Article Text

Abstract
Objectives To search for subclinical inflammatory joint disease in patients with psoriasis without psoriatic arthritis (PsA), and to determine whether such changes are associated with the later development of PsA.
Methods Eighty-five subjects without arthritis (55 with psoriasis and 30 healthy controls) received high field MRI of the hand. MRI scans were scored for synovitis, osteitis, tenosynovitis and periarticular inflammation according to the PsAMRIS method. Patients with psoriasis additionally received complete clinical investigation, high-resolution peripheral quantitative CT for detecting erosions and enthesiophytes and were followed up for at least 1 year for the development of PsA.
Results 47% of patients with psoriasis showed at least one inflammatory lesion on MRI. Synovitis was the most prevalent inflammatory lesion (38%), while osteitis (11%), tenosynovitis (4%) and periarticular inflammation (4%) were less frequent. The mean (±SD) PsAMRIS synovitis score was 3.0±2.5 units. Enthesiophytes and bone erosions were not different between patients with psoriasis with or without inflammatory MRI changes. The risk for developing PsA was as high as 60% if patients had subclinical synovitis and symptoms related to arthralgia, but only 13% if patients had normal MRIs and did not report arthralgia.
Conclusions Prevalence of subclinical inflammatory lesions is high in patients with cutaneous psoriasis. Arthralgia in conjunction with MRI synovitis constitutes a high-risk constellation for the development of PsA.
- Psoriatic Arthritis
- Magnetic Resonance Imaging
- Synovitis
Statistics from Altmetric.com
Introduction
Psoriasis is a chronic inflammatory disease affecting 2–3% of the population.1 Between 15% and 30% of patients with psoriasis develop psoriatic arthritis (PsA), which can manifest as peripheral arthritis, enthesitis or axial disease.2 Usually musculoskeletal symptoms start after the onset of skin disease. Hence, in the majority of cases (60%) skin disease antedates arthritis.3 Development of the Classification of Psoriatic Arthritis (CASPAR) classification criteria for PsA has greatly helped to better characterise musculoskeletal involvement in patients with psoriasis, especially identifying those cases having developed clinical manifestations of inflammatory musculoskeletal disease.4
The fact that psoriatic skin disease has a higher prevalence than arthritis raises the question whether patients with psoriasis without PsA are indeed spared from joint inflammation or whether mild changes, which escape physical examination, can be found in some patients. If the latter is true, a subgroup of patients with psoriasis may be characterised by subclinical inflammation, which has been earlier recognised as ‘occult PsA’.5 Indeed, ultrasound examination of the joints has recently uncovered inflammatory lesions in patients with psoriasis.6 Hence, detecting subclinical joint inflammation could allow better understanding of the transition from skin to joint disease and therefore help to identify patients, who would benefit from more early treatment of the disease.
We recently described that patients with psoriasis without PsA exhibit enthesiophytes as the result of pathological bone formation in the joints.7 Bone formation is a pathological hallmark of PsA. The presence of similar changes in patients with psoriasis strongly supports the hypothesis of subclinical joint pathology that antedates the clinical onset of PsA. These structural lesions also highlight the well described entheseal pathology in patients with PsA.8–14 It is still unclear, however, to which extent inflammatory changes in the joints precede the onset of PsA, how such changes are related to structural pathology and whether they influence the progression of psoriasis to PsA.15
The present study was undertaken to define the prevalence and degree of inflammatory changes in the hand joints of patients with psoriasis without PsA using MRI. To explore whether inflammatory changes are related to structural changes in the joints we performed high-resolution peripheral quantitative CT (HR-pQCT). Finally we addressed whether subclinical inflammation influences the progression from psoriasis to PsA.
Methods
Patients
Patients with psoriasis (N=70) without previous diagnosis of PsA were consecutively referred from the Dermatology to the Rheumatology Clinic of the University of Erlangen-Nuremberg for detailed clinical examination for musculoskeletal disease. Fifteen patients were classified as having PsA according to CASPAR criteria at the initial investigation and were excluded from further analysis. The residual 55 patients with patients with no past or present signs of PsA received a 1.5 Tesla MRI scan as well as an HR-pQCT scan of the dominant hand. In addition, 30 healthy controls without psoriasis and with no signs of musculoskeletal disease received MRI scans of the dominant hand to evaluate the ‘background noise’ of MRI changes in healthy volunteers. The study was conducted upon approval of the local ethics committee of the University of Erlangen and with the authorisation of the National Radiation Safety Agency (Bundesamt für Strahlenschutz). Patients participated after signing informed consent.
