Article Text

Abstract
Objective Epidemiological studies of primary Sjögren's syndrome (pSS) are crucial for describing the burden to society and the public medical system and for shedding light on aetiology. Previous reports of the epidemiology of pSS show variable outcomes. We conducted a systematic review of the epidemiology of pSS to assess the prevalence rates (PRs) and incidence rates (IRs), and to investigate possible geographic variations in pSS.
Methods A systematic literature search of PubMed and Embase (updated to 22 October 2013) was performed to identify all published reports on the epidemiology of pSS. The incidence and prevalence rates of pSS were summarised with IRs or PRs and 95% CIs.
Results The literature search yielded 1880 related citations. Only 21 fulfilled the inclusion criteria. According to a random-effects model, the pooled IR for pSS was 6.92 (95% CI 4.98 to 8.86) per 100 000 person-years. The overall PR was 60.82 (95% CI 43.69 to 77.94) cases per 100 000 inhabitants with a slightly lower estimate of Baodong Qin is BDQ, Jiaqi Wang is JQW, Zaixing Yang is ZXY, Renqian Zhong is RQZ. 43.03 (25.74 to 60.31) cases per 100 000 inhabitants when only considering population-based studies. The female/male ratio in incidence data was 9.15 (95% CI 3.35 to 13.18). The female/male ratio in prevalence data was 10.72 (95% CI 7.35 to 15.62). The overall age of pSS patients was 56.16 years (95% CI 52.54 to 59.78).
Conclusions Incidence and prevalence rates of pSS vary widely around the world. The results help us better understand the global epidemiology of pSS. Large population-based studies combining meticulous case-finding and case-ascertainment strategies are needed.
- Sjögren's Syndrome
- Epidemiology
- Autoimmune Diseases
Statistics from Altmetric.com
Introduction
Primary Sjögren's syndrome (pSS) is a slowly progressive autoimmune disorder characterised by lymphocytic infiltration of the exocrine glands and significant loss of secretory function with oral and eye dryness.1 pSS affects predominantly middle-aged women, typically in the fourth to sixth decades of life.2 Since the first observation of pSS, intense research efforts have been made to understand the pathological aspects, but the aetiology is still not well understood.3––5 To aid in the accurate diagnosis of pSS, several sets of diagnostic criteria have been proposed.6
Incidence and prevalence are two important indicators in the epidemiology of the disease. Incidence is a measure of the risk of developing some new pSS cases within a specified period of time, while prevalence is the proportion of a population found to have pSS. Insight into the incidence and prevalence of pSS would be advantageous to describe the burden of the disease and to better understand its aetiology. Several studies have investigated the incidence and prevalence of pSS, but there were inconsistencies owing to different case-finding, case-ascertainment and populations under study. Until now, epidemiological studies of pSS have not been systematically summarised. In the present study, we systematically reviewed the literature regarding incidence and prevalence rates and conducted a meta-analysis to provide recommendations for future studies describing the epidemiology of pSS.
Methods
Search strategy
We conducted a systematic literature search with a predetermined protocol according to guidelines set by Meta-analysis of Observational Studies in Epidemiology (MOOSE).7 We performed a systematic review of the electronic databases including PubMed and Embase (updated October 2013). The PubMed comprehensive search strategy included the Mesh terms and keywords ("Sjögren's Syndrome"[Mesh]) and ("Epidemiology"[Mesh] or epidemiol* or "Incidence"[Mesh] or Incidenc* or "Prevalence"[Mesh] or Prevalenc*). The BDQ, JQW, ZXY search strategy used in EMBASE included ((exp Sjögren's Syndrome) or (Sjögren's Syndrome)) and ((exp Epidemiology) or epidemiol or (exp Incidence) or Incidenc* or (exp Prevalence) or Prevalenc*)). The search was limited to English language, but no limitation was placed on ethnicity or human subjects. The reference lists of relevant articles were also reviewed.
Study selection
Population-based studies and population surveys aiming to examine an entire geographic region or using a clearly defined random or clustered sampling procedure were included. Reports consisting of surveys or audits in hospitals or clinics were excluded. Studies were eligible for inclusion if they reported incidence ratio (IR), prevalence ratio (PR) or enough data relevant to the outcomes of interest to calculate them. Studies that did not report sufficient published data or original data were excluded. This included reviews, abstracts and letters. Studies conducted in special populations were excluded. The final results were compared by two authors (QBD and WJQ) and any disagreements were resolved by consensus with the third-party authors (MY, YZX and ZRQ).
