ25.1%) compared to RA[−] patients. Moreover, in RA[+] patients, BV/TV (Δ18.8%) and Tb.N (Δ14.2%) were significantly lower, and the Tb.Sp (Δ27%) was significantly higher than in RA[−] patients. Again, the cortical bone parameters did not differ between RA[+] and RA[−] patients.
Comparison of bone microstructure in RA[−] patients and PsA patients
Conversely, no differences were found between RA[−] and PsA patients regarding vBMD, and trabecular and cortical bone microstructure parameters, indicating that RA[−] patients, unlike RA[+] patients, have a bone microstructure that is similar to that of PsA patients.
Regression analysis
The regression model for BV/TV revealed significant relations to gender (β=−0.32, t=−3.56, p=0.001), age (β=−0.21, t=−2.27, p=0.025) and autoantibody positivity (β=−0.24, t=−2.28, p=0.025) when RA patients were compared to PsA patients as a reference (see table 3). All of these characteristics were inversely related to the dependent variable, implying that male gender, younger age and the absence of autoantibodies were related to higher values of BV/TV. Very similar results were found when performing a regression for Tb.N, revealing gender (β=−0.19, t=−2.01, p=0.047) and autoantibodies (β=−0.24, t=−2.20, p=0.030) as the factors determining Tb.N (table 3). Furthermore, in the backward regression model, significant relationships were found between BV/TV and gender (β=−0.35, t=−4.08, p<0.001), and between BV/TV and autoantibody positivity (β=−0.23, t=−2.67, p=0.009). Similar results were found for Tb.N and gender (β=−0.23, t=−2.46, p=0.016), and between Tb.N and autoantibody positivity (β=−0.22, t=−2.38, p=0.019; online supplementary table S1).
Regression models of selected high-resolution peripheral quantitative CT parameters
Discussion
In this study, we demonstrate that RA[+] patients have a bone structure that is different from that of RA[−] patients and PsA patients. Despite similar demographic variables, disease duration and activity, and antirheumatic therapy, RA[+] patients displayed more severe deterioration of the trabecular bone structure than RA[−] patients and PsA patients. In contrast, RA[−] patients were indistinguishable from PsA patients with respect to BMD, and trabecular and cortical bone structure. A multivariate logistic regression model supported the concept that the presence of autoantibodies, next to age and gender, is independently associated with trabecular bone loss and disturbed trabecular microarchitecture.
These data support the concept that RA[+] is a distinct disease entity and can be differentiated from RA[−] disease by its clinical presentation. It is already well known that the presence of autoantibodies such as ACPA and RF is associated with a higher risk for developing radiographic bone erosion.31 ,32 These lesions in the juxta-articular cortical bone result from direct exposure of the bone to synovial inflammatory tissue. In accordance with this observation, digital x-ray radiogrammetry of the hand of RA patients showed more pronounced loss of BMD in RA[+] patients than in RA[–] patients.33 Moreover, mechanistic data suggest that ACPA directly induces osteoclast differentiation and bone resorption.30 These data are additionally supported by the very recent findings that the mere presence of ACPA is associated with bone loss before the onset of inflammatory disease.34 In addition, the presence of autoantibodies such as ACPA and RF could be associated with a higher burden of inflammation. Indeed, the trend towards higher levels of C reactive protein (CRP) and higher DAS28 and HAQ scores in RA[+] patients compared to RA[−] and PsA patients could further enhance the risk for developing bone loss in this subgroup of patients. Whether ACPA or RF plays a more pronounced role in triggering bone loss, however, remains to be determined. Given the overlap of ACPA and RF positivity, which was 82% in our population, the differential effects of ACPA and RF are not easy to determine. Based on the data by Harre and colleagues, ACPA can directly influence bone, which provides a mechanism of how autoantibody positivity can trigger enhanced bone loss. However, this observation does not exclude the role of RF and the role of binding of immune complexes to Fc receptors. Preliminary evidence in bone erosion analysis suggests that RF indeed represents an enhancer of bone loss in ACPA-positive but not ACPA-negative RA patients, but further research is needed to address the role of RF.