Clinical examination
Demographic characteristics including age, sex, body mass index (BMI) and smoking status were recorded. Duration and severity (psoriasis area severity index (PASI) score) of psoriasis were documented by the dermatologist (MS).16 Furthermore, psoriasis subtype, scalp and nail involvement and the Dermatology Life Quality Index (DLQI) questionnaire were recorded.17 All patients received clinical investigation by an experienced rheumatologist (FF) for the presence of musculoskeletal disease including tender joint count (TJC) 68, swollen joint count 66, visual analogue scale (VAS) for pain and VAS for the patients global condition. All patients were additionally checked for the presence of enthesitis, dactylitis and inflammatory back pain. If signs of inflammation such as clinical synovitis (swelling), enthesitis or dactylitis were present patients were excluded. The health assessment questionnaire (HAQ) was assessed to document physical function. Furthermore, current anti-inflammatory treatment for psoriasis was documented. Inflammatory and immunological markers such as C reactive protein (CRP), rheumatoid factor and anticyclic citrullinated peptide antibodies were measured. Patients with psoriasis were followed over at least 1 year to check for the transition to PsA defined as to fulfil the CASPAR criteria.
MRI
MRI scans of the dominant hand were performed with a 1.5 T Magneton Avanto system (Siemens, Erlangen, Germany). Patients were examined in a prone position with the hand to be imaged stretched and overhead. T1-weighted axial images (voxel size 0.5×0.5×3 mm, field-of-view (FOV) 150 mm, echo time (TE): 13 ms, repetition time (TR): 766 ms, slice thickness: 3 mm) after intravenous gadolinium injection (0.2 mL/kg) were used to assess synovitis. The same T1-weighted images were assessed to evaluate tenosynovitis and periarticular inflammation along with coronal images for confirmation of the findings on a perpendicular plane. T2-weighted coronal fat saturated (turbo inversion recovery magnitude (TIRM)) sequences (voxel size 0.5×0.5×2.5 mm, FOV 220 mm, TE: 60 ms, TR: 3500 ms, slice thickness 2.5 mm) were used to assess osteitis.
MRI analysis
Image analysis focused on the metacarpophalangeal (MCP), proximal interphalangeal (PIP) and distal interphalangeal (DIP) joints of the second to fifth fingers. Synovitis and osteitis were assessed according to the Outcome Measures in Rheumatology Clinical Trials (OMERACT) pathology definitions and scored by using the PsA MRI scoring system (PsAMRIS).17 According to the scoring system for synovitis and flexor tenosynovitis the entire joint was assessed, for osteitis the proximal and distal part of each joint were evaluated separately and for periarticular inflammation volar and dorsal aspects of the entire joint were evaluated.18 We assigned a score to synovitis on a 0–3 scale, which includes absent, mild, moderate or severe thickening of the synovial membrane by thirds of the maximum potential volume of the enhancing synovium.18 Similarly the grading of osteitis on a 0–3 scale was correspondent to thirds of the assessed bone volume showing increased water content.18 Flexor tendon tenosynovitis was graded 0–3 on the basis of the thickening of the tendon sheath measured by half of the maximum thickness of the enhancing tendon sheath synovium. Periarticular inflammation was just graded as present or absent.18 The analysis was conducted per patient, all images were evaluated by two blinded and independent readers (DS, FF).