Data extraction
The primary variables of interest were the prevalence and incidence of pSS. The prevalence rate data included the number of patients with pSS and number of inhabitants recorded for individual years when they were reported. The incidence rate per 100 000 person-years with 95% CI was documented for the overall study period. Secondary variables extracted from the articles included country of origin, study period, age, male/female incidence rate ratio (IRR), the methods of case finding, study design and case ascertainment.
Assessment of study quality
A population-based study is a study of the entirety from the general population in a defined region using the administrative database or hospital medical records.8 And sample survey describes the process of choosing a sample of individuals from a target population often using questionnaire. Bias in sample survey is undesirable but unavoidable including non-response bias, coverage bias and selection bias. To some extent, the population-based study could avoid those bias and provide a more accurate epidemiological data of pSS. Due to the lack of standardised quality criteria for meta-analyses of epidemiology studies, evaluation of study quality was based on the method of case-finding method, the study design and the method of case ascertainment. The study quality was considered ‘good’ when the study design was based on population. The case-finding method included administrative databases or hospital medical records. A well-directed case ascertainment was established using internationally accepted diagnostic criteria. Study quality was classified to be ‘moderate’ when the study design was a population survey or the case-finding method was a questionnaire and clinical examination; the case-ascertainment method was inadequate for the diagnosis of pSS. If case finding or case ascertainment was not performed, the quality of a study would identified to be ‘poor’.9
Statistical analysis
The incidence and prevalence of pSS was summarised using IR and PR. These were defined as the number of pSS patients in a population per 100 000 person-years and per 100 000 persons, respectively. IRs and PRs adjusted for confounding factors were preferred over unadjusted values. The 95% CI for IRs and PRs were estimated under the assumption of a Poisson distribution. The female to male ratio was summarised with an Incidence Rate Ratio (IRR) and Prevalence Rate Ratio (PRR). This was defined as the IR and PR of pSS in women over the IR and PR of pSS in men. When the IRR and PRR were not reported but the number of female and male pSS patients and the total study population were included, the IRR or PRR were calculated using the assumption that ratio of women to men in the background population was 1:1.10 The overall rates and 95% CI were calculated using a random effect. Heterogeneity of effects among studies was estimated using the Q test and quantified by using the I2 test.11 ,12 Meta-regression analysis was used to identify the potential source of heterogeneity if there were sufficient number of studies. Subgroup analysis was conducted according to the method of case ascertainment, study design or case finding. Funnel plots and the Egger's test were used to determine the possibility of publication bias. Sensitivity analysis was performed to evaluate the degree that each single study affected the overall PR or IR using the one-study remove approach. All statistical analyses were done using Comprehensive meta-analysis software V.2.0 (Biostat Inc, Englewood Cliffs, New Jersey, USA) (http://www.meta-analysis.com). p Values less than 0.05 were considered significant.
Results
Studies selection
A total of 1880 non-overlapping citations were identified and screened from the previously described electronic databases. A total of 1808 articles were excluded based on screening of abstracts or titles, leaving 72 articles for the full-text review and assessment for eligibility. Fifty-one of these articles were excluded after retrieving the full-text articles (figure 1), leaving 21 eligible studies for inclusion in the meta-analysis.13––33 The agreement between reviewers for the eligibility of articles was 100%.