So far, trabecular bone architecture has been inadequately examined in patients with inflammatory arthritis. No study has been performed in PsA and only one study has been carried out in RA patients which focused on a subsegment of RA patients. Zhu and colleagues found that vBMD and BV/TV were decreased and trabecular inhomogeneity was increased in women with RA compared to those without RA.35 Although this study confirmed the notion that RA is associated with trabecular bone loss, the results can hardly be generalised based on the exclusive assessment of women, the lack of information about the autoantibody status and the fact that only a very few patients received biological drug therapy, which is now widely used for the treatment of RA and PsA patients in many countries. Furthermore, it is particularly interesting to compare RA and PsA patients with respect to trabecular bone structure, since these diseases share a chronic course but differ profoundly in their pathophysiology, for instance in their cytokines mediators apart from TNF. Moreover, RA and PsA are profoundly different with respect to periarticular bone architecture with many more bony proliferations in PsA than in RA.26
In the present study, trabecular vBMD and BV/TV were significantly decreased in RA[+] patients as compared to their RA[−] counterparts, as well as to PsA patients. Trabecular bone loss affected the central marrow region and the peripheral region adjacent to the cortical bone. Moreover, we assessed bone quality, since alterations of trabecular density and microstructure are associated with a higher risk for peripheral fractures.36 Indeed, we found decreased Tb.N associated with higher Tb.Sp and inhomogeneity in RA[+] patients compared to their RA[−] counterparts and PsA patients. These data suggest that bone quantity and bone quality are decreased in RA[+] patients.
Aside from the presence of autoantibodies, gender and age were the key factors determining bone structure in patients with RA and PsA, which supports the robustness of the analyses, as both factors strongly influence bone quantity and quality. Further research, however, is needed to better understand the interactions of the individual variables determining bone loss in patients with RA and PsA. For instance, it was stunning that despite the well-described negative effects of glucocorticoids on the skeleton,37 the use of low-dose glucocorticoids (5 mg prednisolone or less) positively rather than negatively influenced Tb.N. However, the most likely explanation for this finding is the anti-inflammatory effect of low-dose glucocorticoids, which counteracts inflammation-dependent bone loss and beneficially influences bone quality, as previously demonstrated by others.12 ,38
Cortical bone is a main component of bone strength. In peripheral sites, especially intracortical porosity in particular seems to play a crucial role in bone fragility.39 It was suggested that even small changes in Ct.Po more strongly affect bone stiffness than changes in the trabecular bone.40 Little is known about cortical bone changes in patients with RA apart from bone erosion and cortical bone loss in the phalangeal bones, as assessed by Dual-energy x-ray absorptiometry.41 Zhu and colleagues reported that Ct.Po is increased in women with compared to those without RA.35 In our study we did not find major differences in cortical density, Ct.Th or Ct.Po among RA[+], RA[−] and PsA subjects, suggesting that cortical bone changes are shared by various different inflammatory joint diseases. On the other hand, we could find a trend towards lower Ct.Th in RA patients compared to PsA patients; Ct.Th was, in fact, lowest in RA[+] patients, suggesting that also cortical bone is affected by the autoimmune processes in RA patients.
In conclusion, these data show that RA[+] patients face the most profound changes in trabecular bone. ‘RA’ represents a mixed population with respect to bone composition and, if not stratified for autoantibody status, RA has a very similar trabecular BMD and micro-architecture to that of PsA. Our observations, as well as previous data, suggest that the impact of inflammation on bone is similar in RA and PsA. However, autoantibodies are an additional factor aggravating bone loss in arthritis. In fact, (1) the observation of occurrence of osteopenia very early in the disease course of RA,33 and (2) the detection of cortical bone changes in the periarticular bone of autoantibody-positive healthy individuals34 and the functional properties of ACPA to stimulate osteoclastogenesis30 all support the specific bone phenotype of RA[+] patients.
Acknowledgments
The authors thank Tommy Vacca and Annemarie Kocijan for proofreading.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online table
Footnotes
-
Handling editor Tore K Kvien
-
Contributors RK, SF and ME collected and analysed the data. RK, JR, SF and GS designed the study. RK and G S wrote the manuscript. KE and JR, revised the manuscript.
-
Funding Roland Kocijan was supported by a postdoctoral research fellowship from the Bayerische Forschungsstiftung. This study was supported by the Deutsche Forschungsgemeinschaft (SPP1468-IMMUNOBONE), the Bundesministerium für Bildung und Forschung (project ANCYLOSS) and the TEAM and MASTERSWITCH projects of the European Union and the Innovative Medicines Initiative-funded project BTCure.
-
Competing interests None.
-
Ethics approval Local ethics committee University Erlangen–Nuremberg.
-
Provenance and peer review Not commissioned; externally peer reviewed.