High-resolution peripheral quantitative CT
All patients underwent HR-pQCT scans of the MCP joints 2 and 3 of the dominant hand through an XtremeCT scanner (SCANCO Medical, Bruetisellen, Switzerland). Image acquisition and analysis have been described in detail elsewhere.7 Two independent and blinded readers (DS, SK) examined the HR-pQCT images for the presence and extent of enthesiophytes and erosions. Enthesiophytes, bony protrusions originating from the cortical shell and found at the insertion sites of capsule and ligaments, or at the pulleys of extensor tendons, were evaluated in number and size.7 The distance between the highest surface of the enthesiophyte and the original surface of the cortical bone was defined as the size (mm).8 ,19 Erosions, defined as breaks of the cortical shell and visible in two planes, were evaluated in their numbers and volumes.19 The volume (mm3) assessment was obtained by applying the half-ellipsoid formula as previously described.20 Erosion volume and enthesiophyte size were assessed in the largest lesion of each quadrant (target lesion). All images were analysed and measured through the open source DICOM viewer Osirix V4.1 (Rosslyn, Virginia, USA). Three-dimensional image software provided by the manufacturer was used to obtain additional images for illustrative purposes.
Statistical analysis
To analyse data we used SPSS software for statistics (IBM SPSS 21.0, IBM Corporation, Armonk, New York, USA). Continuous variables are summarised as mean±SD while categorical variables as numbers and percentages. To compare mean values between subgroups and to explore correlations, after testing for Gaussian distribution, parametrical or non-parametrical tests were applied as appropriate. Adjustments for confounding factors such as age and disease duration were applied to partial correlation analysis as appropriate. To explore associations between categorical variables, χ2 test or Fisher's test were used as appropriate. To test inter-reader reliability in defining MRI pathologies in a semiquantitative manner, Kappa coefficients were calculated to assess inter-reader reliability in detecting MRI pathologies. p Values <0.05 were regarded as statistically significant.
Results
Demographic and clinical features of the patients with psoriasis
Fifty-five patients with psoriasis (35 men and 20 women) underwent MRI and HR-pQCT imaging. Demographic and clinical characteristics of these patients are shown in table 1. Briefly, patients with psoriasis showed a mean (±SD) age of 49.0±11.4 years, and disease duration of 15.2±15.4 years. The most common psoriasis subtype was plaque psoriasis (72.7%). Nail and scalp involvement were present in 50.9% and 29.1%, respectively. Disease severity was moderate with a mean (±SD) PASI score of 6.2±8.0, moderately impacting patients’ quality of life (DLQI score: 6.3±6.1). None of the patients had signs of joint swelling, while some reported tenderness (38%; TJC 1.6±2.9), pain (57%; VAS pain 25.6±27.0) or impaired function (53%; HAQ score 0.4±0.5). CRP levels were within the normal range. Details on treatment regimens are indicated in table 1.
Demographic and disease-specific characteristics
Inflammatory MRI changes in patients with psoriasis
Prevalence of MRI inflammatory lesions in patients with cutaneous psoriasis was high. Hence, 26 out of the 55 patients (47.3%) showed at least one sign of MRI inflammation. In detail 21 (38.2%) patients showed synovitis, 6 (10.9%) osteitis, 2 (3.6%) presented with flexor tendon tenosynovitis and 2 (3.6%) periarticular inflammation (figure 1 and table 2).