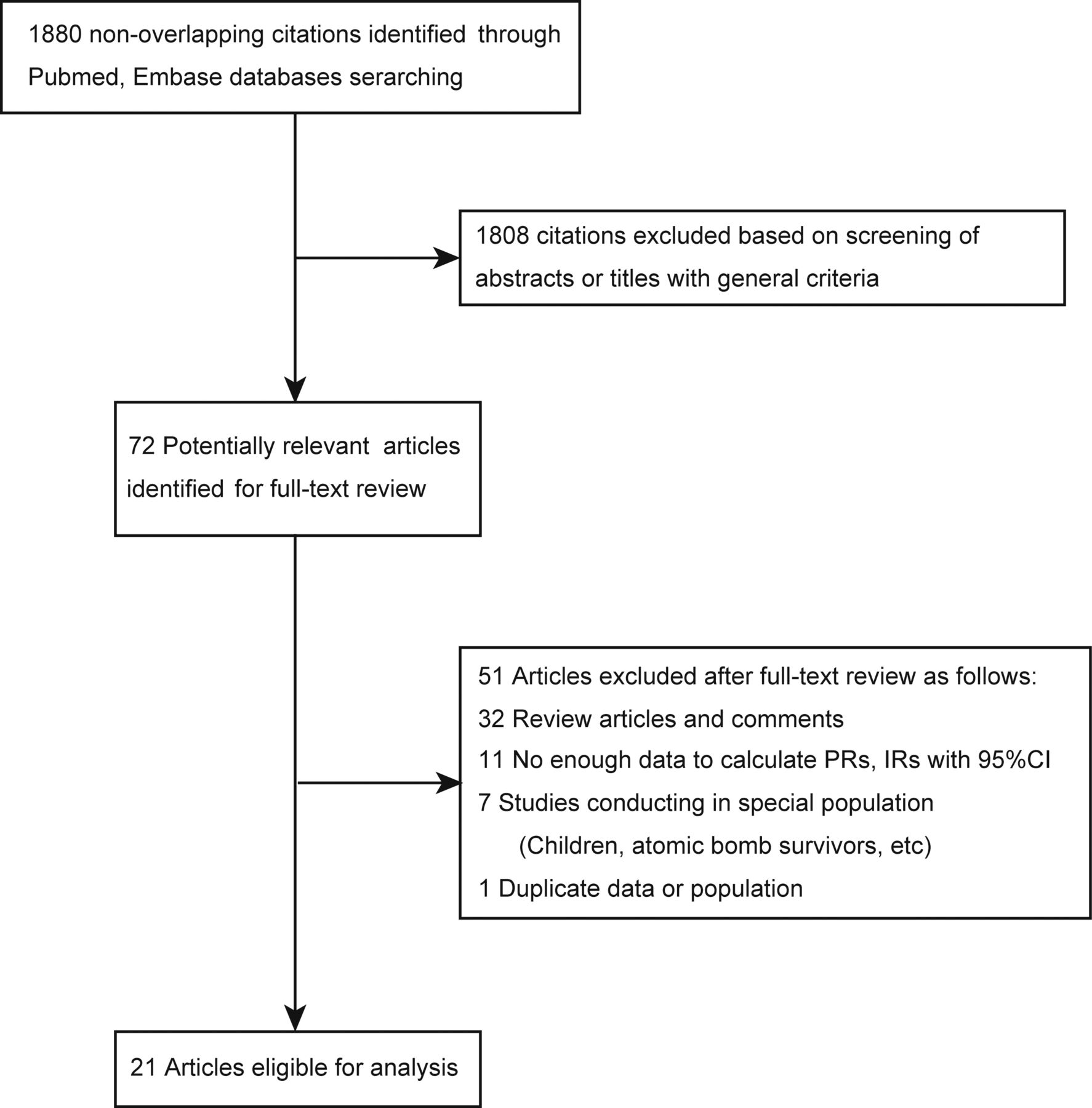
Flowchart showing article identification, inclusion and exclusion.
Characteristics of included studies
All 21 studies included were published in English between 1995 and 2013. Of included studies, 15 reported incidence or prevalence rates in European populations, 2 in America30 ,31 and 4 in Asia13 ,19 ,20 ,33 (tables 1 and 2).
Six studies discussed the IR of pSS, all of which were population-based studies and evaluated the female/male ratio.13 ,14 ,19 ,31––33 Studies varied in size from 53 to 3352 patients, and in catchment areas ranging from 1 358 994 to 55 866 666 person-years (table 1).
