Article Text

Abstract
Objective To describe clinical outcomes of juvenile idiopathic arthritis (JIA) in a prospective inception cohort of children managed with contemporary treatments.
Methods Children newly diagnosed with JIA at 16 Canadian paediatric rheumatology centres from 2005 to 2010 were included. Kaplan–Meier survival curves for each JIA category were used to estimate probability of ever attaining an active joint count of 0, inactive disease (no active joints, no extraarticular manifestations and a physician global assessment of disease activity <10 mm), disease remission (inactive disease >12 months after discontinuing treatment) and of receiving specific treatments.
Results In a cohort of 1104 children, the probabilities of attaining an active joint count of 0 exceeded 78% within 2 years in all JIA categories. The probability of attaining inactive disease exceeded 70% within 2 years in all categories, except for RF-positive polyarthritis (48%). The probability of discontinuing treatment at least once was 67% within 5 years. The probability of attaining remission within 5 years was 46–57% across JIA categories except for polyarthritis (0% RF-positive, 14% RF-negative). Initial treatment included joint injections and non-steroidal anti-inflammatory drugs for oligoarthritis, disease-modifying antirheumatic drugs (DMARDs) for polyarthritis and systemic corticosteroids for systemic JIA.
Conclusions Most children with JIA managed with contemporary treatments attain inactive disease within 2 years of diagnosis and many are able to discontinue treatment. The probability of attaining remission within 5 years of diagnosis is about 50%, except for children with polyarthritis.
- Epidemiology
- Juvenile Idiopathic Arthritis
- Outcomes research
- Treatment
Statistics from Altmetric.com
Introduction
At the time of diagnosis of juvenile idiopathic arthritis (JIA), families have many questions about the prognosis of their child, treatments that may be required and their potential side effects. Despite numerous studies, our ability to answer these questions remains limited.1–3 In a systematic review of 21 papers published before 2005, Adib et al concluded the prognosis of JIA remained unclear, but that overall, children with oligoarthritis had a better prognosis.3 Only three papers were prospective and only one followed patients systematically from disease diagnosis. Most children were diagnosed before newer disease-modifying antirheumatic drugs (DMARDs) and biological agents were widely used to treat JIA.
International League of Associations for Rheumatology (ILAR) criteria classify children with JIA into seven categories based on clinical manifestations and laboratory tests.4 Current practice recommendations propose use of medications tailored according to JIA category5 or according to treatment groups defined by the number of joints affected and features of poor prognosis.6 In general, initial treatment with intra-articular corticosteroids and non-steroidal anti-inflammatory drugs (NSAIDs) is recommended for JIA affecting a few joints, while DMARDs followed by biological agents if DMARDs fail to bring the disease under control are recommended for polyarthritis and for children with features of poor prognosis.5 ,6
Previous reviews highlighted shortcomings of retrospective studies and called for prospective studies with standardised outcomes.1–3 Data from recent prospective cohorts suggest that early improvement is achievable in many patients7 and that the frequency of disease remission varies substantially with JIA category.8
The aim of the present descriptive analysis is to report JIA clinical outcomes in a prospective inception cohort of children managed with contemporary treatments in order to better counsel families of newly diagnosed patients. The specific objectives are (1) to estimate the probabilities of ever attaining an active joint count of 0, inactive disease and disease remission within the first 5 years after diagnosis, and (2) to describe treatments used in this cohort.
Methods
The methods of the Research in Arthritis in Canadian Children emphasizing Outcomes study (ReACCh-Out) have been described previously.9 Briefly, from January 2005 to December 2010, ReACCh-Out recruited consecutive patients diagnosed with JIA at all 16 paediatric rheumatology referral centres across Canada. Comprehensive study visits occurred at 0, 6, 12, 18, 24, 36, 48 and 60 months after enrolment. Data collected consisted of demographic and clinical information, juvenile arthritis core variables,10 medications and quality-of-life measures.11 ,12 Centres were required to report active joint count, enthesitis count, physician global assessment of disease activity measured in a 100 mm visual analogue scale (PGA) and medications at all other clinic visits (interim visits). Treatment was at the discretion of the paediatric rheumatologist and the family. The study was approved by the research ethics boards at each institution and carried out in conformity with the Declaration of Helsinki. Informed consent was obtained from parents, and assent from participants as appropriate for age.