Prevalence of inflammatory MRI and structural CT lesions
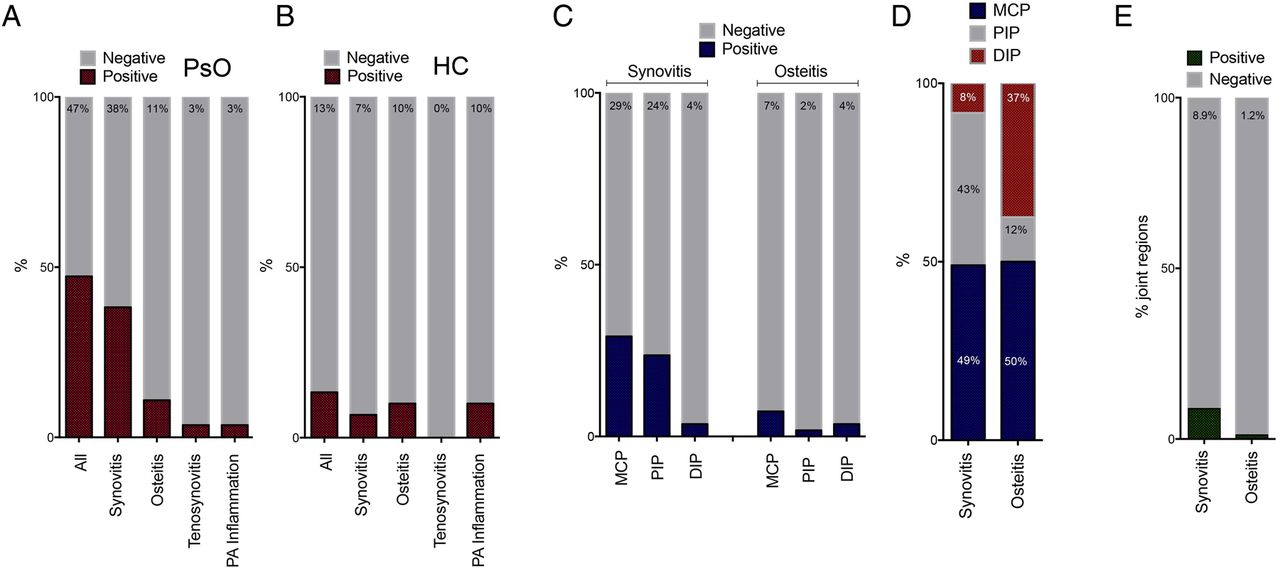
Frequency, distribution and extent of joint inflammation in patients with psoriasis. (A and B) Number of patients with psoriasis (A) and healthy controls (B) with signs of inflammatory changes in the metacarpophalangeal (MCP), proximal interphalangeal (PIP) and distal interphalangeal (DIP) joints in the MRI. (C) Number of patients with psoriasis with synovitis and osteitis in the equivalent joint regions. (D) Anatomical distribution of synovitis and osteitis, if present, in patients with psoriasis. (E) Percentage of joint regions afflicted by synovitis or osteitis of all joint regions.
Synovitis was most pronounced in the MCP and PIP joints with MCP involvement in 29.1%, PIP involvement in 23.6% and DIP involvement in 3.6% of the patients (figure 1). Signs of osteitis were detected in 7.3% of the patients in the MCP joints, 1.8% in the PIP joints and 3.6% in the DIP joints. Tenosynovitis was detected in two patients, one of them involving the flexor tendon of the fourth digit and in one the fifth digit. In both cases, thickening and effusion affected the entire tendon sheath (figure 2). Periarticular inflammation was found in the PIPs and DIPs in two patients and resembled bright appearance of the periosteal area and the periarticular soft tissues.

MRI synovitis and osteitis associated with CT erosions in patients with psoriasis. (A and B) Axial T2-weighted (left) and postcontrast T1-weighted (right) MRI of the metacarpophalangeal joints of patients with psoriasis. Dotted arrow indicates synovitis in (A), full arrow indicates tenosynovitis in (A) and osteitis in (B). (C and D) Coronal postcontrast T1-weighted MRI scans (left) showing osteitis (red arrows). Coronal high-resolution peripheral quantitative CT of the same joint region (right). Red circles indicate bone erosions. (E and F) Axial postcontrast T1-weighted MRI scans (left) showing osteitis (red arrows). Axial high-resolution peripheral quantitative CT of the same joint region (right). Red circles indicate bone erosions.
According to the PsAMRIS scoring system, the extent of synovitis in patients with MRI lesions was 3.0±2.5 units, for osteitis it was 1.8±1.0 units, for tenosynovitis 10.5±2.1 units and for periarticular inflammation 3.0±1.4 units. If present, synovitis was mild to moderate: None of the joints scored 3 (severe), while only five scored 2 (moderate) and the remaining were scored 1 (mild synovitis). Interobserver agreement for the detection of synovitis, osteitis, tenosynovitis and periarticular inflammation ranged from substantial to almost perfect. Kappa coefficient accounted for 0.91 for synovitis (p<0.001), 0.68 for osteitis (p<0.001), 0.80 for tenosynovitis (p<0.001) and 0.82 (p<0.001) for periarticular inflammation.
Comparison of MRI findings in patients with psoriasis and healthy controls
In contrast to patients with psoriasis the prevalence of inflammatory MRI changes in the healthy control group was low. Only 4 out of 30 subjects (13.3%) displayed at least one sign of inflammation. Synovitis was found in two patients (6.7%), osteitis and periarticular inflammation were each found in three patients (10.0%), while tenosynovitis was absent (table 2). Prevalence of inflammatory changes was significantly higher in patients with psoriasis than in healthy controls (χ2 (1)=9.791, p=0.002). This difference was attributable to synovitis (χ2 (1)=9.768, p=0.002), while the prevalence of osteitis, tenosynovitis and periarticular inflammation were not statistically different.