Summary of studies including the incidence of primary Sjogren’s syndrome
Summary of studies including the prevalence of primary Sjogren’s syndrome
Eighteen studies assessed the prevalence rate of pSS (table 2). Various sources were used for case-finding purposes. In 11 studies, pSS was identified using questionnaires and clinical examination. Other sources included physician registries and medical record databases. The method of case ascertainment varied among these studies, including International Classification of Diseases (ICD) codes, AECG criteria (2002), EC criteria (1993, 1996) and other criteria.6 ,34 ,35 Three of eleven population surveys only reported the PRs of pSS in women.21 ,24 ,26
Incidence rate of pSS
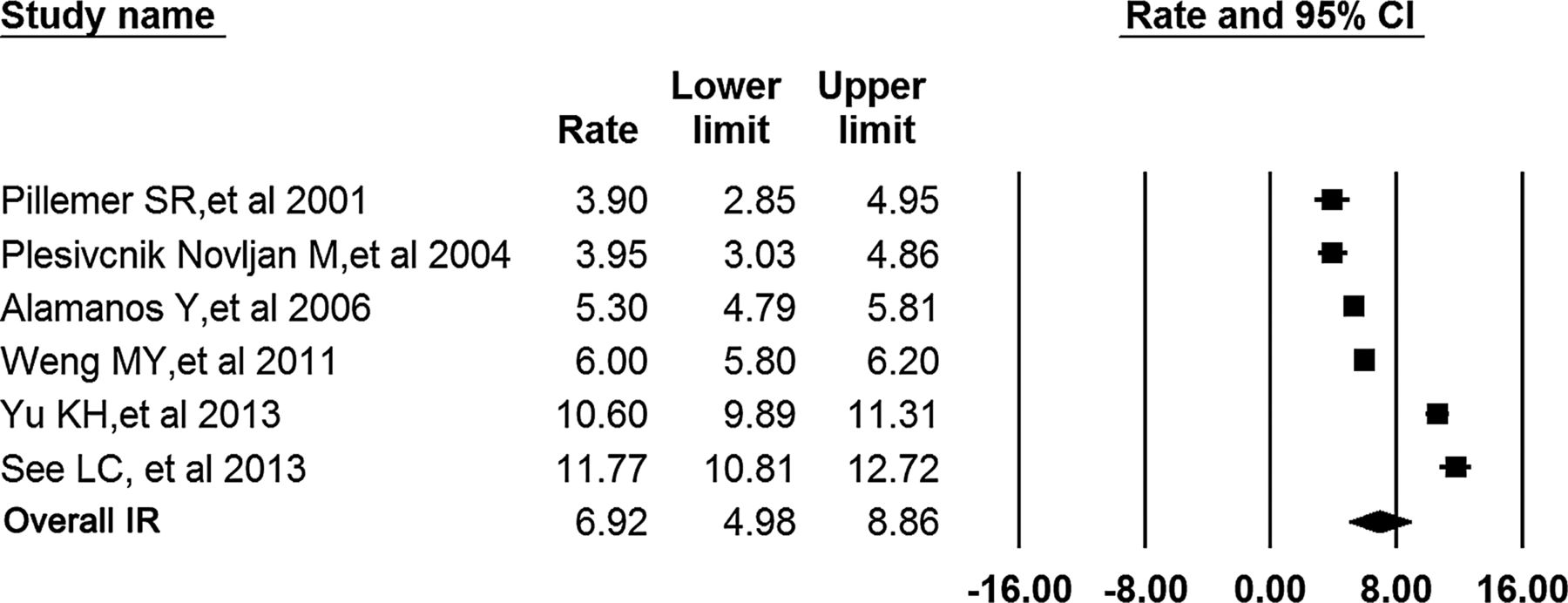
The six studies describing IRs for pSS gave an overall IR estimate of 6.92 (95% CI 4.98 to 8.86) per 100 000 person-years at risk (figure 2). Statistically significant heterogeneity was observed between studies (p<0.001, I2=98.51%). In Plesivcnik Novljan M's study, the total number of female or male patients was not reported. We analysed IRs by gender using the assumption of a 50% female background population.32 In the female population, the meta-analysis indicated that the pooled IR was 12.30 (95% CI 9.07 to 15.53). The estimated IR in the male population was 1.47 (95% CI 0.81 to 2.12) (see online supplementary figure 1). The IRR for females versus males was pooled to give an overall IRR estimate of 9.29 (95% 6.61 to 13.04) (figure 3A) The IRR based on AECG (2002) classification criteria was only discussed in Alamanos Y's study, which reported an estimate of 20.1(95% CI 12.83 to 31.49).

Overall incidence rate estimates of primary Sjögren's syndrome per 100 000 person-years at risk (meta-analysis using the random-effects model).

Rate ratios of primary Sjögren's syndrome for females versus males (a, incidence; b, prevalence; meta-analyses using the random-effects model).