For the present report, we included children enrolled in ReACCh-Out within 6 months of diagnosis who had active disease at enrolment as defined below and at least one follow-up visit.
Definitions
Date of diagnosis was the date the paediatric rheumatologist established a diagnosis of JIA. Date of attaining an active joint count of 0 was the date of the first visit when no active joints were found on examination. Active joint was defined as swelling within a joint or limitation of movement with joint pain or tenderness.4 Inactive disease was defined as an active joint count of 0, absence of systemic manifestations in those with systemic arthritis, absence of enthesitis in those with enthesitis-related arthritis (ERA) or psoriatic arthritis, absence of uveitis and a PGA <10 mm. This definition was based on that of Wallace et al, with modifications.13 Date of treatment discontinuation was the date when all antirheumatic and antiuveitis medications were first discontinued, if known, otherwise it was the date of the visit when the patient was first reported to be off medications. Disease remission was defined as at least 12 months of inactive disease after discontinuation of all medications. Data from interim visits were reviewed to verify absence of medication use, active joints and enthesitis, and that the PGA remained <10 mm. The date of extension in patients with oligoarthritis was the date of the visit when the site investigator reported the disease had extended as per ILAR criteria.4
Inactive disease and disease remission status were assigned by three investigators based on the above definitions. JIA category assignments were reviewed to confirm that they conformed to ILAR criteria.4 Medications were categorised as NSAIDs, DMARDs, biological agents, systemic corticosteroids, intra-articular corticosteroids and ophthalmic corticosteroids. Mydriatics or medications to reduce intraocular pressure were not considered active uveitis treatment.
The online supplementary appendix describes the process for verifying JIA categories and attainment of outcomes.
Analysis
For each JIA category, survival tables and Kaplan–Meier survival curves were constructed from the date of diagnosis (time 0) to estimate the cumulative probabilities of attaining an active joint count of 0, inactive disease and disease remission using SPSS software V.20. Survival curves were also constructed to estimate the cumulative probabilities of starting DMARDs, biological agents, systemic corticosteroids and intra-articular corticosteroids. The probabilities of discontinuing all treatments and of extension in patients with oligoarthritis were estimated the same way. Data on each subject were analysed until the occurrence of the outcome of interest or until their last available visit by the study end date for this report (30 June 2011). When the outcome of interest had not occurred and the status of the outcome was indeterminate at the last visit because of missing information, the preceding visit date was used as the censoring date for that subject; the last observation was not carried forward. This occurred in 1 (0.1%) and 15 (1.5%) cases, respectively, in the analyses for inactive disease and disease remission (see online supplementary appendix).
Results
The ReACCh-Out study recruited 1497 patients with JIA between January 2005 and December 2010. Study visits continued at all centres until 30 June 2011. Five patients were excluded from this report because there was insufficient information to assign a JIA category; 126 because they had no follow-up visits after enrolment, 156 because they were enrolled >6 months after diagnosis and 106 because they had inactive disease at enrolment. Thus, 1104 patients were included (table 1). Median time from diagnosis to study enrolment was 0.3 (IQR 0–1.6) months. The number of subjects in the cohort at each time interval in each ILAR category is reported in the online appendix. Forty-two patients withdrew from the study at a median of 18.2 (IQR 7.7–30.7) months. Their data to the time of withdrawal are included.
Characteristics of patients in the cohort by juvenile idiopathic arthritis category*
Disease outcomes
Survival curves for attaining an active joint count of 0, inactive disease, treatment discontinuation and disease remission are shown in figure 1. Overall, 1007 children attained an active joint count of 0 for the first time during the study, at a median of 7.0 (IQR 3.5–13.3) months after diagnosis. All JIA categories had >78% probability of attaining an active joint count of 0 at least once within 2 years of diagnosis.