Relation of MRI inflammation to clinical and demographic characteristics
We next tested whether subclinical inflammation in patients with psoriasis is related to specific clinical characteristics. Patients presenting with inflammatory lesions (either synovitis, osteitis, tenosynovitis or periarticular inflammation) were significantly older than those without lesions (51.9±10.9 years vs 46.6±11.4 years; U=258.5, Z=−2.001, p=0.045).). Similar age differences were found in the presence or absence of synovitis (52.3±11.6 years vs 47.0±11.0 years; p=0.049). Furthermore, presence of inflammation in the MRI was associated with smoking exposure (χ2 (1)=13.13, p=0.001), while no sex differences were found. Also the extent and duration of psoriasis, the presence or absence of nail or scalp involvement and the BMI at the time of the imaging were not different between patients with or without MRI signs of inflammation.
Relation of MRI inflammation to structural bone changes
To address potential associations between inflammation and bone microstructural changes we compared inflammatory changes in the MRI to structural changes obtained by HR-pQCT. As reported previously,6 enthesiophytes were the dominant structural lesion in patients with psoriasis (table 2). While an average number of 0.5 erosions were found in patients with psoriasis (mean±SD: 0.49±0.94), the average number of enthesiophytes exceeded 5 lesions per patient (5.62±3.30). Erosions were typically localised in the metacarpal heads, while enthesiophytes were more evenly distributed among the metacarpal heads and the phalangeal bases. Patients with psoriasis with MRI inflammation did not show higher numbers (5.7±3.6 vs 5.6±3.1, p=0.86) or increased size (4.0±2.5 vs 4.0±2.0, p=0.73) of enthesiophytes compared with patients without inflammation. Furthermore, no significant correlation between enthesiophytes and the extent of MRI synovitis (r=−0.125, p=0.38) and osteitis (r=−0.072, p=0.62) was found. Similarly, no significant correlation between bone erosions and MRI synovitis (r=−0.125, p=0.39) and osteitis, (r=−0.072, p=0.62) was found.
MRI characteristics of patients with psoriasis developing PsA
Forty-one patients with psoriasis (24 men and 17 women) completed the follow-up examination after 1 year with a mean time interval between baseline and follow-up of 426±88 days. Twelve patients (29.6%) developed PsA according to the CASPAR criteria. Patients with psoriasis, which developed PsA had significantly more pain, as shown by higher VAS pain scale (17.5±20.4 vs 44.4±30.9, p=0.003) and joint tenderness (1.0±1.9 vs 4.0±4.7, p=0.008) at baseline than those not progressing to PsA (table 3). Also, the VAS global health indicated a higher disease burden (41.0±34.7 vs 16.9±17.9, p=0.007) and the HAQ a more compromised physical function (0.8±0.8 vs 0.2±0.4, p=0.007) for the patients who progressed to PsA during the follow-up. In contrast, no differences related to MRI findings were found between the groups.
Clinical and MRI characteristics of patients with psoriasis with and without progression to psoriatic arthritis
We next tested whether a combination of clinical symptoms and MRI findings can predict the progression from psoriasis to PsA. Regarding MRI data 21 out of the 41 patients showed signs of synovitis or osteitis at baseline (MRI>0). Furthermore, with respect to clinical data, 17 patients had at least one tender joint (TJC>0). Patients with psoriasis with MRI synovitis and symptoms related to arthralgia had 55.5% likelihood to develop PSA within 1 year. In contrast, only 15.3% of patients with psoriasis without signs of synovitis or arthralgia progressed to PsA (figure 3).

{kind=link}
{kind=link}
{kind=link}
Risk for development of psoriatic arthritis in subgroups of patients with psoriasis. (A) Per cent risk of developing psoriatic arthritis in subgroups of patients with psoriasis based on the presence or absence of MRI findings (synovitis and/or osteitis positive; MRI>0) or joint pain (tender joint count (TJC) of 1 or more, TJC>0). (B) Clinical characteristics of the four subgroups: TJC, visual analogue (VAS) pain scale, VAS global symptoms scale and health assessment questionnaire (HAQ). (C) MRI characteristics of the four subgroups. SY, symptoms.