Of six studies reporting IR, three were from Taiwan.13 ,19 ,33 The subgroup meta-analysis stratified by country showed that IR of pSS in Taiwan was 6.57 (95% CI 6.37 to 6.76) and had significant heterogeneity (p<0.001, I2=99.25%). In total, 6 of 21 studies reported the age of patients with pSS at diagnosis. The meta-analysis showed the pooled age at evaluation was 56.2 years (95% CI 52.5 to 59.8 years) (see online supplementary figure 2).
Three studies from Asia gave a pooled IR of 6.57 per 100 000 person-years. Two studies from Europe reported the IRs for pSS to range from 3.9 in Slovenia up to 5.3 in Greece. The prospective population-based study from the USA between 1976 and 1992 reported an IR of 3.9.
Prevalence rate of pSS
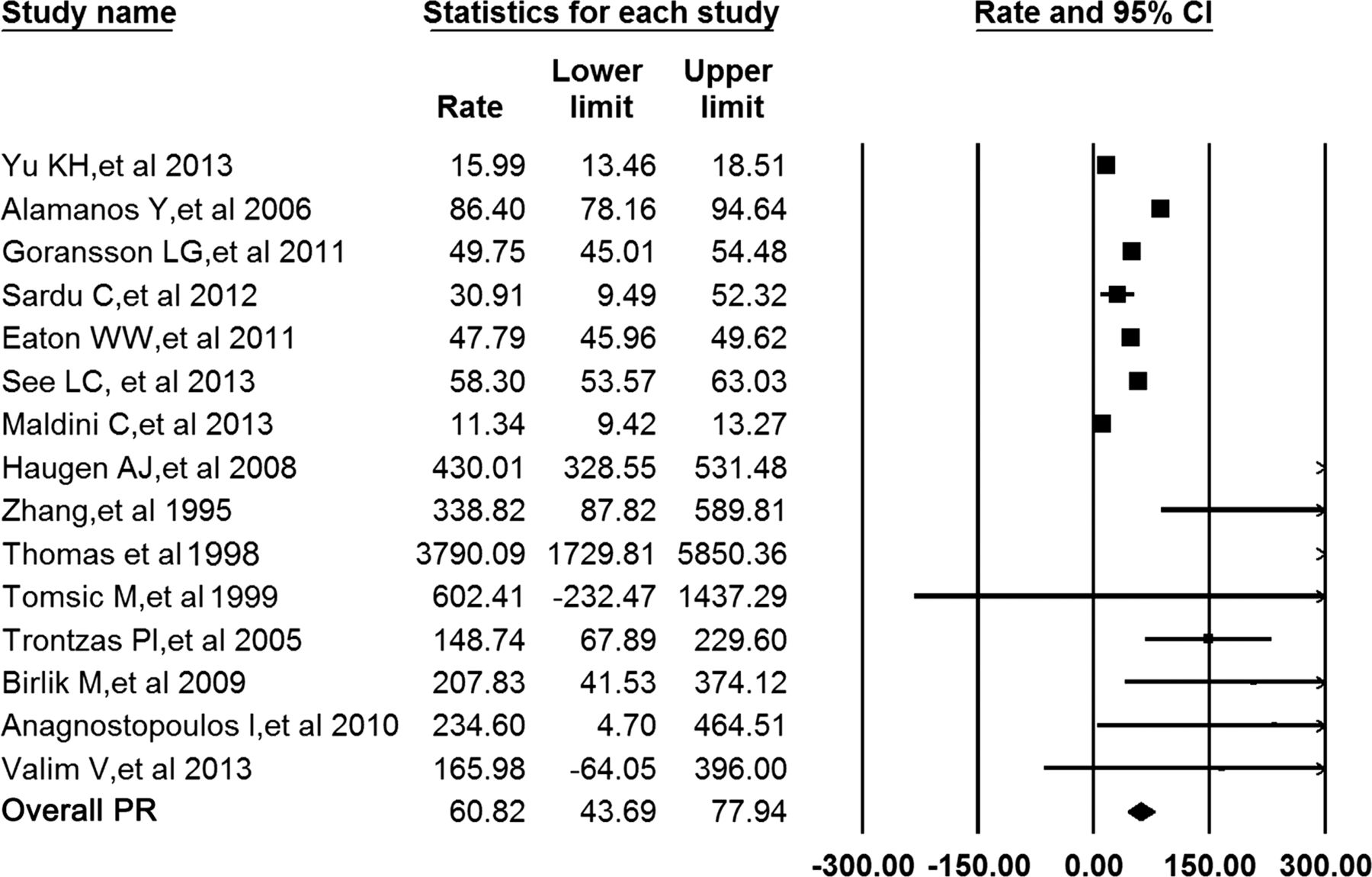
The pooled PR of pSS in the total population was 60.82 (95% CI 43.69 to 77.94) cases per 100 000 inhabitants (figure 4). Seven population-based epidemiological studies reported PRs for pSS in a defined geographical area of at least 20 000 adult inhabitants. However, the number of inhabitants in eight sample surveys reporting PR was relatively small, ranging from 332–16 046. Therefore, significant heterogeneity was observed (p<0.001, I2=98.95%). After stratifying by study design, the pooled PR across population-based studies was 43.03 (25.74 to 60.31) cases per 100 000 inhabitants. The pooled PR across studies consisting of sample surveys was 282.35 (135.32 to 429.38) cases per 100 000 inhabitants (see online supplementary figure 3). Population size significantly affected the evaluation of PR in patients with pSS. The prevalence rate reported in small studies was higher than that in larger studies. Metaregression suggest study design (p<0.001), but not sample size (p=0.136), may contribute to heterogeneity of pSS prevalence.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Pooled prevalence rate for primary Sjögren's syndrome per 100 000 inhabitants across all studies.
The estimated PR was 116.72 (95% CI 70.39 to 163.05) per 100 000 inhabitants in the female population and the pooled PR in the male population was 5.53 (95% CI 2.49 to 8.58) per 100 000 inhabitants (see online supplementary figure 4). The overall female/male ratio of patients used to calculate the prevalence of pSS (PRR) was 10.72 (95% CI 7.35 to 15.62) (figure 3B)