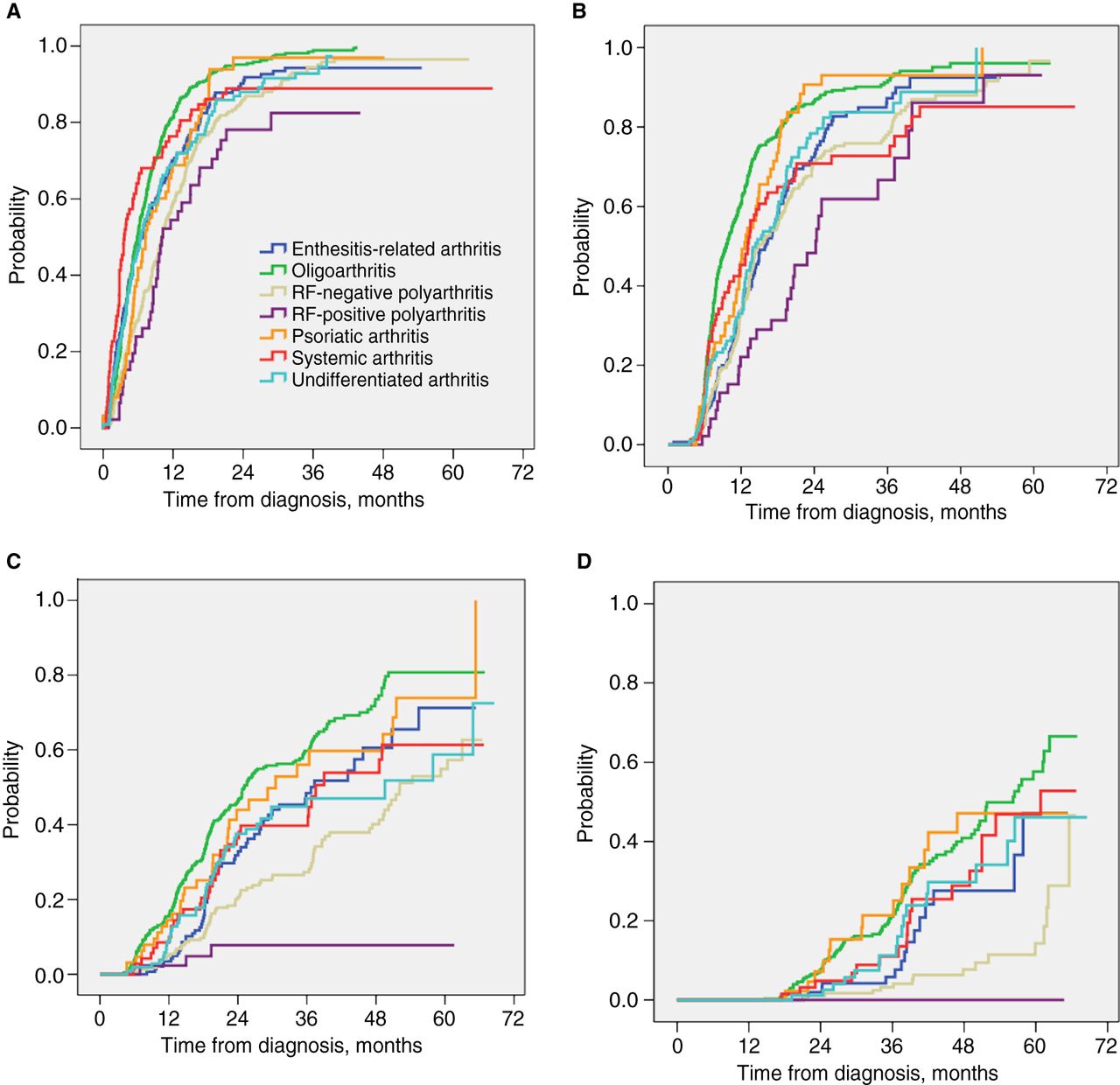
Outcomes in seven categories of juvenile idiopathic arthritis. Shown are Kaplan–Meier estimates of the probability of (A) attaining a joint count of 0, (B) attaining inactive disease, (C) discontinuing antirheumatic treatment due to inactive disease and (D) attaining remission off medications. Time 0 is time of diagnosis.