Discussion
Our data show that a third of patients with cutaneous psoriasis exhibit subclinical inflammatory changes in the hand. We were surprised by the abundance of inflammatory lesions in our patient population, as we carefully excluded clinical signs of inflammatory joint disease. Hence, patients were recruited at the dermatology rather than rheumatology clinic avoiding bias towards musculoskeletal disease. Furthermore, they received detailed musculoskeletal investigation by the rheumatologist before inclusion into the study for excluding arthritis, enthesitis and dactylitis. Nonetheless, the prevalence of subclinical inflammation was high (47%) affecting significantly more individuals than healthy controls (13%) as well as compared with data in healthy individuals (27%) from recent meta-analysis.21
Few studies have yet searched for subclinical inflammation in patients with psoriasis. In an elegant ultrasound study, Naredo and colleagues showed higher prevalence of synovitis and enthesitis among patients with psoriasis compared with non-psoriatic controls.6 The absolute frequency of inflammatory changes in this ultrasound study was lower than in our MRI study, but this might be explained by differences in the techniques and by the possibility of MRI to visualise sites not accessible by ultrasound. Two previous MRI studies in patients with psoriasis addressed the prevalence of inflammatory lesions in the knee and the foot joints.22 ,23 Both studies concluded that the prevalence of inflammatory lesions is rather high in patients with psoriasis.
It is important to consider that the mere presence of inflammatory lesions in the MRI does not indicate that cutaneous psoriasis is causally linked to such lesions. In fact, neither the activity nor the duration of skin disease was associated with MRI lesions. Also, the presence of scalp involvement or nail disease, which are considered as predictors for the development of PsA24 ,25 were not associated with a higher burden of MRI inflammation. These findings suggest that skin and joint inflammation occur uncoupled and that skin disease may not represent the key pacemaker for joint inflammation. In contrast, higher age and active smoking were factors determining the presence of subclinical joint inflammation in patients with psoriasis. Smoking has recently been recognised as a risk factor for incident PsA.26
Our longitudinal analysis showed that subclinical inflammation appears to substantially influence the risk of patients with psoriasis to progress to PsA. This transition to PsA is considered being a critical step in defining the onset of musculoskeletal disease in patients with psoriasis and to shape early interventions. In our longitudinal analysis we show that both symptoms related to arthralgia as well as subclinical synovitis influence the risk for progression to PsA. Hence, more than half of the patients with concomitant presence of arthralgia as well as positive MRI changes, but only 15% of patients without such changes developed PsA. Transition of psoriasis into PsA was rather high in our study as compared with other studies,27 which may be based on accumulation of more severe cases including those with beginning joint involvement in the highly specialised care setting of an University Clinic. Nonetheless, these findings indicate the possibility to define patients with psoriasis, in which preventive treatment for the development of PsA may be feasible.28 In this context it is particularly interesting that Tinazzi and colleagues also observed high progression rates from psoriasis to PsA in patients with entheseal abnormalities in the ultrasound.29
In summary, we provide evidence for a high prevalence of subclinical inflammation in patients with psoriasis. These findings suggest that subclinical musculoskeletal disease affects a substantial proportion of patients with psoriasis. Together with arthralgia these changes predict the risk for the onset of PsA.
References
Footnotes
Handling editor Tore K Kvien
FF, DS and IO contributed equally to authorship of this paper.
MS and JR contributed equally to senior authorship.
Contributors DS, FF, IO, AK, JH, SK, AJH, RK, MS, ARC, AC collected the data. DS, FF, ME, IO, AJH, GS and JR analysed and interpreted the data. DS, FF, GS and JR prepared and revised the manuscript.
Funding This study was supported by the Deutsche Forschungsgemeinschaft (SPP1468, CRC1181), the Marie Curie project OSTEOIMMUNE, the Metarthros project of the German Ministry of Science and Education, the IMI-funded project BTCure and the Pfizer Competitive Grant Award Germany.
Competing interests None declared.
Patient consent Obtained.
Ethics approval University of Erlangen-Nuremberg.
Provenance and peer review Not commissioned; externally peer reviewed.