The 15 included studies were performed in Europe, Asia and South America. The 11 studies from Europe gave a pooled PR of 71.22 (95% CI 48.7 to 93.7) per 100 000 inhabitants. Studies from Asia had a lower pooled estimate of 44.85 (95% CI 3.51 to 86.2). Only one study was conducted in South America and had a relatively higher PR of 0.17%. The number of patients in this study was only 1205 individuals.
A subgroup meta-analysis by diagnostic criteria was conducted to evaluate the different diagnostic criteria used in these studies. The pooled PR for ICD diagnoses was 38.60 (95% CI 17.21 to 59.99) per 100 000 inhabitants. The overall estimated PR for AECG (2002) was 73.57 (95% CI 37.51 to 109.63), and the pooled female/male ratio based on those studies using AECG (2002) was 16.10 (95% CI 12.10 to 21.42) (see online supplementary figure 5). The meta-analysis for EC-1993 estimated a relatively higher PR of 929.32 (95% CI 261.01 to 1597.62).
Sensitivity analysis
The pooled IRs ranged from 5.97 (4.21 to 7.73) to 7.51 (5.35 to 9.67) per 100 000 person-years after excluding one study at a time in the sensitivity analysis. Excluding Plesivcnik Novljan M's study and evaluating only those studies that reported the total number of female and male population led to a pooled IRR of 9.15 (95% CI 3.35 to 13.18).
The overall PRs of pSS did not significantly change after one study at a time was removed (70.86 after emitting Yu's study to 51.60 after emitting Haugen's study). Four studies did not report whether they recruited secondary SS patients.17 ,18 ,22 ,23 After excluding these four studies, the pooled PR for pSS was 68.67 per 100 000 inhabitants. The four incompletely defined studies had a PR of 42.76 per 100 000 inhabitants.
Publication bias
There was no evidence of publication bias for the overall IR (Egger's test: t=0.624, p=0.566) or the overall PR (Egger's test: t=1.566, p=0.145). No significant publication bias was detected in the other meta-analyses.
Discussion
pSS is an autoimmune disease of unknown aetiology. The burden of this disease is substantial because of the lack of effective therapeutic options. pSS poses a significant burden to patient quality of life and the health are system.36 ,37 At present, few population-based epidemiological studies have investigated the prevalence and incidence of pSS.38 As a result, the epidemiology of this disease remains poorly defined. To better demonstrate this, we conducted the systematic review to comprehensively summarise the current literature on the epidemiology of pSS.