Inactive disease was attained by 883 children at a median of 13.0 (IQR 7.7–21.7) months after diagnosis. The probability of attaining inactive disease within 2 years ranged from 48% for patients with RF-positive polyarthritis to 91% for patients with psoriatic arthritis (figure 1B, table 2). Eleven children did not achieve inactive disease status due to persistent uveitis.
Cumulative probabilities of attaining inactive disease within 1, 2, 3, 4 and 5 years after diagnosis
Overall, 478 children with inactive disease stopped treatment at a median of 37.3 (IQR 18.7–65.3) months after diagnosis. They were followed for a median of 16.6 (IQR 6.7–28.5) months after treatment discontinuation. The probability of discontinuing all medications at least once within 5 years of diagnosis ranged from 8% for RF-positive polyarthritis to 81% for oligoarthritis (figure 1C, table 3).
Cumulative probabilities of discontinuing all antirheumatic and antiuveitis treatment because of inactive disease within 1, 2, 3, 4 and 5 years after diagnosis
During follow-up, 178 children attained disease remission. The probability of attaining remission varied among JIA categories (figure 1D, table 4). Within 5 years, children with oligoarthritis had the highest probabilities of remission (57%), and children with RF-positive polyarthritis had the lowest (0%).
Cumulative probabilities of attaining disease remission within 2, 3, 4 and 5 years after diagnosis
Among 416 children with oligoarthritis at enrolment, 76 developed extended oligoarthritis during the study. The probability of extension was 8.3, 15.6, 18.7, 21.6 and 24.4% within 1, 2, 3, 4 and 5 years of diagnosis, respectively (online appendix). Virtually all patients with oligoarthritis who attained remission had a persistent oligoarthritis (98 of 99).
Treatments
Survival curves for starting DMARDs, biological agents and corticosteroids are shown in figure 2. Most children received NSAIDs at enrolment (88%). A total of 608 children started DMARDs during the study, including most children with RF-positive polyarthritis (93%) and RF-negative polyarthritis (83%). These patients received their first DMARD at a median of 0.3 (IQR 0–1.5) and 1.5 (IQR 0.03–7.7) months after diagnosis, respectively. Children with systemic JIA received DMARDs later (median 3.5, IQR 0.6–56.5 months), while DMARD usage was substantially lower in other JIA categories (figure 2A).

{kind=link}
{kind=link}
Treatments in seven categories of juvenile idiopathic arthritis. Shown are Kaplan–Meier estimates of the probability of starting (A) disease-modifying antirheumatic drugs, (B) biological agents, (C) systemic corticosteroids and (D) intra-articular corticosteroids. Time 0 is time of diagnosis. Most patients received nonsteroidal anti-inflammatory drugs at diagnosis.
Overall, 129 patients started biological therapies during the study (figure 2B). The probabilities of starting a biological agent within 6 months of diagnosis were 11.1% in children with RF-positive polyarthritis and 5.3% in children with systemic JIA. Biological agents were used infrequently in children with oligoarthritis (6.6% within 5 years). There was a trend to start biologics earlier in children diagnosed at later dates (Spearman's correlation coefficient −0.489, p<0.0001).
The probabilities of starting systemic corticosteroids within 6 months of diagnosis were 79% and 61% in systemic JIA and RF-positive polyarthritis, respectively (figure 2C). Intra-articular corticosteroids were used most often in oligoarthritis and least often in systemic JIA (figure 2D). Triamcinolone hexacetonide was the most commonly used preparation (96% of all injections).
The online supplementary appendix reports probabilities of receiving each treatment in each JIA category and the specific DMARDs and biologics used.
Adding to the cohort the 106 patients who had inactive disease at enrolment did not significantly change our findings (see online supplementary appendix).
Discussion
We used data from a large inception cohort of children with JIA to estimate the probabilities of attaining positive clinical outcomes within 5 years of diagnosis. Probabilities of attaining an active joint count of 0 and a state of inactive disease increased quickly during the first 2 years. The probability of attaining remission off medications was about 50% within 5 years, except for children with polyarthritis. Overall, children with oligoarthritis or psoriatic arthritis had the best outcomes; however, the latter received more aggressive treatment. Children with RF-positive polyarthritis had the worst outcomes but they still had about a 90% probability of attaining inactive disease at least once within 5 years after diagnosis.