Six studies investigating the IR of pSS were population-based and of good quality.13 ,14 ,19 ,31––33 The systematic review yielded a wide range of incidence rates for pSS in Europe,14 ,32 North America31 and Asia.13 ,19 ,33 The studies from Asia reported a relatively higher IR than other regions, ranging from 6.0 to 11.8 per 100 000 person-years, and the pooled IR reached 6.57. Two studies from Europe reported the IRs for pSS to range from 3.9 to 5.3. A study from North America reported an IR of 3.9, which is the lowest IR of pSS found worldwide in the included study. Only two European studies and one North American study were included, which restricted us to conduct a meta-analysis to analyse the overall IR of pSS in these regions. Data regarding the incidence of pSS in Africa, Oceania and South America were lacking. The present study indicated that pSS occurred primarily in women with overall average age of 56.2 years at diagnosis. Three studies reported the IR for pSS in different age groups, all of which demonstrated that the incidence of pSS increased progressively with age in women, peaking at 55–65 years. In men, the occurrence of pSS mainly occurred in those aged 65 or older.14 ,31 ,33
In total, 7 of 18 studies regarding the prevalence of pSS fulfilled ‘good’ quality criteria.13 ,14 ,16––19 ,29 The other 11 studies were designed as sample surveys in which patients with pSS were initially found through questionnaires and then diagnosed using clinical examination based on established diagnostic criteria. Due to the non-population-based nature of this study and the low response rates, the prevalence was likely largely overestimated. This is also the reason why these studies were classified as of ‘moderate’ study quality. Population-based studies provide a more accurate and reliable estimate of the prevalence rate of disease. The PR of 43.03 per 100 000 is likely more representative of the true prevalence of pSS. The female/male ratio in prevalence rate for pSS is 10.72, which is higher than the female/male ratio in incidence for pSS. The reason may be that all included studies of incidence were population-based, while several studies describing prevalence were not. Both the estimated PR and PRR for AECG (2002) were relatively higher than the overall PR and PRR. Different criteria have different classification items and different diagnostic efficacy, the PRs/IRs varied among different classification criteria. It is not clear why the PR or IR in female is so much higher than male population when using AECG (2002), but it remains clear that there is no difference in sex ratio among populations of different geographical areas with different ethnic backgrounds in these studies (1.04±0.09 in all studies; 1.02±0.08 in the study using AECG (2002)). So the reason may be that the AECG (2002) classification criteria could find more female pSS cases than other criteria, but the previous study has not reported this point.
Significant heterogeneity was observed across studies exploring the prevalence of pSS. Meta-regression demonstrated that study design and diagnostic criteria contributed to the significant heterogeneity by geographic region. The great heterogeneity was still present after excluding population survey studies, suggesting the consistency of heterogeneity was not entirely due to the much larger PR estimates and the smaller overall study population in these non-population-based studies. Study design (case-finding and case-ascertainment methods) was vital for assessing the incidence and prevalence rates.
Our meta-analysis had some limitations. First, the number of studies included was relatively small, especially studies of incidence. Second, due to the lack of data provided by each study for comprehensively studying the demographics and time trends of the incidence of pSS, secondary calculations were required. Third, available studies consisted of published data. Unpublished data were not identified. This suggests that publication bias cannot be absolutely excluded even though no significant publication bias was observed. It was impossible to completely exclude the influence of confounding factors inherent in these included studies, although subgroup analyses or meta-regression by gender, region, case ascertainment and study design were performed. Other confounders such as age and study period could not be excluded. Despite these limitations, this study provides a comprehensive summary of the current literature.
In conclusion, this study evaluated the epidemiology of pSS by systematically reviewing the relevant literature. The findings also highlight the need for research on the epidemiology of pSS. Such research should employ appropriate study design and include evaluation of temporal trend in the incidence and prevalence of pSS.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online figures
Footnotes
Handling editor Tore K Kvien
BDQ, JQW and ZXY contributed equally.
Contributors BDQ and JQW were responsible for extraction and collection of data. MY and NM analyzed the data. FLH and YL wrote the paper. ZXY and RQZ mainly designed the meta-analysis.
Funding This study was supported by two grants from the China National Natural Science Foundation Council (81001333, 81072479 and 81170263).
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.