Comparing our data with other prospective cohorts requires caution because of differences in outcome definitions, treatments and statistical methods. Nordal et al8 reported that 70% of 390 patients with JIA had at least one period of remission off medications during a median follow-up of 98 months. Selvaag et al14 reported an overall 28% remission rate at 3 years, defining remission as inactive disease off medications for only 6 months. Our findings are consistent with the 1-year median active joint counts reported in a prospective cohort in Britain.15 These prospective cohorts have not reported Kaplan–Meier estimates for attaining outcomes.
Comparison with earlier retrospective studies requires even greater caution. Oen et al16 reported probabilities of remission similar to our present data, after considering differences in diagnostic criteria and definitions of remission. In a retrospective single-centre study, Wallace et al17 observed higher remission rates. Applying ILAR criteria retrospectively, Flato et al reported 44% of patients with ERA and 55% with psoriatic arthritis were in remission 15 years after diagnosis.18 ,19 Our survival curves project numerically similar probabilities of remission within 5 years. A recent retrospective cohort from the Netherlands reported similar chance of attaining inactive disease within 2 years as our whole cohort (77%). Patients with RF-negative polyarthritis were overrepresented in that cohort and 95% of children received DMARDs.20
The lower probabilities of attaining remission compared with high probabilities of attaining inactive disease may be due to continued treatment of inactive patients, disease flares or a short observation period after discontinuing treatment. Further analysis of our data and longer follow-up may help quantify the relative impact of these three factors.
In our cohort, the probability of extension in children with oligoarthritis was less than 25% within 5 years of diagnosis, somewhat lower than the 30–35% frequency of extension previously reported.8 ,17 ,21 This could be due to differences in length of follow-up, treatment or intrinsic aggressiveness of the disease across populations.
Children with RF-positive polyarthritis in our cohort rarely discontinued treatment, suggesting disease remission off medications may not be an achievable goal in this JIA category despite early use of DMARDs and frequent use of biological agents. These children had substantially different outcomes to children with RF-negative polyarthritis, suggesting they should be considered separately in clinical trials.22 ,23
Study strengths and limitations
This is the largest prospective inception cohort of children with JIA published to date, and study subjects were recruited during a narrow window of 6 years. Treatments received by this cohort are largely consistent with current practice recommendations,5 ,6 ,24 although the recommendations were published after study recruitment and our study did not dictate the treatments used. The only difference may be a later use of biological therapies for those with poor prognostic features.6 ,24 The use of biological agents in our cohort and in current treatment recommendations is less aggressive than in recent trials of early treatment22 ,23 and a cross-sectional report from the USA.25 Our study shows that relatively conservative use of biological agents is compatible with achievement of inactive disease in the majority of children with JIA. However, even within our 6-year recruitment window, we found a trend for earlier use of biologics in patients diagnosed at later dates, showing that treatment of JIA is evolving.
One limitation of our study is that our definition of inactive disease differs from a recently published consensus definition of inactive disease26 in that we required absence of enthesitis in children with ERA and psoriatic arthritis; used a PGA of <10 mm, rather than 0, as indicative of the best possible score; and did not require normal levels of acute phase reactants (measured only when clinically indicated) or a morning stiffness <15 min. We defined remission as inactive disease for a year or more after treatment discontinuation, as recommended.26 Other authors have also used a PGA of <10 mm as indicative of inactive disease,27 ,28 excluding small values that could be marking errors or simply physicians’ avoidance of the edge of the scale. Others have also disregarded the requirement for normal levels of acute phase reactants when studying patients in clinical practice.29
Our results may not apply to all children with JIA because some children may not be referred to paediatric rheumatologists and some patients did not consent to or withdrew from the study. Paediatric rheumatology services are available in every major Canadian city free of charge and referral of all JIA patients is encouraged, but we cannot ensure all patients were referred. We decided to exclude from this report children with inactive disease at enrolment and those diagnosed more than 6 months earlier to approximate the clinical situation of a patient just diagnosed with JIA. These factors and decisions may have biased the cohort towards increased disease severity, although inclusion of patients with inactive disease at enrolment in secondary analyses did not change our findings. Overall, our data seem representative of patients with active JIA newly diagnosed by a paediatric rheumatologist in Canada.
Kaplan–Meier survival table methods make use of most of the information available in our cohort. Kaplan–Meier estimates are robust when there is a substantial number of subjects remaining under observation (usual guidance is >20).30 Therefore, our estimates at 4 or 5 years for the smaller categories of JIA should be interpreted with caution. We report probabilities of attaining clinical outcomes, and our results should not be interpreted as the probabilities of maintaining these outcomes.
Implications for practice
While treatment approaches will continue to evolve, our data show that children recently diagnosed with JIA in Canada can expect the following: (1) irrespective of their JIA category and differences in treatment, they will have roughly a 70–90% chance of attaining inactive disease by 2 years unless they have RF-positive polyarthritis; (2) they will likely receive intra-articular corticosteroids, and if they have systemic JIA or RF-positive polyarthritis they will likely receive systemic corticosteroids; (3) they have a less than 20% chance of receiving biological agents within 5 years of diagnosis unless they have RF-positive polyarthritis or systemic JIA; (4) it will take an average of 3 years to the first attempt at discontinuing all treatment and, except for those with polyarthritis, there is about a 50% chance of remission; (5) children with oligoarthritis have about a 40% chance of receiving DMARDs, about a 40% chance of experiencing remission and a 20% chance of extension within 4 years of diagnosis; and (6) children with RF-positive polyarthritis will likely receive DMARDs and biological agents and will eventually attain inactive disease, but they are unlikely to discontinue treatment within 5 years of diagnosis. Children in other countries receiving similar care may experience similar outcomes.
Conclusions
In conclusion, Canadian children with JIA diagnosed between 2005 and 2010 had high probabilities of attaining a joint count of 0 and a state of inactive disease at least once within 2 years after diagnosis, while receiving treatment largely in keeping with present treatment recommendations. Many were able to discontinue treatment, and the probability of remission off medications within 5 years of diagnosis was about 50%, except for those with polyarthritis.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
Handling editor Tore K Kvien
JG and KO contributed equally.
Collaborators Additional members of the Research in Arthritis in Canadian Children emphasizing Outcomes Study (ReACCh-Out): Dr Roxana Bolaria and Dr Katherine Gross, University of British Columbia; Dr Brian Feldman, Dr Debbie Feldman and Dr Bonnie Cameron, Hospital for Sick Children and University of Toronto; Dr Roman Jurencak and Dr Johannes Roth, Children's Hospital of Eastern Ontario and University of Ottawa; Dr Jean Dorval, Centre Hospitalier Universitaire de Laval and Université Laval, Quebec; Dr Claire LeBlanc, McGill University Health Centre and McGill University, Montreal; Dr Claire St. Cyr, CHU Ste. Justine and Université de Montréal, Montréal; all in Canada.
Contributors CMD, KO, LBT and RY designed the original study and were the principal investigators who obtained the research grant. JG, KO and AMH verified achievement of outcomes and quality of the data used in the analysis. KO conducted statistical analysis with assistance by JG. JG and KO drafted the manuscript and coordinated revisions to the manuscript; they contributed equally as first authors. All named authors (1) provided substantial contributions to conception and design, acquisition of data or analysis and interpretation of data; (2) revised the manuscript for important intellectual content and (3) approved of the version to be published.
Funding This study was funded by a New Emerging Team research grant from the Canadian Institutes of Health Research.
Competing interests None.
Ethics approval Research Ethics Boards at each participating institution.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Additional tables reporting probabilities of receiving specific treatments in each JIA category are included in the online appendix. Access to unpublished data may be granted to other investigators provided that (1) they collaborate in a team that includes at least one ReACCh-Out investigator, and (2) their research protocol is approved by the Canadian Alliance of Pediatric Rheumatology Investigators Scientific Protocol Evaluating Committee. For more details, contact Dr Jaime Guzman at jguzman@cw.bc.ca.